The Lower Extremity
This section is not intended as a definitive treatise on the lower extremity, but rather it is to serve as the introduction to the lower-extremity physical examination, based on the principles presented in the introductory chapters of this book. This section reviews the more salient aspects of lower-extremity structure, function, and physical examination. Its intended objective is to present the entire lower extremity as a whole. With this perspective, it is hoped that the examiner will become sensitized to the anatomical relationships that place an individual at risk of injury. Its purpose is to provide the examiner (and patient) with the means for identifying, addressing, and avoiding causes of injury.
The linkage and interdependence of articulations and structures of the lower extremity, back, and pelvis must be considered when evaluating and diagnosing complaints of the lower extremity.
The lower extremities are pillars on which the body is supported. They permit and facilitate movement of the body in space. They accomplish this task through a series of linkages: the pelvis, hip, knee, ankle, and foot. Each of these linkages has a unique shape and function. Together they permit the lower extremity to efficiently accommodate varying terrains and contours.
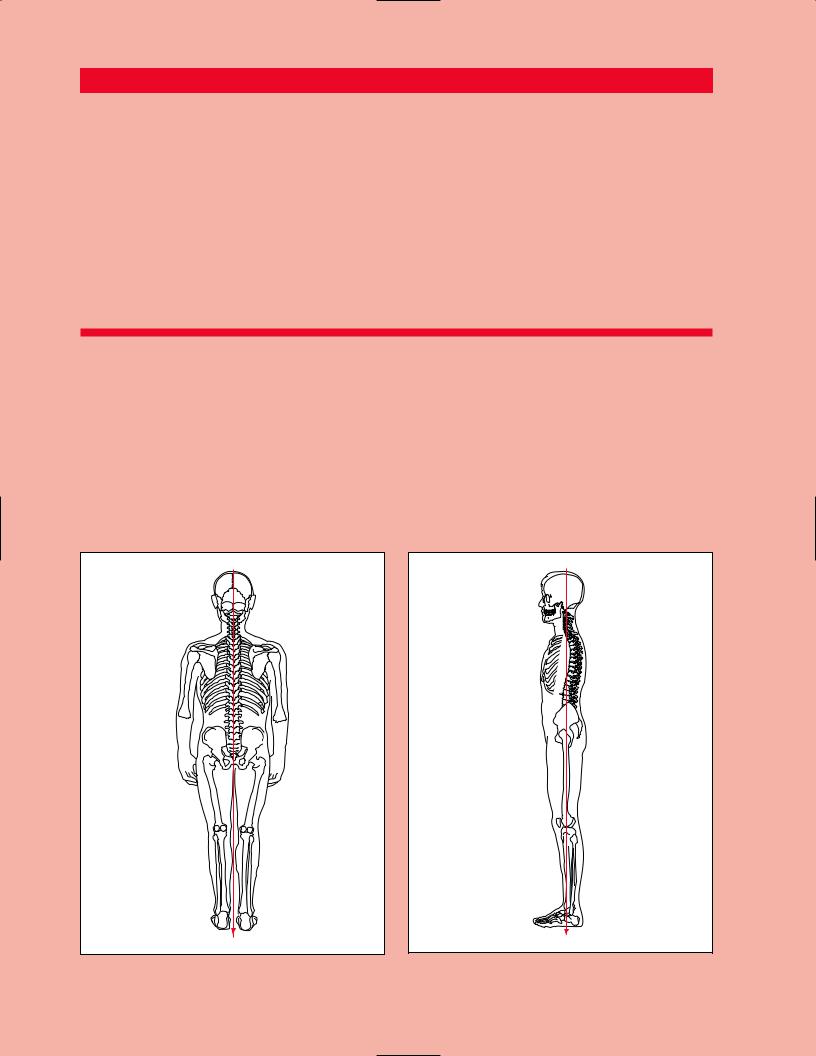
The body’s center of gravity is located in the midline, 1 cm anterior to the first sacral vertebra. During bipedal stance, the body’s weight is supported equally over each lower limb, creating a downward compression load on the joints of the lower extremities. During the unilateral support phase of gait, however, the body’s center of gravity is medial to the supporting limb. Therefore, during unilateral support, the hip, knee and ankle of the supporting limb will experience not only a compression load, but also a varus (inward) rotational destabilizing force referred to as a moment. This destabilizing force must be counteracted by a muscular effort. Otherwise, the body will fall to the unsupported side (Figure 11.1).
