

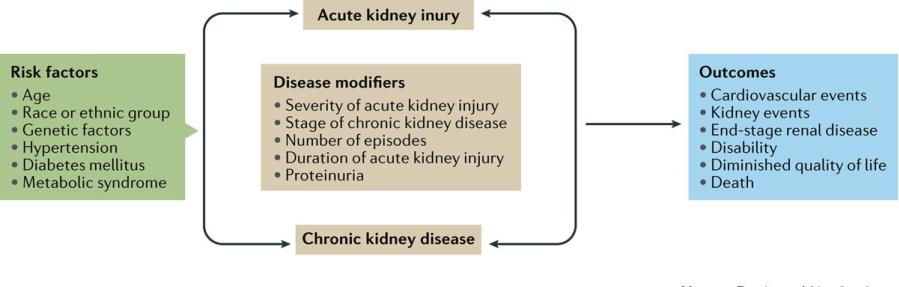
Acute kidney injury and chronic kidney disease
Chawla, L. S. et al. (2017) Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup Nat. Rev. Nephrol. doi:10.1038/nrneph.2017.2
Conceptual model of CKD
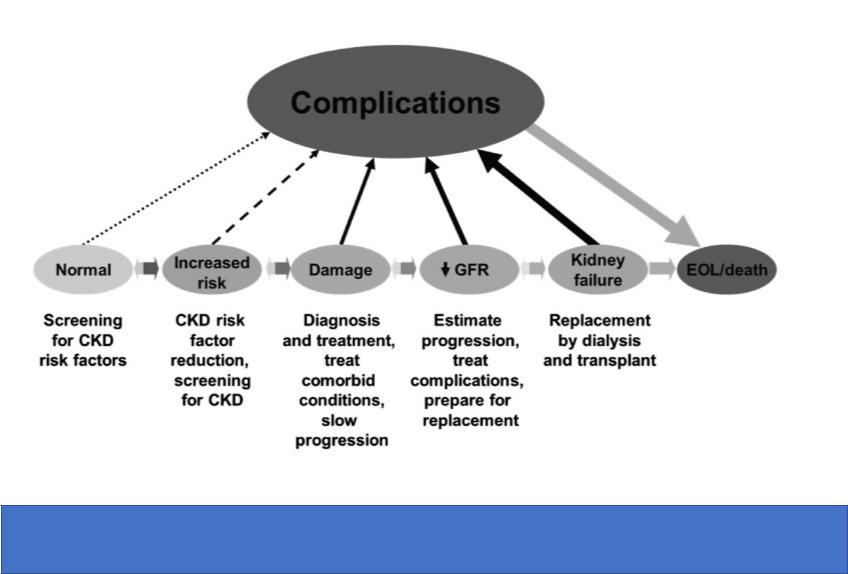
Continuum of development, progression, and complications of CKD and strategies to improve outcomes
Key questions in CKD
Is there GFR decrease |
How to calculate GFR? |
<60 ml/min/1.73 m2? |
|
Albuminuria? |
How to assess albuminuria? |
|
|

Assessment of renal function: estimation of GFR
1976
Cockroft-Gault equation (ml/min) (gender, age, body weight, serum creatinine (sCr))
1999
MDRD formula (ml/min/1.73 m2) (gender, age, ethnicity, sCr)
2009
Highly accurate formula CKD-EPI (ml/min/1.73 m2) (gender, age, ethnicity, sCr)
Why CKD-EPI is the most appropriate estimation of GFR?
•High evidence
•More accurate with ethnic aspects (may be used in mongoloids)
•Takes into consideration increased tubular secretion of creatinine in severe CKD
•May be used at any CKD stage, including early

www.kidney.org

Assessment of renal function: GFR measurement
Reberg-Tareev test (90-140 ml/min/l.73 m2)
CrCl = (Uv)х(Ucr) / (SCr)х(1440) x 1.73 m2/ BSA
Uv = volume of urine/24h, Ucr = creatinine concentration in urine, SCr =creatinine concentration in serum,1440 – minutes in 24 hours, BSA – body surface area, CrCl – clearance ml/min
Measurement of creatinine clearance is used when estimation methods are not appropriate
•Pregnancy
•Non-standard body dimensions (e,g, amputation)
•Severe cachexia or obesity (BMI < 15 or > 40 kg/m2)
•Heavy protein-energy insufficiency
•Diseases of skeletal muscles
•Paraplegia and tetraplegia
•Vegetarian diet
•Rapid decrease of kidney function (acute or rapidly progressive GN)
•Monitoring during therapy with nephrotoxic drugs
•Determination of the dose of drugs with renal excretion in renal failure
•Decision of initiating renal replacement therapy
•Patients with renal transplants

How to assess albuminuria?
1.Dipstick test (random spot urine sample)
•If screening test is positive quantative assessment is needed
2.Quantative albuminuria/proteinuria assessment in 24-h urine
3.Albumin/creatinine ratio in morning spot urine sample
HemoCue Albumin
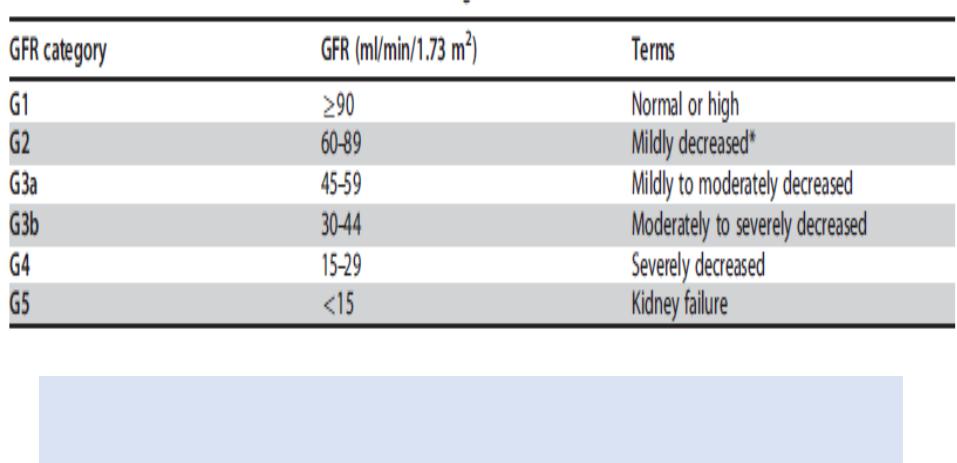
GFR categories in CKD
In the absence of evidence of kidney damage, neither GFR category G1 nor G2 fulfill the criteria for CKD