

211
PathoPhysiology of lowEr Urinary tract obstrUction
Table 16.1. Voiding and post-micturition symptoms as defined |
suitable range, and is comparable to the typical |
|||||
by the international continence society (ics) standardisation |
voided volume on the individual’s frequency |
|||||
committee in 200217,18 |
|
volume chart, is a means by which to ascertain |
||||
Voiding symptoms |
|
that the flow rate test is representative and infor- |
||||
|
mative. Qmax is affected by VV, so nomograms |
|||||
slow stream |
the patient’s perception of |
|||||
have been developed to aid interpretation,exem- |
||||||
|
reduced urine flow, usually |
plified by the Liverpool nomograms for men |
||||
|
compared to previous |
and women22 and the Siroky nomogram for |
||||
|
performance or in |
men.23,24 At low VV, the bladder has insufficient |
||||
|
comparison with others |
|||||
|
volume to expel and Qmax may be reduced as a |
|||||
intermittent stream |
the urine flow stops and starts, |
|||||
result; nonetheless, informative conclusions can |
||||||
|
on one or more occasions, |
sometimes be drawn regardless of low VV.25 |
||||
|
during micturition |
Above 550 mL, the bladder starts to overfill and |
||||
hesitancy |
difficulty initiating micturition, |
efficiency declines,26 again causing artefactual |
||||
|
resulting in a delay in the |
reduction in Qmax. Failure of expulsion of the |
||||
|
onset of voiding after the |
entire bladder contents, leading to a PVR, signi- |
||||
|
individual is ready to pass |
fies inefficient bladder emptying; this suggests |
||||
|
urine |
either reduced bladder contractility or outlet |
||||
straining |
describes the muscular effort |
obstruction, or both. |
|
|
||
|
used to initiate, maintain, or |
|
The normal flow curve should have a rapid |
|||
|
improve the urinary stream |
upstroke, a clear Qmax, and decline quickly to |
||||
terminal dribble |
the term used to describe a |
end cleanly. Abnormal patterns include; |
||||
|
|
|
|
|||
|
prolonged final part of |
1. |
Prostatic (men): Characterized by a slow |
|||
|
micturition, when the flow |
|||||
|
|
upstroke, reduced Qmax, and prolonged down- |
||||
|
has slowed to a trickle/ |
|
||||
|
dribble |
|
stroke. |
|
|
|
Post-micturition symptoms |
2. |
Urethral stricture (men): the pattern has a |
||||
|
“plateau” appearance. |
|
|
|||
feeling of incomplete |
a self-explanatory term for a |
|
|
|
||
3. Intermittent (men or women): several peaks |
||||||
emptying |
feeling experienced by the |
|||||
|
in the flow curve can result if the patient |
|||||
|
individual after passing urine |
|
||||
|
|
strains during voiding. Likewise, a poorly |
||||
Post micturition |
involuntary loss of urine |
|
||||
|
sustained detrusor contraction causes the |
|||||
dribble |
immediately after he or she |
|
||||
|
stream to fluctuate. |
|
|
|||
|
has finished passing urine, |
|
|
|
||
|
usually after leaving the |
In men of the appropriate age group, a prostatic |
||||
|
toilet in men, or after rising |
|||||
|
pattern with a reduced Qmax |
when VV is ade- |
||||
|
from the toilet in women |
|||||
|
|
quate is suggestive of BOO but accuracy is inad- |
||||
|
|
equate by itself.27 Where Q |
max |
is above the |
||
|
|
expected range, outlet obstruction is unlikely. |
||||
is not so clear-cut,since relief of obstruction with |
However, sensitivity of flow rate testing by itself |
|||||
prostate resection surgery does not lead to reso- |
as a diagnostic test for BOO is inadequate. |
|||||
lution of storage urinary problems.21
Flow Rate and Post-void Residual
Flow rate machines measure flow volume over time and evaluate various parameters, of which the maximum flow rate (Qmax), flow pattern and post-void residual (PVR) volume are most widely used clinically. Findings have to be interpreted in the light of clinical circumstances; checking the voided volume (VV) falls into a
Voiding Cystometry
BOO is characterized by increased detrusor pressure and reduced urine flow rate.17 It is usually diagnosed by studying the synchronous values of flow rate and detrusor pressure, and is thus a urodynamic diagnosis.17
Consensus on what constitutes BOO in men has been achieved because of the relatively homogeneous nature of male BOO, reflecting

|
|
|
|
|
|
212 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Practical Urology: EssEntial PrinciPlEs and PracticE |
|
high prevalence of benign prostate enlargement |
2. An alternative nomogram has been proposed |
||||||
in older men, and the availability of transure- |
by a different group.39 |
||||||
thral resection surgery to relieve obstruction. |
3. The BOOI is applicable in men with benign |
||||||
This provided suitable circumstances to derive |
