

MusculoSkeletal Exam
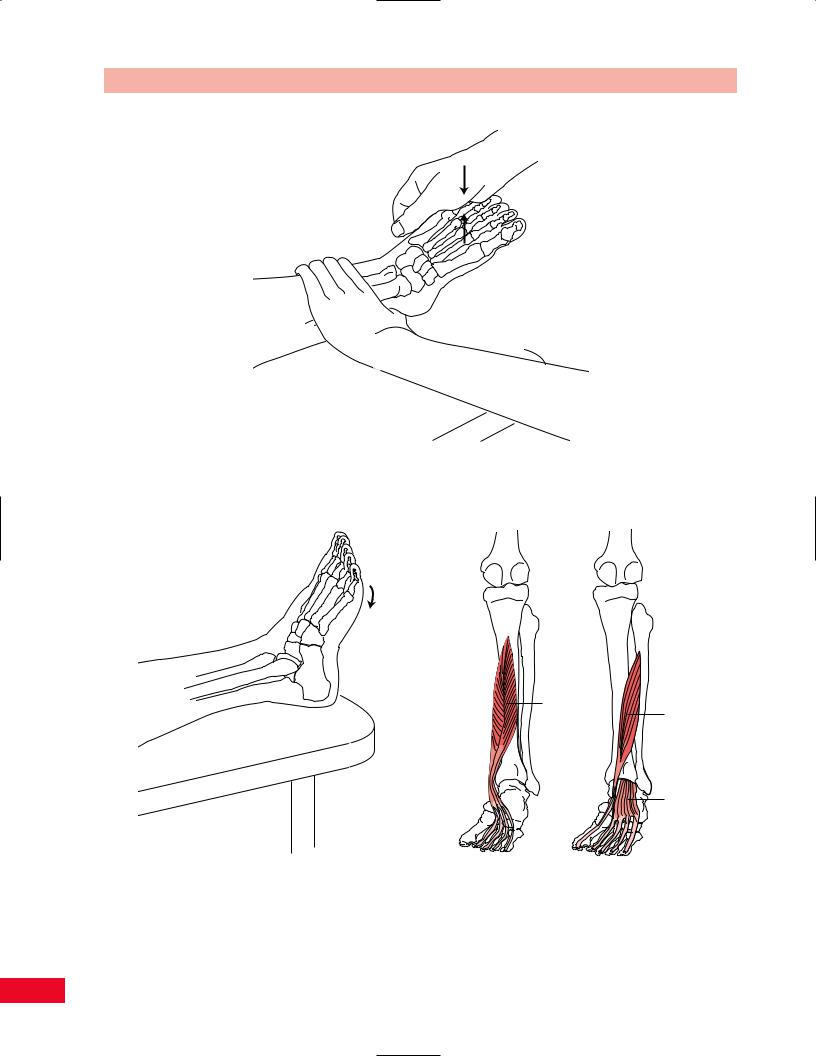
.pdfFigure 13.73 Testing subtalar inversion with gravity eliminated.
Painful resisted foot inversion can be due to a tendinitis of the tibialis posterior muscle at its attachment to the medial tibia, known as shin splints. Pain can also indicate tendinitis of the tibialis posterior or flexor hallucis longus posterior to the medial malleolus.
