485
Urinary tract FistUla
urography, or MR urography. Retrograde pyelo- |
successful in small fistulas only,less than 2–3 mm |
|||
grams may be utilized if the distal ureter is not |
in diameter. |
|
||
well visualized, and a concomitant ureterovagi- |
|
|
||
nal fistula is suspected but has not been demon- |
Surgical Management |
Once the decision has been |
||
strated on alterative upper urinary-tract |
||||
imaging.1,11 Delayed visualization of contrast |
made by the patient and physician to pursue |
|||
within the vagina on CT urogram or direct con- |
definitive surgical repair, it is essential to |
|||
trast extravasation into the fistula tract on CT |
carefully plan an operative approach that will |
|||
cystogram provide alternate means of evalua- |
maximize the chance of success.The first attempt |
|||
tion, with the added ability to detect additional |
at VVF repair is usually the best opportunity for |
|||
intra-abdominal pathology.23 |
fistula closure, due to later scarring and |
|||
|
|
anatomical distortion. There is no “best” |
||
|
|
approach for VVF repair as long as the basic |
||
Treatment |
|
principles are followed. |
||
The goal of treatment of VVF should be the |
Classic teaching suggests a minimal waiting |
|||
period of several months after diagnosis for |
||||
timely and complete cessation of urinary leak- |
||||
definitive repair; however, delayed management |
||||
age with minimal effect on normal urinary and |
||||
has fallen out of favor over the past few decades. |
||||
genital function. |
|
|||
|
Immediate management, especially in cases of |
|||
|
|
|||
|
|
uncomplicated iatrogenic fistula, can minimize |
||
Conservative Management |
Conservative management |
patient discomfort and anguish without com- |
||
of small VVF can be attempted prior to surgical |
promising the surgical repair.11,27-33 However, in |
|||
intervention. Although there is some morbidity |
cases of continued infection, obstetric fistula, |
|||
and discomfort associated with indwelling |
or radiation-induced fistula, demarcation of |
|||
catheterization, a trial of continuous bladder |
inflamed or devascularized tissues may require |
|||
drainage and anticholinergic medication for |
a waiting period of 1–6 months and 6–12 months, |
|||
2–3 weeks can be associated with spontaneous |
respectively.18,34,35 Medical factors and wound |
|||
healing in properly selected patients.24 Small |
care also should be addressed and optimized |
|||
epithelializedfistulasmaybenefitfromminimally |
prior to intervention in these and all other fis- |
|||
invasive cystoscopic electrocoagulation of the |
tula cases. |
|
||
fistula tract, followed by bladder catheterization. |
Vesicovaginal |
fistula can be repaired via |
||
In patients with |
fistula diameter less than |
a transvaginal or transabdominal approach. |
||
3.5 mm,11/15 had successful fistula tract ablation |
Each approach has benefits and drawbacks, |
|||
with cauterization and catheter drainage in a |
but each results in traditionally high rates of |
|||
study by Stovsky et al.25 Fibrin sealant has also |
successful fistula closure, usually greater than |
|||
been utilized with some success to plug the |
90% (Table 35.3).7,36-38 Consideration of fac- |
|||
fistula tract, presumably until tissue ingrowth |
tors such as size, location, and need for adjunc- |
|||
occurs.26 In general, conservative measures are |
tive procedures can affect the approach, but |
|||
Table 35.3. surgical management of vesicovaginal fistula. comparison of transabdominal and transvaginal approaches to repair
Approach |
Transabdominal |
Transvaginal |
timing |
delayed (3–6 month) |
immediate/delayed |
Ureteral involvement |
reimplant possible if indicated |
no reimplant possible |
sexual function |
no change in vaginal depth |
risk of vaginal shortening |
Flaps |
omental, peritoneal |
labial, peritoneal, gluteal, gracilis |
indications |
large fistula, high fistula in narrow vault, radiation, failed |
low fistulas, failed taFr |
|
vaginal approach, other procedures (augment) |
|
Morbidity |
High |
low |

|
|
486 |
|
|
|
|
|
Practical Urology: EssEntial PrinciPlEs and PracticE |
the most important factor should be surgeon |
throughout the case. Ureteral stents are placed |
|
experience and comfort. Surgical mobilization |
if the fistula is in close proximity to the ureteral |
|
of well-vascularized flaps, followed by a sepa- |
orifices. A urethral catheter is placed, and a |
|
rate water-tight closure of the urinary and |
supra-pubic catheter may also be utilized for |
|
genital tracts with nonoverlapping suture lines |
bladder drainage. An inverted U-shaped inci- |
|
is the intraoperative goal regardless of the |
sion is made which circumscribes the fistula |