|||||||
prostate enlargement and no relevant neuro- |
|||||||
urodynamic nomograms28; the nomogram of |
|||||||
logical problem. Nonetheless, the parameters |
|||||||
Abrams and Griffiths was adopted and adapted |
|||||||
of the BOOI have been evaluated in women, |
|||||||
by the International Continence Society as a |
|||||||
such that the BOOI evaluated in conjunction |
|||||||
standardized criterion for diagnosing male |
|||||||
BOO. Thus a plot of Qmax |
against simultaneous |
with Qmax could be a usable urodynamic |
|||||
detrusor pressure (P |
Q |
) allows derivation of |
parameter of female BOO.40 A separate study |
||||
|
|
det |
max |
|
|
||
the bladder outlet obstruction index (BOOI), |
came to similar conclusions, but cut-off val- |
||||||
from which a definite diagnosis of BOO, equivo- |
ues were different.41 |
||||||
cal BOO or unobstructed can be made, as illus- |
4. An alternative compared women with ana- |
||||||
trated in Fig. 16.1. The concept superseded the |
|||||||
tomical BOO against women with stress uri- |
|||||||
earlier concept of a urethral resistance factor, |
|||||||
nary incontinence,42 with revisions using a |
|||||||
which originated from rigid tube hydrodyn- |
|||||||
amics. Since the urethra is an irregular and |
larger study group in 2000,43 and a control |
||||||
distensible conduit, whose walls and surround- |
group without stress incontinence in 2004.44 |
||||||
ings have active and passive elements which |
5. A panel of criteria derived during videouro- |
||||||
influence the flow, a resistance factor does not |
dynamic evaluation has been proposed based |
||||||
reliably provide a valid |
comparison |
between |
|||||
on study of a group of women clinically felt |
|||||||
patients.29 |
|
|
|
|
|||
|
|
|
|
to have BOO.45 |
|||
While measurements to derive a BOOI are |
|||||||
6. Area under the curve of detrusor pressure |
|||||||
generally made by invasive urodynamic testing, |
|||||||
during voiding, adjusted for voided volume, is |
|||||||
noninvasive techniques are now emerging30,31 |
|||||||
which may be able to derive an estimate of the |
a proposed parameter for diagnosing female |
||||||
detrusor pressure generating maximum flow |
BOO, though more work is needed.46 |
||||||
(i.e., with no catheter within the bladder lumen |
7. Abnormalities of free flow pattern are seen in |
||||||
to measure pressure). Penile cuff intermittent |
|||||||
a greater proportion of women subsequently |
|||||||
urethral compression32 is one approach and a |
|||||||
concluded to be obstructed on urodynamic |
|||||||
nomogram has been developed for the tech- |
|||||||
evaluation.47 |
|||||||
nique.33 Similar noninvasive pressure measure- |
|||||||
ment can be derived from a modified condom |
|
||||||
collecting device.34 Detrusor wall thickness is |
Causes of Bladder Outlet |
||||||
another parameter which may also indirectly |
|||||||
signify the presence of BOO.35,36 |
|
Obstruction |
|||||
Diagnosis of BOO in women has not been |
|||||||
standardized and remains an area of ongoing |
|
||||||
discussion.37 Proposals for urodynamic diagno- |
Male |
||||||
sis of BOO have been made as follows; |
|
The additional anatomical structure of the male |
|||||
1. Female BOO nomogram38; derived a nomo- |
|||||||
bladder outlet is the prostate gland, which |
|||||||
gram based on study of several hundred |
|||||||
encompasses the urethra between the genital |
|||||||
women defined as obstructed on clinical |
and urethral sphincters. With aging, the gland |
||||||
grounds, with quite a heterogeneous group of |
undergoes benign prostate enlargement (BPE), |
||||||
causative pathologies. The study estimated |
which can typically be shown to be a conse- |
||||||
the prevalence of female BOO at 6.5%. The |
quence of benign prostate hyperplasia (BPH); |
||||||
BPH can only be diagnosed where pathological |
|||||||
nomogram |
employs |
somewhat |
different |
||||
specimens by biopsy or resection are available.48 |
|||||||
parameters from the male BOOI, using the |
|||||||
The prevalence of BPH determined from autopsy |
|||||||
maximum |
detrusor |
pressure ascertained |
|||||
studies shows that it does not occur below the |
|||||||
during invasive urodynamics and the maxi- |
|||||||
age of 30 years and that almost 90% of men have |
|||||||
mum flow rate on free flow testing. |
|
developed BPH by their ninth decade.49 Likewise, |
|||||
213
PathoPhysiology of lowEr Urinary tract obstrUction
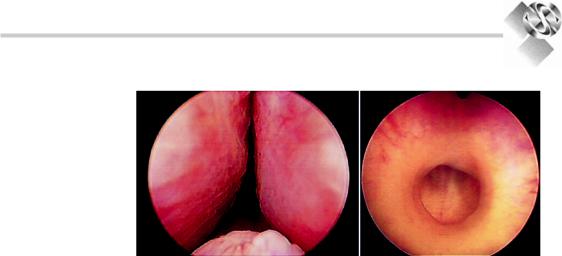
Figure 16.3. Left panel; a urethroscopic view of the intrusion of the lateral lobes and median lobe of a benignly enlarged prostate gland. Right panel; urethroscopic view of a dense fibrotic urethral stricture.
