


93
PrinciPlEs of BactErial Urinary tract infEctions and antimicroBials
Epidemiological Breakpoints
The epidemiological breakpoints are categorized into wild-type and non-wild-type microorganisms by applying the appropriate cut-off value in a defined phenotypic test system. Wild-type and non-wild type microorganisms may or may not respond clinically to antimicrobial treatment. These cut-off values will not be altered by changing circumstances.
•Wild-type: A microorganism is defined as wildtype for a species by the absence of acquired and mutational resistance mechanisms to the drug in question.
•Microbiological resistance-non-wild type: A microorganism is defined as non-wild type for a species by the presence of an acquired or mutational resistance mechanism to the drug in question.
Clinical Breakpoints
The clinical breakpoints are categorized into susceptible,intermediate,and resistant by applying the appropriate breakpoint in a defined phenotypic test system. These clinical breakpoints may be altered with legitimate changes in circumstances, such as new pharmacological data on antimicrobial substances.
•Clinically susceptible (S): A microorganism is defined as susceptible by a level of antimicrobial activity associated with a high likelihood of therapeutic success.
•Clinically intermediate (I): A microorganism is defined as intermediate by a level of antimicrobial agent activity associated with uncertain therapeutic effect. It implies that an infection due to the isolate may be appropriately treated in body sites where the drugs are physically concentrated or when a high dosage of drug can be used; it also indicates a buffer zone that should prevent small, uncontrolled, technical factors from causing major discrepancies in interpretations.
•Clinically resistant (R): A microorganism is defined as resistant by a level of antimicrobial activity associated with a high likelihood of therapeutic failure.
The establishment of clinical breakpoints implies the assessment of pharmacodynamic and pharmacokinetic parameters.
Pharmacodynamic Parameters
Pharmacodynamic parameters are those that describe the action of an antimicrobial at the bacterial cell. Several laboratory tests have been implemented to assess phenotypical pharmacodynamic parameters in vitro and thus predict the effectiveness of an antimicrobial therapy in vivo.
The primary aim of laboratory testing with antimicrobials is to predict therapeutic success in the individual patient treated. The most frequently used tests were designed to quantitate the lowest concentration of an antimicrobial that inhibits visible in vitro growth of the microbe, which is called the minimal inhibitory concentration (MIC). The MIC can be assessed by different tests, the most frequently used tests are the brothand agar dilution tests. The disk diffusion procedure is a simplified method to approximate the MIC. The MIC is a parameter defined to predict therapeutic success, at least in an immunocompetent environment. The factors that determine the outcome of an infection are, however, complex and incompletely addressed by in vitro tests. A variety of factors can influence the efficacy of antimicrobials in vivo: Aminoglycosides or fluoroquinolones lose their activity in acidic pH as frequently found in urine or at sites of purulent infection. The concentrations of certain cations, such as Ca2+ or Mg2+, which is extensively varying in urine, also influence the activity of aminoglycosides or fluoroquinolones in UTI. The MIC has therefore to be interpreted with caution.
Theminimalbactericidalconcentration(MBC) is defined as the lowest concentration of an antimicrobial that kills 99.9% of the inoculum. This test is not used in clinical routine with the exception of certain questions, such as treatment of infections in compartments deprived of the immune system, such as endocarditis, meningitis, or neutropenic situations. The MBC can also be used in situations where the medium to be tested is turbid, such as urine, where the inhibition of growth cannot be assessed.
Because of the worldwide increase of antibiotic resistance, a secondary aim in the treatment
94
Practical Urology: EssEntial PrinciPlEs and PracticE
of infections has been defined for antimicrobial substances. Especially in the development of new antibiotics, substances with a low potential to cause emergence of antibiotic resistance are selected nowadays.One parameter that describes the probability of an antimicrobial substance is the mutant preventive concentration (MPC). The MPC is defined as the concentration needed to inhibit the emergence of resistant mutants among 1010 bacteria. The MPC might be a future parameter to assess antimicrobial substances and dosing.
Pharmacokinetic Parameters
The pharmacokinetic parameters describe the absorption, distribution, and elimination of an antimicrobial substance, which also includes metabolization of a substance. For simplification, the pharmacokinetic parameters are usually assessed in the blood. However, the pivotal target is the effective antibiotic concentration at the site of infection, which in case of urinary tract infections is the urine and the tissues of the urogenital organs (kidney, bladder, prostate). Additionally, modifying factors, such as protein binding, will influence the concentrations at the site of infection. Pharmacokinetics can also vary remarkably within the population and especially between the patients being the targets treated. Therefore, mathematical models such as the Monte-Carlo simulations are nowadays applied to transfer limited pharmacokinetic data from clinical studies to large population collectives and better reflect the interindividual variations.
Pharmacokinetic/Pharmacodynamic
Correlations
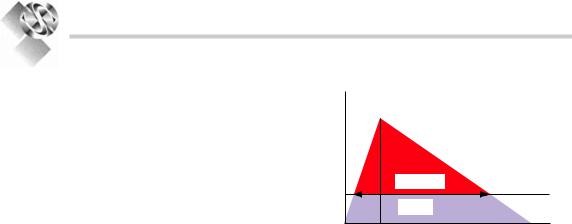
The effect of an antimicrobial substance over the time at the site of infection is the most important pharmacological parameter reflecting therapeutic success. This aspect can be assessed in an integrated evaluation of the pharmacokinetic and pharmacodynamic parameters. In this regard pharmacokinetic parameters are often correlated with the MIC as the pharmacodynamic parameter (Fig. 6.1). Employing those evaluations it became evident that drug classes behave differently toward the pathogens at which they are directed:
Conc.