|
approach. |
site. Anterior and posterior vaginal wall flaps |
|
Transabdominal approaches for fistula repair |
are developed after hydro-dissection with ster- |
|
include supravesical or transvesical approaches, |
ile saline, and retracted using the ring retractor. |
|
and laparoscopic/robotic techniques. The |
Using double-armed SAS, the fistula is closed in |
|
O’Conor transabdominal VVF repair has been |
an interrupted fashion. The perivesical tissue is |
|
well described.39 The patient is positioned in a |
then closed over the initial suture line in an |
|
low lithotomy position, with access to the vagina |
interrupted imbricated fashion, 90° in respect |
|
and abdomen. Ureteral catheters may be placed |
to the first layer. A peritoneal flap or a martius |
|
and are recommended if the fistula is near the |
flap can be positioned over the imbricated layer |
|
ureteral orifices or the trigone. A lower midline |
of peri-vesical tissue. The posterior vaginal wall |
|
incision is performed and the bladder is mobi- |
flap is advanced over the suture line anteriorly |
|
lized. The bladder is then bivalved vertically to |
to complete the closure. |
|
the level of the fistula, and dissection is contin- |
Adjacent tissue flaps can be useful in the |
|
ued distally to open the vesicovaginal space, |
setting of complex fistula with compromised |
|
2–3 cm distal to the fistula site. Following mobi- |
surrounding tissue, or in patients with prior |
|
lization of the vaginal wall from the bladder wall |
failed repairs, radiotherapy, obstetric fistula, or |
|
distal to the fistula tract, the fistula tract is |
large fistula tracts. For patients undergoing a |
|
excised, and the vaginal wall is closed with run- |
transvaginal approach, a labial fat pad (Martius) |
|
ning synthetic absorbable suture (SAS). The |
or peritoneal flaps are most frequently utilized |
|
bladder is closed in multiple layers with running |
with success rates of greater than 90%.7 The |
|
SAS. An additional layer of tissue can be placed |
Martius graft is harvested from the fibrofatty |
|
between the suture lines utilizing an omental |
tissue of the labia majora. It maintains blood |
|
interposition flap or peritoneal flap. It is impor- |
supply from the external pudendal artery supe- |
|
tant to secure the interpositional flap distally |
riorly and the inferior labial artery inferiorly, |
|
beyond the fistula. |
allowing rotation and mobilization from either |
|
In the transvesical approach, the bladder is |
pedicle. Once mobilized via a labial incision, this |
|
opened via a midline cystotomy on the anterior |
flap can be tunneled into the vaginal dissection |
|
surface of the bladder. The VVF tract is then cir- |
for additional layers of fistula closure. In high |
|
cumscribed and excised.Following mobilization |
VVF repairs from a transvaginal approach, the |
|
of the vesicovaginal space surrounding the fis- |
peritoneum is often encountered during the |
|
tula site, the vaginal and vesical tissues are |
course of dissection. The peritoneum can be |
|
closed separately. A flap of adjacent bladder tis- |
advanced over the fistula repair as an additional |
|
sue may be advanced to avoid overlapping suture |
layer of closure, with success rates of 91–96%.7,41 |
|
lines as described by Gil-Vernet.40 |
As noted previously, omental interposition flaps |
|
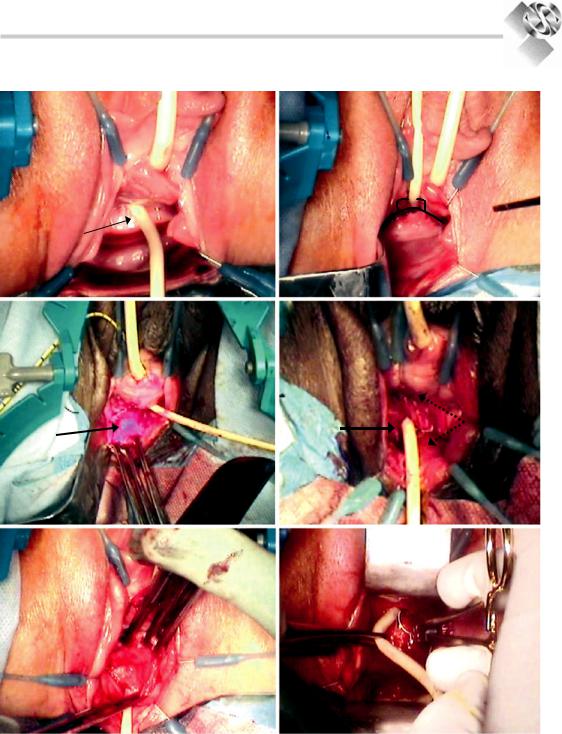
The transvaginal approach for fistula repair |
are useful adjunctive procedures when perform- |
|
is shown in Fig. 35.3.7,41,42 The patient is placed |
ing transabdominal VVF repairs in the manner |
|
in the dorsal lithotomy position, and a rectal |
of O’Conor. Interposition flaps or peritoneal |
|
pack is placed. Labial retraction sutures are |
flaps can be incorporated into transabdominal |
|
placed as well as a weighted speculum. A self- |
fistula repairs between bladder and vaginal wall |
|
retaining ring retractor with hooks is very use- |
suture lines. The omental vascular supply is |
|
ful for visualization and retraction. Cystoscopy |
based on the right and left gastroepiploic arter- |
|
is performed to localize the fistula tract, and a |
ies. In order to provide sufficient length for the |
|
guide wire is placed though the fistula into the |
flap to reach the pelvis, the omentum can be |
|
vagina. A 10–12 French foley catheter should be |
mobilized along the greater curvature of the |
|
placed though the fistula site, using the previ- |
stomach, sacrificing the left gastroepiploic |
|
ously placed guide wire. This catheter provides |
artery and allowing larger right gastroepiploic |
|
traction of the fistula toward the introitus |
artery to maintain blood supply. |
|