there is a steady increase in both LUTS50 and |
placebo, the alpha-blocker terazosin, the 5-alpha |
BPE,51 and all three processes are clearly inter- |
reductase inhibitor finasteride and combination |
related with ageing in men.52 |
therapy, suggested that factors other than BOO |
Implicitly, the intrusion of the prostate into |
alone almost certainly contribute to LUTS in |
the urethral lumen in BPE (Fig. 16.3) can be |
BPH. Recent studies using botulinum injections |
expected to provide a degree of anatomical |
within the prostate suggest that afferent nerve |
impedance to urine flow during voiding by |
activity may also be an element of LUTS in |
direct flow impedance, and by distortion of the |
BPE.58 Furthermore, the persistence of LUTS |
bladder outlet. Thus, flow rate does decline with |
after effective surgical management of BPE21 |
ageing in a population of men with BPE.25 The |
strongly suggests that age-related changes in |
role of anatomical impedance to flow is sup- |
bladder function contribute to male LUTS as a |
ported clinically by the response to treatment |
codependent variable alongside BPE.59 The |
aimed at reducing male sex hormones, which |
inherent difficulties of controlling for the range |
reduces the trophic factors giving rise to BPH |
of contributory variables means that the |
and thereby can partly reverse the enlargement. |
pathophysiology of male LUTS will remain a |
Within the prostate, the conversion of andro- |
source of considerable scientific debate for the |
gens to dihydrotestosterone by 5-alpha reductase |
foreseeable future. |
is a means by which this can be achieved.53 A |
Urethral strictures are another mechanism |
second contribution to BOO in BPE is the active |
giving rise to BOO in men. They comprise an |
contraction of smooth muscle in the prostate |
inelastic circumferential fibrous constriction |
stroma. The smooth muscle of the prostate |
(Fig. 16.3), and thereby differ from BPE in that |
expresses alpha-adrenergic receptors, falling |
there is not contribution of active muscle con- |
into at least two subtypes in the human pros- |
traction to the BOO. They can be present at any |
tate.54 Clinically, alpha-adrenergic antagonists |
point along the urethra; postsurgical bladder |
relax prostate smooth muscle, indicating a con- |
neck stenosis is a related situation. Strictures |
tribution of functional prostate muscle activity |
have comparatively little effect on lower urinary |
in BOO.55 On this basis, alpha-adrenergic antag- |
tract function until they cause significant con- |
onists and hormonal therapy may respectively |
striction of the lumen. Characteristically, the pat- |
decrease BOO by relaxing or shrinking the pros- |
tern of urine flow differs from that seen in BPE. |
tate. These clinical observations support the |
Strictures usually arise as a consequence of ure- |
hypothesis that there are both dynamic and |
thral trauma,which can be iatrogenic.Congenital |
static components of BOO associated with BPE. |
male urethral strictures have been described. |
The Olmstead County Study of Urinary |
Cobb’s collar is a congenital narrowing in the |
Symptoms and Health Status56 studied 2,115 |
male urethral bulb of uncertain etiology.60 |
men between 40 and 79 years of age and showed |
BPE and urethra stricture are by far the most |
that the severity of LUTS, peak flow rate, and |
common causes of BOO in men. Rare causes of |
extent of prostate enlargement were all age- |
obstruction in men include congenital urethral |
dependent and interrelated. However, the |
abnormalities,61,62 foreign bodies,63 uretero- |
Veterans Affairs Cooperative Study57 comparing |
coele,64 adult onset voiding dysfunction.65 |

214
Practical Urology: EssEntial PrinciPlEs and PracticE
Female |
|
|
|
2. |
BOO caused by stress incontinence surgery is |
|||||||
In women, several factors can contribute to BOO |
|
symptomatic of |
the conflicting roles of the |
|||||||||
|
lower urinary tract in being responsible both |
|||||||||||
(Table 16.2), which consequently represents a |
|
|||||||||||
|
for urinary storage and intermittent expulsion |
|||||||||||
more diverse |
situation |
pathophysiologically |
|
|||||||||
|