Subtalar Eversion
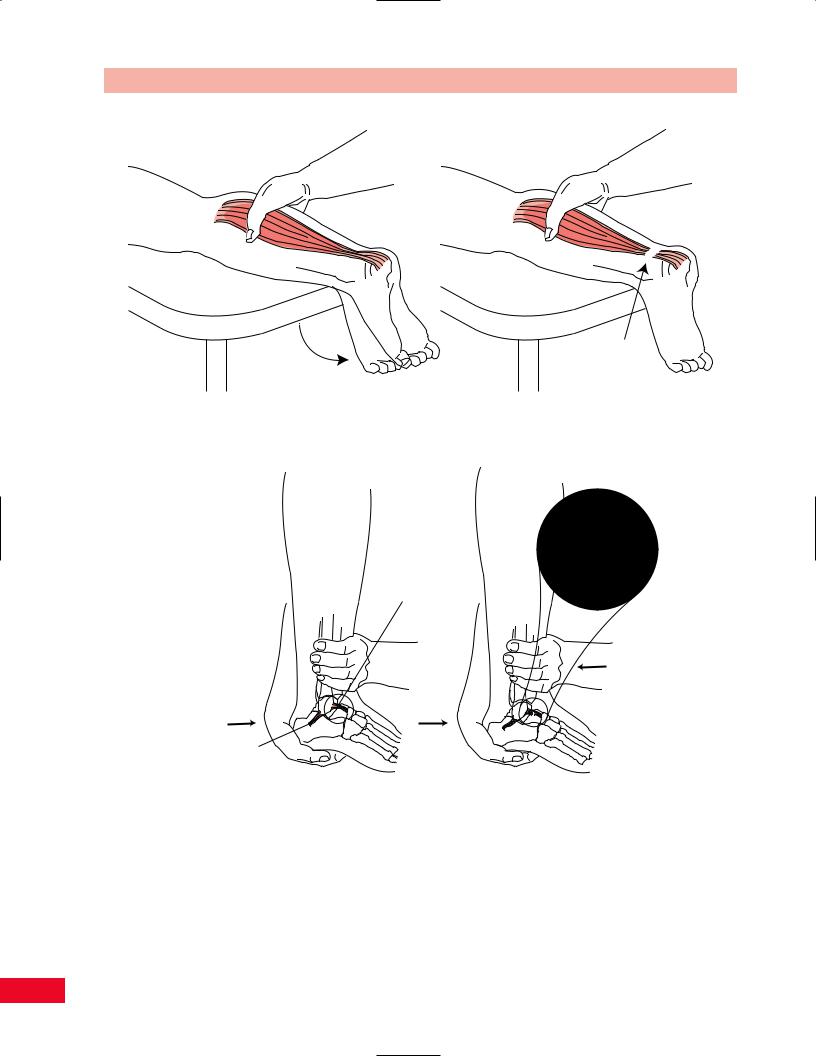
The evertors of the foot are the peroneus longus and peroneus brevis muscles (Figure 13.74). They are assisted by the extensor digitorum longus and peroneus tertius muscles.
•Position of patient: Lying on the side with the ankle in neutral position (Figure 13.75).
•Resisted test: Stabilize the lower leg of the patient with one hand. The other hand is used to apply a downward pressure on the lateral border of the foot. Ask the patient to raise the lateral border of the foot. This maneuver is more specific for the peroneus brevis.
Testing foot eversion with gravity eliminated is per-
formed by having the patient lie in the supine position and attempting to evert the foot through a normal range of motion. Observe for extension of the toes, as this signifies substitution (Figure 13.76).
Painful resisted foot eversion can be due to tendinitis of the peroneal tendons posterior to the ankle
Chapter 13 The Ankle and Foot
Peroneus longus
Peroneus brevis
Plantar view of foot
Figure 13.74 The evertors of the foot.
or at the attachment site of the muscles to the fibula. An inversion sprain of the ankle can result in stretching or tearing of the peroneal tendons and painful resisted foot eversion. A snapping sound may be heard as the tendons pass anteriorly over the lateral malleolus.
Weakness of foot eversion may result in a varus position of the foot and cause reduced stability of the lateral aspect of the ankle.
Toe Flexion
The flexors of the toes are the flexor hallucis brevis and longus and the flexor digitorum brevis and longus (Figure 13.77).
•Position of patient: Supine (Figure 13.78).
•Resisted test: Apply an upward pressure to the bottoms of the patient’s toes as he or she attempts to flex them. The flexors of the great toe may be examined separately.
Inability to flex the distal phalanx of the toes results
from dysfunction of the long flexors.
Painful resisted toe flexion may be due to tendinitis of the long flexors.
415
The Ankle and Foot Chapter 13
Figure 13.75 Testing subtalar eversion.
