


Vascular
CASE 51: loWer limb ulCeration
history
A 50-year-old man presents to the vascular clinic with an ulcer on the lower aspect of the left leg. It appeared 3 months ago following minor trauma to the leg and has grown in size steadily. There is no other past medical history of note.
examination
There is an ulcer, shown in Figure 51.1, with slough and exudate at the base. There is surrounding dark pigmentation. Examination of the rest of the leg shows varicose veins in the long saphenous distribution.
Figure 51.1 venous ulceration.
Questions
•What is the definition of an ulcer?
•What are the causes of ulceration?
•What else should be included in the examination and investigation for lower limb ulceration?
•What does the management of a venous ulcer involve?
•How should the patient be managed once the ulcer has healed?
117

100 Cases in Surgery
ANSWER 51
An ulcer is the dissolution of an epithelial surface. This patient has venous ulceration. The ulcer is situated in the medial gaiter region. The edges slope and the base has healthy tissue. The surrounding skin changes support a venous aetiology.
!Causes of leg ulceration
•venous
•arterial
•mixed venous/arterial
•Diabetic: underlying aetiology neuropathic/arterial or mixture of both
•rheumatoid
•Scleroderma
•Sickle cell
•Syphilitic
•pyoderma gangrenosum
During examination, peripheral pulses should be palpated and Doppler pressures obtained. Investigations include full blood count and erythrocyte sedimentation rate, auto-antibodies (if there is a possibility of rheumatoid vasculitis) and blood glucose levels.
The mainstay of treatment for venous ulcers is calf pump compression using multi-layered bandages applied to the lower leg. The ulcer is inspected weekly to ensure that it is healing, and bandages are reapplied. An ulcer that fails to heal with these measures may benefit from surgical debridement and the application of a mesh skin graft. Malignant transformation (Marjolin’s ulcer) can develop in a long-standing, non-healing venous ulcer.
Once the ulcer has healed, the superficial and deep veins of the leg should be assessed using a duplex ultrasound scan. Saphenous vein surgery should be considered if there is evidence of sapheno-femoral or sapheno-popliteal reflux with patent deep veins. This can prevent recurrences. Patients who do not undergo surgery should wear graduated elastic support stockings to prevent recurrence.
KEY POINTS
•venous ulceration should be treated with compression bandaging.
•Caution should be taken in patients with peripheral arterial disease.
118
Vascular
CASE 52: punCheD out ulCeration
history
A 69-year-old retired plumber presents to the emergency department complaining of a painful, non-healing wound on the right lower leg. He knocked his leg on a supermarket trolley 4 weeks ago and the wound has grown in size since then. Over the past 6 months he has been getting pain in both his calves after walking approximately 10 yards. He is on medication for hypercholesterolaemia and hypertension. He had a myocardial infarction 5 years ago. He smokes 25 cigarettes each day.
examination
There is a 4 × 5 cm punched-out ulcer on the lateral aspect of the right lower leg with some surrounding erythema. In addition, there is a small ulcer between the third and fourth toe. The right foot feels cooler than the left, but capillary return is not diminished. There is a full range of movement in the right foot and sensation is intact. The femoral pulse is palpable on both sides, but no popliteal, dorsalis pedis or posterior tibial pulses are present on either side.
INVESTIGATIONS
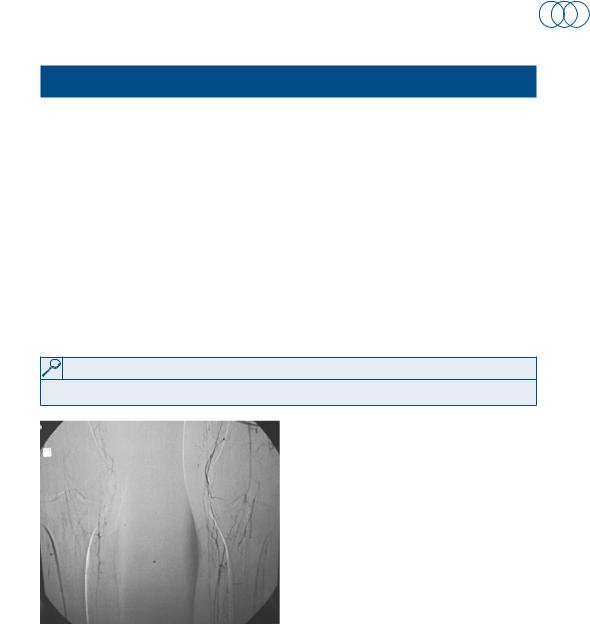
an angiogram is done and is shown in Figure 52.1.
Figure 52.1 bilateral lower limb angiogram.
Questions
•What is the likely aetiology of the ulceration?
•What does the angiogram reveal?
•What other investigations need to be carried out?
•What are the treatment options?
119
100 Cases in Surgery
ANSWER 52
The limb is ischaemic with tissue loss secondary to arterial insufficiency. The most common cause of ischaemia is atherosclerosis. This patient’s angiogram reveals that all the major vessels in both legs are occluded from the level of the popliteal artery downwards. Multiple small collaterals are seen on both sides.
The investigations should include:
•ABPI: this is related to the severity of symptoms but may be inaccurate in diabetic patients:
•1.0: normal
•0.5–0.9: claudication
•<0.4: rest pain
•<0.2: risk of limb loss
•Blood tests, including full blood count, urea and electrolytes, glucose
•Electrocardiogram
•Duplex ultrasound can be used to delineate arterial stenoses/occlusions
•Computerized tomography and magnetic resonance angiography are alternative imaging modalities
•Intra-arterial angiography and angioplasty are used to confirm and treat the lesions demonstrated on non-invasive imaging
It is important to distinguish arterial from venous ulceration, as use of compression to treat the former type of ulcer is contraindicated. Patients with tissue loss require intervention. Short, single stenoses in the vessels above the inguinal ligament are amenable to angioplasty. Below the inguinal ligament, the results are not as good and the patient may be best served by bypass surgery. Similarly, multiple stenoses, long stenoses (>10 cm) and calcified vessels are best treated with a bypass. Investigations may show that the stenoses are not suitable for either angioplasty or bypass surgery (i.e. absence of a suitable distal vessel to bypass onto), in which case a primary amputation may be the end result.
KEY POINTS
medical treatments should not be neglected. these include:
•pain control: opiate analgesia is often required
•antiplatelet agents: e.g. aspirin, clopidogrel
•lipid-lowering agents: e.g. statins
•anticoagulants: e.g. low-molecular-weight/unfractionated heparin
120