of the urine. In women with incontinence, the |
|||||||||||
than is the case in men. As discussed above, |
|
|||||||||||
|
need to improve urine storage surgically car- |
|||||||||||
this renders formal standardized diagnosis |
|
|||||||||||
|
ries an implicit risk that voiding may be |
|||||||||||
problematic. |
|
|
|
|
||||||||
1. Pelvic Organ Prolapse (POP). Deficiency of |
|
impaired.For most women,voiding function is |
||||||||||
|
satisfactorily preserved, but a minority do suf- |
|||||||||||
ligamentous support of the pelvic floor and |
|
|||||||||||
|
fer impaired voiding, taking the form of void- |
|||||||||||
weakness of the musculature results in pro- |
|
|||||||||||
|
ing symptoms, an increased post-void residual |
|||||||||||
lapse of pelvic and abdominal organs. Where |
|
|||||||||||
|
or acute urinary retention. This is recognized |
|||||||||||
the anterior vaginal compartment is affected, |
|
|||||||||||
|
for the main surgical options available, includ- |
|||||||||||
the altered configuration may distort the ure- |
|
|||||||||||
|
ing midurethral slings,74 other forms of sling75 |
|||||||||||
thra, which can impair voiding.Where middle |
|
and colposuspension,76 along with techniques |
||||||||||
compartment prolapse to the level of the vag- |
|
no longer in general use such as the Stamey |
||||||||||
inal introitus is present, a direct compression |
|
|||||||||||
|
procedure77 and bone-anchored slings.78 |
|
||||||||||
effect on the urethra could also |
occur. |
3. |
Functional causes; the lower urinary |
tract |
||||||||
Obstructive voiding, LUTS, in general, and |
||||||||||||
|
musculature and the range of CNS structures |
|||||||||||
occult stress incontinence can all coexist.72 |
|
|||||||||||
|
contributing |
to |
their regulation requires |
|||||||||
Some women with prolapse find that voiding |
|
|||||||||||
|
coordinated activity to achieve normal func- |
|||||||||||
is impeded during the daytime, as a conse- |
|
|||||||||||
|
tion. Some women manifest voiding abnor- |
|||||||||||
quence of upright posture, and complain of |
|
|||||||||||
|
malities, |
which |
appear |
to |
derive |
from |
||||||
incontinence |
overnight, when the |
supine |
|
|||||||||
|
excessive |
activity, failure |
of |
relaxation, or |
||||||||
position reduces the |
prolapse. The |
precise |
|
|||||||||
|
impaired coordination of some of these com- |
|||||||||||
effect can be hard to evaluate urodynami- |
|
|||||||||||
|
plex components. In part, this can derive |
|||||||||||
cally,73 since effects on voiding are dependent |
|
|||||||||||
|
from failure to acquire normal toileting hab- |
|||||||||||
on the patient’s position, which will affect the |
|
|||||||||||
|
its in childhood, or acquired in adulthood,65 |
|||||||||||
anatomical relationship between the abnor- |
|
leading |
to |
dysfunctional |
voiding79 |
and |
||||||
mally mobile structures and markedly influ- |
|
“pseudo-dyssynergia.” Fowler’s syndrome is |
||||||||||
ence their function. |
|
|
|
|||||||||
|
|
|
an acute onset condition arising in adult |
|||||||||
|
|
|
|
|
||||||||
|
|
|
|
|
women, characterized by painless retention, |
|||||||
Table 16.2. causes of female bladder outlet obstruction |
|
and diagnosed by high urethral closure pres- |
||||||||||
|
sures and abnormal urethral sphincter EMG |
|||||||||||
Anatomical |
|
Functional |
|
|
||||||||
|
|
|
activity 80 (Fig. 16.4). |
|
|
|
||||||
|
|
|
|
|
|
|
|
|||||
gynecological; pelvic organ |
bladder neck obstruction |
prolapse, fibroids, lichen |
|
sclerosus66 |
|
Postsurgical |
Pseudodyssynergia |
Urethral abnormalities, |
fowler’s syndrome |
such as diverticulum,67 |
|
stenosis68 |
|
Mass lesions such as |
|
uterine fibroids,69 other |
|
intra-abdominal |
|
lesions70 |
|
Ureterocoele71 |
|
Neurourology
Impaired voiding function is common in patients with neurological disease, resulting from reduced bladder contractility (Fig. 16.4), BOO, or both. In lower motor neurone neurological lesions, BOO can be a consequence of pelvic floor denervation, leading to pelvic organ prolapse and urethral distortion. For upper motor neurone neurological lesions, the problem is one of failure of the urethral sphincter to relax appropriately at the time of voiding. This can