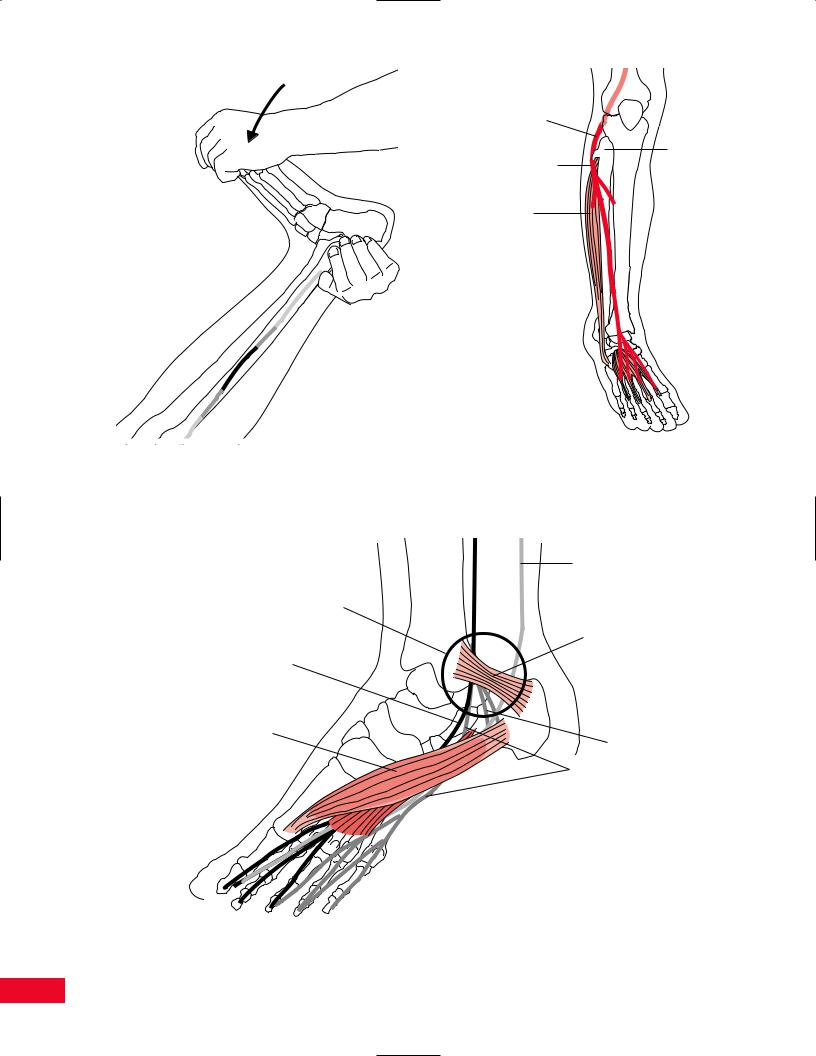
Flexor digitorum longus
Posterior view of leg
Plantar
Figure 13.76 Testing subtalar eversion with gravity eliminated. view of foot
Flexor hallucis longus
Flexor digitorum brevis
Figure 13.77 The flexors of the toes.
416

Chapter 13 The Ankle and Foot
Figure 13.78 Testing toe flexion.
Extensor digitorum longus
Extensor hallucis longus
Extensor digitorum brevis
Figure 13.79 The extensors of the toes.
Figure 13.80 Testing toe extension.
Toe Extension
The extensors of the toes are the extensor hallucis brevis and longus, and the extensor digitorum brevis and longus (Figure 13.79).
•Position of patient: Supine (Figures 13.80 and 13.81).
•Resisted test: Apply a downward pressure on the distal phalanx of the great toe, as the patient attempts to extend the toe, to test the extensor hallucis longus. Resistance can be applied to the middle phalanges of the other toes together to test the extensor digitorum longus and brevis. Weakness of toe extension may result in decreased
ability to dorsiflex the ankle and evert the foot. Walking barefoot may be unsafe, due to increased risk of falling as the toes bend under the foot.
Neurological Examination
Motor
The innervation and spinal levels of the muscles that function in the ankle and foot are listed in Table 13.1.
417

The Ankle and Foot Chapter 13
Reflexes
The ankle jerk primarily tests the S1 nerve root. It will be diminished or lost in patients with S1 radiculopathy or sciatic or tibial nerve damage. Loss of continuity of the Achilles tendon will also result in loss of an ankle jerk.