(mg/L) Cmax
AUC/MIC |
MIC |
T>MIC |
Time (t)
Figure 6.1. association of pharmacokinetic and pharmacodynamic parameters in serum. Cmax maximal concentration, MIC minimal inhibitory concentration, AUC/MIC area under the curve (aUc) over mic, T>MIC time above mic.
b-Lactam agents have their rate of killing maximized at a low multiple of the MIC, because the effect of b-lactams is dependent on their binding to the b-lactam-binding protein within the bacterial cell. The antibacterial effect only appears if a substantial portion of the binding proteins is already occupied by the b-lactam agent. At increasing drug concentrations, the effect quickly maximizes. Therefore, achieving higher drug concentrations does not result in greater killing. For b-lactam agents the best therapeutic results are obtained by using smaller doses more frequently during the day.8
Other antibiotic substances such as aminoglycosides or fluoroquinolones exhibit a concentration dependent post-antibiotic effect. For example,after the removal of the antibiotic there exists still an inhibitory effect on the bacterial cells. This inhibitory effect is greater the higher the initial concentration is. Therefore, for best therapeutic results those antibiotics are usually administered once or twice per day with high doses in order to achieve high peak concentrations (Cmax) or a high area under the concentration time curve (AUC).
Bacterial Spectrum and
Antimicrobial Resistance
Patterns
The above mentioned aspects lead to a selection of antibiotic substances for the individual indication, such as UTI. In the next step a further selection is carried forward based upon the
95
PrinciPlEs of BactErial Urinary tract infEctions and antimicroBials
bacterial spectrum and the current antimicrobial resistance patterns. This is modified over the time depending on the development of bacterial resistance.
In uncomplicated UTI E. coli is the most common pathogen, typically being isolated from approximately 80% of outpatients with acute uncomplicated cystitis across the various regions of the world.2,9-11
A recent surveillance study, the ARESC (Antimicrobial Resistance Epidemiology Survey on Cystitis) project exclusively investigated female patients with uncomplicated cystitis.12 The results of this study showed that antibiotic substances classically used for the treatment of uncomplicated cystitis, such as TMP/SMX, fluoroquinolones or aminopenicillins, lose their effectiveness due to increasing resistance. Substances with high susceptibility rates were fosfomycin tromethamine, nitrofurantoin, or
pivmecillinam.
In uncomplicated pyelonephritis, the identical resistance developments should be expected. For treatment, fluoroquinolones or group 3a cephalosporines might be suitable substances.
In complicated and nosocomially acquired UTI, Gram-negative species account for approximately 60–80% of the bacterial spectrum and comprises E. coli, followed by Klebsiella spp.,
Pseudomonas spp., Proteus spp., Enterobacter spp., and Citrobacter spp. The Gram-positive pathogens account for about 20–40% of the spectrum and comprise enterococci and staphylococci.13-18
Nosocomial uropathogens are frequently subject to antibiotic pressure and cross-infection. Different species of uropathogens show distinct abilities to develop antibiotic resistance.
Surveillance studies such as the SENTRY-, ESGNIor PEP study, or a local urological surveillance study revealed that, considering the total bacterial spectrum investigated, in general the aminopenicillins (with b-lactamase inhibitors) showed resistance rates of approximately 60% (respectively 30%). TMP/SMX showed resistance rates between 22% and 45%. Resistance to ciprofloxacin was approximately 20–40%, to gentamicin 18–34%, to ceftazidime 13–28%, to piperacillin/ tazobactam 8–15%, to imipenem 7–14%. Resistance in enterococci to vancomycin was between 0% and 5%.13-18 In all the studies, increasing rates of antibiotic resistance were found with specific species like E. coli,
P. aeruginosa, Klebsiella spp., Enterobacter spp., enterococci, and coagulase negative staphylococci. Extended-spectrum b-lactamase producing E. coli and K. pneumoniae rapidly increase and may cause significant clinical problems in the treatment of UTI.19,20 Carbapenems fortunately still retained their activity in most of these uropathogens.
Election of an Antibiotic
Treatment
The choice of an antibiotic and its dosage for the treatment of an infection depends on all those described aspects and parameters. Additionally, nowadays the different propensity of the antibiotics to cause so called collateral damages is also considered. Collateral damages are defined as ecological adverse effects of antibiotic therapy, namely, the selection of drug-resistant organisms and the unwanted development of colonization or infection with multidrug-resistant organisms. Different antibiotic classes have significantly different propensities to cause collateral damage.Cephalosporin use,for example,has been linked to subsequent infection with vanco- mycin-resistant enterococci, extended-spectrum beta-lactamase-producing (ESBL) Klebsiella pneumoniae,beta-lactam-resistant Acinetobacter species, and Clostridium difficile. Quinolone use has been linked to infection with methicillinresistant Staphylococcus aureus(MRSA) and with increasingquinoloneresistanceinGram-negative bacilli, such as Pseudomonas aeruginosa.21
To incorporate these different aspects into a concept of antimicrobial chemotherapy of UTIs, for uncomplicated UTIs and especially uncomplicated cystitis, antimicrobials exclusively used for this indication are recommended. For complicated UTIs antibiotics with optimal activity in the urinary tract and high dosage are recommended.
Uncomplicated, Community
Acquired UTI
Ideal substances are those with high susceptibility rates, exclusively used for this indication, such as fosfomycin tromethamine, nitrofurantoin or pivmecillinam for the treatment of uncomplicated cystitis (Table 6.1).