At the base of each pillar is the foot and ankle complex. The ankle and foot are structures uniquely designed to tolerate a lifetime of significant cyclic loads of varying rates while traversing any terrain. The key to the successful functioning of these structures lies in the extraordinary stability of the ankle, and the impact attenuation and surface accommodation properties of the foot. The stability of the ankle may well explain its ability to resist the inevitable mechanical degeneration
Tibia
Fibula
Tibial
plafond
Talus
Calcaneus
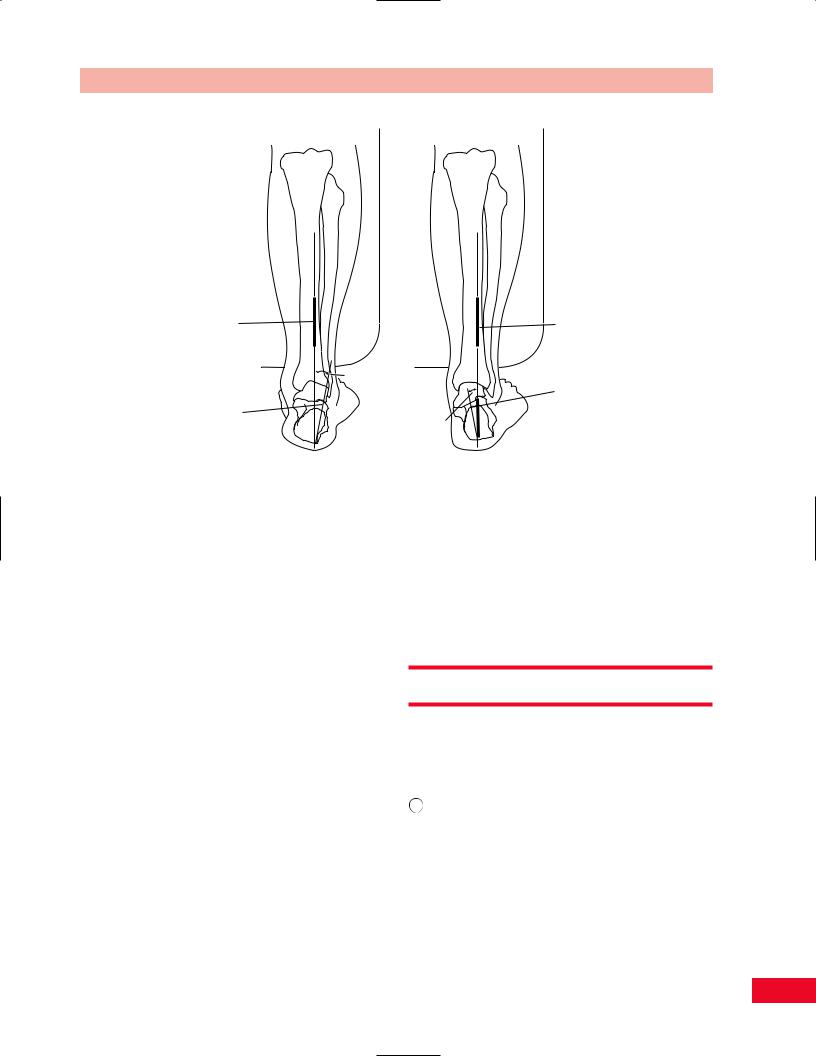
Figure 14.1 The talus is a rectangular bone keystoned within a rigid mortise formed by the medial malleolar process of the tibia, the tibial plafond, and the lateral malleolus.
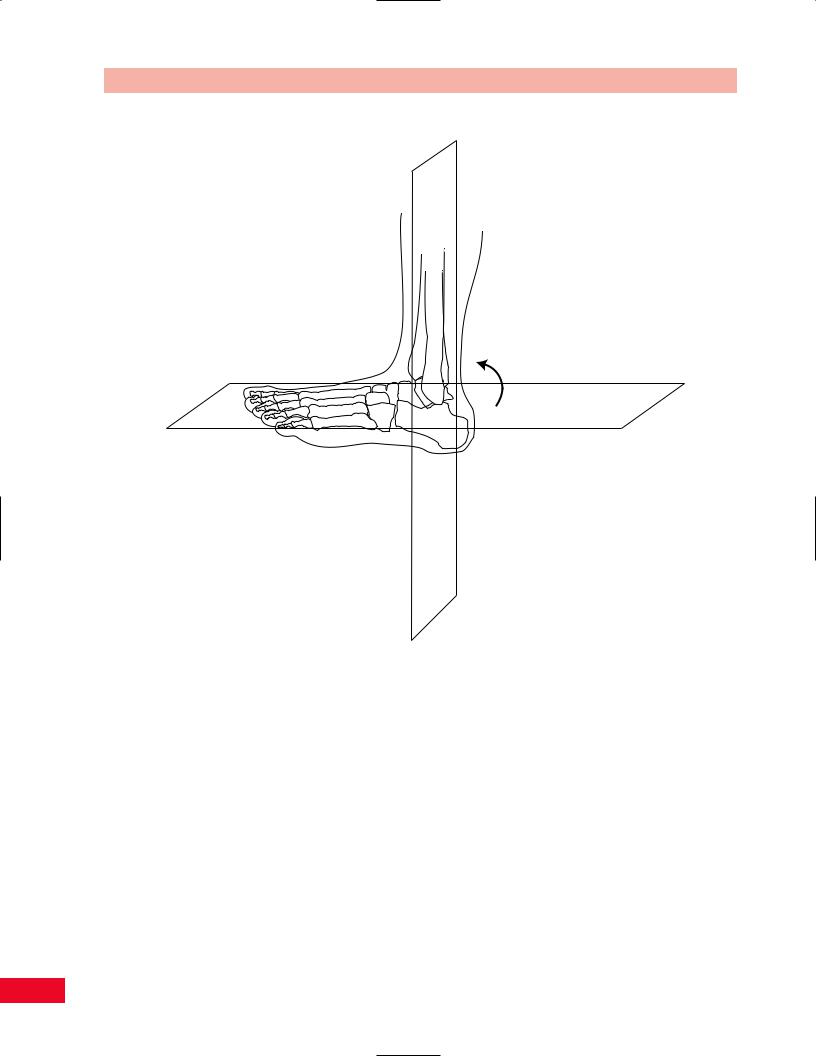
expected in such a small articulation exposed to such repetitive stress. The ankle structure is that of a keystone recessed into a rigid mortise (Figure 14.1). It is because of this extraordinary stability, unless lost secondary to injury, that the ankle does not demonstrate the normal osteoarthritic changes with aging found in all other synovial joints. This is