The ankle jerk is easily elicited when the patient is relaxed (Figure 13.82). Have the patient sit on the edge of the table with the knees flexed to 90 degrees. Support the ball of the patient’s foot gently upward with one hand while asking him or her to relax and try not to assist in dorsiflexion of the foot. Take the reflex hammer and gently tap the Achilles tendon to elicit a plantar flexion response at the ankle. The test can also be Eperformed with the patient prone with the feet off the edge of the table. In this position, the Achilles tendon is tapped with the reflex hammer. Always compare findings bilaterally.
Sensation
Figure 13.81 Testing great toe extension by the extensor hallucis longus.
Figure 13.82
Light touch and pinprick sensation should be examined following the motor examination. The dermatomes of the lower leg are L3, L4, L5, S1, and S2 (Figure 13.83).
Testing the ankle jerk.
418

Table 13.1 Movements of the ankle and foot: the muscles and their nerve supply, as well as their nerve root derivations, are shown.
Movement |
Muscles |
Innervation |
Root levels |
|
Plantar flexion (flexion) |
1 Gastrocnemius |
Tibial |
S1, S2 |
|
of ankle |
2 Soleus |
Tibial |
S1, S2 |
|
|
3 |
Flexor digitorum longus |
Tibial |
L5, S1, S2 |
|
4 |
Flexor hallucis longus |
Tibial |
L5, S1, S2 |
|
5 |
Peroneus longus |
Superficial peroneal |
L5, S1 |
|
6 |
Peroneus brevis |
Superficial peroneal |
L5, S1 |
|
7 |
Tibialis posterior |
Tibial |
L4, L5, S1 |
Dorsiflexion (extension) |
1 Tibialis anterior |
Deep peroneal |
L4, L5 |
|
of ankle |
2 Extensor digitorum longus |
Deep peroneal |
L4, L5, S1 |
|
|
3 |
Extensor hallucis longus |
Deep peroneal |
L5, S1 |
|
4 |
Peroneus tertius |
Deep peroneal |
L4, L5, S1 |
Inversion |
1 |
Tibialis posterior |
Tibial |
L4, L5, S1 |
|
2 |
Flexor digitorum longus |
Tibial |
L5, S1, S2 |
|
3 |
Flexor hallucis longus |
Tibial |
L5, S1, S2 |
|
4 |
Extensor hallucis longus |
Deep peroneal |
L5, S1 |
|
5 |
Tibialis anterior |
Deep peroneal |
L4, L5 |
Eversion |
1 Peroneus longus |
Superficial peroneal |
L5, S1 |
|
|
2 |
Peroneus brevis |
Superficial peroneal |
L5, S1 |
|
3 |
Extensor digitorum longus |
Deep peroneal |
L4, L5, S1 |
|
4 |
Peroneus tertius |
Deep peroneal |
L4, L5, S1 |
Flexion of toes |
1 Flexor digitorum longus |
Tibial |
L5, S1, S2 |
|
|
2 |
Flexor hallucis longus |
Tibial |
L5, S1, S2 |
|
3 |
Flexor digitorum brevis |
Tibial (medial plantar) |
L5, S1 |
|
4 |
Flexor hallucis brevis |
Tibial (medial plantar) |
L5, S1 |
|
5 |
Flexor digit minimi |
Tibial (lateral plantar) |
S1, S2 |
Extension of toes |
1 Extensor digitorum longus |
Deep peroneal |
L4, L5, S1 |
|
|
2 |
Extensor hallucis longus |
Deep peroneal |
L5, S1 |
|
3 |
Extensor digitorum brevis |
Deep peroneal |
L5, S1 |
Abduction of great toe |
1 Abductor hallucis |
Tibial (medial plantar) |
S1, S2 |
|
|
|
|
|
|
|
|
|
L5 |
|
|
|
|
|
L4 |
Dermatome |
|
|
|
|
|
|
|
|
|
|
L5 |
L4 |
|
L5 |
|
|
|
|
|
|
S1 |
|
L |
L |
|
|
|
Dermatome |
|
||
|
|
|
|
L5 |
4 |
4 |
|
|
|
|
|
|
|
|
|
|
|
|
S1 |
S1 |
|
|
|
S2 |
|
|
|
L4 Key |
|
|
|
|
L5 |
|
|
|
Dermatome |
|
|
||
|
|
|
|
|
||
sensory |
|
|
|
|
|
|
areas |
|
|
|
|
|
|
|
|
|
|
Plantar |
|
|
|
|
|
|
aspect |
|
|
S1 |
|
|
S1 |
|
|
|
|
|
S1 |
|
|
|
|
S1 Key
sensory area
L5 Key sensory area
Figure 13.83 The dermatomes of the lower leg, foot, and ankle. Note the key sensory areas for L4, L5, and S1.
419

Lateral cutaneous nerve (L5, S1)
Saphenous
nerve |
|
|
(L3, L4) |
|
Saphenous |
|
|
nerve |
Superficial |
|
(L3, L4) |
|
|
|
peroneal |
|
|
nerve |
|
|
(L4, L5, S1) |
|
|
|
|
Superficial |
|
|
peroneal |
|
|
nerve |
|
Sural |
(L4, L5, S1) |
|
|
|
Deep |
nerve |
Deep |
peroneal |
(L5, S1, S2) |
peroneal |
nerve |
|
nerve |
(L5, S2) |
|
(L5, S1) |
Figure 13.84 Anterior view of the peripheral nerves of the lower leg and foot and their distributions. 1 = saphenous nerve (L3, L4); 2 = lateral cutaneous nerve of the calf (L5, S1); 3 = superficial peroneal nerve (L4, L5, S1); 4 = deep peroneal nerve (L5, S1);
5 = sural nerve (L5, S1, S2).
Sural |
Sural |
|
communication |
nerve |
|
nerve |
(L5, S2, S2) |
|
(L5, S1, S2) |
Sciatic |
|
Lateral |
nerve |
|
(L4, L5, |
||
cutaneous |
||
S1, S2, S3) |
||
nerve |
||
|
||
(L5, S1) |
|
|
Medial cutaneous |
|
|
nerve of |
|
|
thigh |
Saphenous |
|
(L2, L3, L4) |
nerve |
|
|
(L2, L3, L4) |
|
Sural |
|
|
nerve |
|
|
(L5, S1, S2) |
|
Saphenous nerve
(L2, L3, L4)
Medial calcaneal
(S1, S2)
Medial calcaneal (S1, S2)
Figure 13.85 Posterior view of the peripheral nerves of the lower leg and foot with their distributions. 1 = saphenous nerve (L2, L3, L4); 2 = medial cutaneous nerve of the thigh (L2, L3, L4); 3 = sural nerve (L5, S1, S2); 4 = sural communication (L5, S1, S2); 5 = lateral cutaneous nerve of the calf (L5, S1; 6 = medial calcaneal branch of the tibial nerve (S1, S2); 7 = sciatic nerve (L4, L5, S1, S2, S3).
420

Chapter 13 The Ankle and Foot
Medial calcaneal branches(S1, 2)
|
Lateral plantar |
|
|
nerve (S1,2) |
|
Medial |
|
|
plantar |
Sural nerve |
|
nerve (L4,5) |
||
(L5, S1, 2) |
||
|
||
Saphenous |
|
|
nerve |
|
|
(L2, 3, 4) |
|
Figure 13.86 The nerves of the plantar surface of the foot.
Note the location of the key sensory areas for the L4, L5, and S1 dermatomes. The peripheral nerves providing the sensation to the leg and foot are shown in Figures 13.84, 13.85, and 13.86.
Referred Pain Patterns
Pain in the leg and foot may be referred from the lumbar spine, sacrum, hip, or knee (Figure 13.87).
Special Tests
Flexibility Test
Homan’s Sign
This maneuver is used to aid in the diagnosis of thrombophlebitis of the deep veins of the leg (Figure 13.88).
Figure 13.87 Pain in the leg and foot may be due to pathology in the lumbar spine, sacrum, hip, or knee.
The test is performed by passively dorsiflexing the patient’s foot with the knee extended. Pain in the calf is considered a positive Homan’s sign. Swelling, tenderness, and warmth of the lower leg are also indicative of deep vein thrombosis.