even more impressive in light of the significant loads that are being supported by the relatively small articular surface of the ankle joint (approximately 40% that of the hip or knee) during weight-bearing activities such as running. However, this stability carries with it an inability to accommodate rotational and angular stresses that would otherwise ultimately lead to compromise of the ankle joint if they were not first buffered by the foot below. The suppleness of the foot articulations, that is, subtalar pronation, accommodates varying surface topographies to reduce these torques. The arches attenuate the repetitive stress of the weight-bearing loads that occur during locomotion. This system of complementary functions forces recognition of the ankle and foot not as isolated regions, but rather as a single ankle–foot mechanism.
The talus holds the key to the intimate structural and mechanical relationship that exists between the ankle and foot. As the part of the ankle that is held within a rigid mortise, the talus is limited to flexion– extension motion. As a part of the foot, the talus must


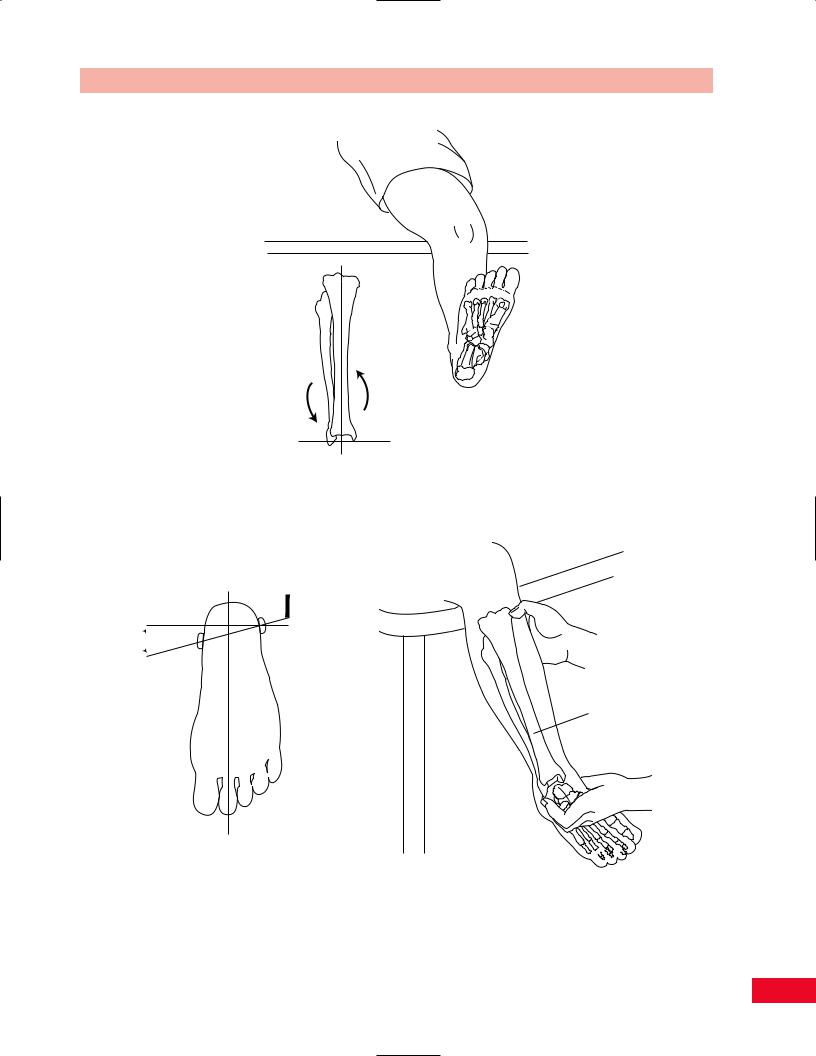
 15˚
15˚