Special Neurological Tests
Peroneal Nerve Compression
The common peroneal nerve can be injured where it wraps around the head of the fibula and is close to the skin (Figure 13.89). Tinel’s sign may be elicited inferior
421
Common peroneal nerve
|
Head of |
Site of compression |
fibula |
of common peroneal |
|
nerve |
|
Peroneus |
|
longus |
|
Extensor digitorum 
 brevis
brevis
Figure 13.88 Homan’s sign is used to test for deep vein thrombophlebitis. This stretching maneuver places the deep veins of the calf on stretch.
Figure 13.89 The peroneal nerve is shown at its most common site of compression, where it wraps around the fibular head.
Posterior tibial nerve
Tarsal tunnel
Flexor retinaculum
Medial plantar nerve
Abductor hallucis
muscle
Calcaneal branches
Lateral plantar nerve
Quadratus plantae muscle
Figure 13.90 The anatomy of the tarsal tunnel. The posterior tibial nerve passes underneath the flexor retinaculum and is subject to compression at this site.
422

Chapter 13 The Ankle and Foot
Fanning
Dorsiflexion
Dorsiflexion |
|
Figure 13.91 Babinski’s response is found in patients with upper |
Figure 13.92 Oppenheim’s sign is found in patients with upper |
motor neuron disease. |
motor neuron disease. |
and lateral to the fibular head by tapping with a reflex hammer. The patient will note a tingling sensation down the lateral aspect of the leg and onto the dorsum of the foot. The patient will have a foot drop.
Tarsal Tunnel Syndrome
Entrapment of the posterior tibial nerve underneath the flexor retinaculum at the tarsal tunnel may also occur (Figure 13.90). Tinel’s sign may be obtained inferior to the medial malleolus by tapping with a reflex hammer.
Upper Motor Neuron Signs
Babinski’s response and Oppenheim’s test are used to diagnose upper motor neuron disease. Babinski’s response is obtained by scratching the foot on the plantar aspect from the heel to the upper lateral sole and across the metatarsal heads (Figure 13.91). A positive response is dorsiflexion of the great toe. Flexion of the foot, knee, and hip can occur concomitantly.
Oppenheim’s test is performed by running a knuckle or fingernail up the anterior tibial surface. A posit-
ive response is the same as for Babinski’s response (Figure 13.92).
Tests for Structural Integrity
Thompson Test for Achilles Tendon Rupture
This test is performed to confirm rupture of the Achilles tendon (Figure 13.93). The tendon often ruptures at a site 2–6 cm proximal to the calcaneus, which coincides with a critical zone of circulation. The test is performed with the patient prone and the feet dangling over the edge of the table. Squeeze the gastrocnemius muscle firmly with your hand and observe for evidence of plantar flexion. The absence of plantar flexion is a positive test result. Also observe the patient for excessive passive dorsiflexion and a palpable gap in the tendon.
Anterior Drawer Sign
This test is used to determine whether there is structural integrity of the anterior talofibular ligament, anterior joint capsule, and calcaneofibular band (Figure 13.94).
423
The Ankle and Foot Chapter 13
No foot movement when tendon
is ruptured
Figure 13.93 The Thompson test for continuity of the Achilles tendon. Absence of plantar flexion on squeezing the calf indicates a ruptured Achilles tendon (or a fused ankle joint).
Anterior talofibular ligament
Calcaneofibular ligament
Figure 13.94 Testing anterior drawer of the ankle. Excessive anterior movement of the foot indicates a tear of the anterior talofibular ligament.
The test is performed with the patient sitting with the knees flexed over the edge of the table. Stabilize the lower leg with one hand and take the calcaneus in the palm of the opposite hand. Place the ankle in 20 degrees of plantar flexion. This position makes the anterior talofibular ligament perpendicular to the lower leg. Now attempt to bring the calcaneus and
talus forward out of the ankle mortise. Excessive anterior movement of the foot, which is often accompanied by a clunk, is a positive anterior drawer sign. This test can also be performed with the patient in the supine position with the hips and knees flexed. The reliability depends in part on the ability of the patient to relax and cooperate.
424