

- •Overview
- •Preface
- •Translator’s Note
- •Contents
- •1. Fundamentals
- •Microscopic Anatomy of the Nervous System
- •Elements of Neurophysiology
- •Elements of Neurogenetics
- •General Genetics
- •Neurogenetics
- •Genetic Counseling
- •2. The Clinical Interview in Neurology
- •General Principles of History Taking
- •Special Aspects of History Taking
- •3. The Neurological Examination
- •Basic Principles of the Neurological Examination
- •Stance and Gait
- •Examination of the Head and Cranial Nerves
- •Head and Cervical Spine
- •Cranial Nerves
- •Examination of the Upper Limbs
- •Motor Function and Coordination
- •Muscle Tone and Strength
- •Reflexes
- •Sensation
- •Examination of the Trunk
- •Examination of the Lower Limbs
- •Coordination and Strength
- •Reflexes
- •Sensation
- •Examination of the Autonomic Nervous System
- •Neurologically Relevant Aspects of the General Physical Examination
- •Neuropsychological and Psychiatric Examination
- •Psychopathological Findings
- •Neuropsychological Examination
- •Special Considerations in the Neurological Examination of Infants and Young Children
- •Reflexes
- •4. Ancillary Tests in Neurology
- •Fundamentals
- •Imaging Studies
- •Conventional Skeletal Radiographs
- •Computed Tomography (CT)
- •Magnetic Resonance Imaging (MRI)
- •Angiography with Radiological Contrast Media
- •Myelography and Radiculography
- •Electrophysiological Studies
- •Fundamentals
- •Electroencephalography (EEG)
- •Evoked potentials
- •Electromyography
- •Electroneurography
- •Other Electrophysiological Studies
- •Ultrasonography
- •Other Ancillary Studies
- •Cerebrospinal Fluid Studies
- •Tissue Biopsies
- •Perimetry
- •5. Topical Diagnosis and Differential Diagnosis of Neurological Syndromes
- •Fundamentals
- •Muscle Weakness and Other Motor Disturbances
- •Sensory Disturbances
- •Anatomical Substrate of Sensation
- •Disturbances of Consciousness
- •Dysfunction of Specific Areas of the Brain
- •Thalamic Syndromes
- •Brainstem Syndromes
- •Cerebellar Syndromes
- •6. Diseases of the Brain and Meninges
- •Congenital and Perinatally Acquired Diseases of the Brain
- •Fundamentals
- •Special Clinical Forms
- •Traumatic Brain injury
- •Fundamentals
- •Traumatic Hematomas
- •Complications of Traumatic Brain Injury
- •Intracranial Pressure and Brain Tumors
- •Intracranial Pressure
- •Brain Tumors
- •Cerebral Ischemia
- •Nontraumatic Intracranial Hemorrhage
- •Infectious Diseases of the Brain and Meninges
- •Infections Mainly Involving the Meninges
- •Infections Mainly Involving the Brain
- •Intracranial Abscesses
- •Congenital Metabolic Disorders
- •Acquired Metabolic Disorders
- •Diseases of the Basal Ganglia
- •Fundamentals
- •Diseases Causing Hyperkinesia
- •Other Types of Involuntary Movement
- •Cerebellar Diseases
- •Dementing Diseases
- •The Dementia Syndrome
- •Vascular Dementia
- •7. Diseases of the Spinal Cord
- •Anatomical Fundamentals
- •The Main Spinal Cord Syndromes and Their Anatomical Localization
- •Spinal Cord Trauma
- •Spinal Cord Compression
- •Spinal Cord Tumors
- •Myelopathy Due to Cervical Spondylosis
- •Circulatory Disorders of the Spinal Cord
- •Blood Supply of the Spinal Cord
- •Arterial Hypoperfusion
- •Impaired Venous Drainage
- •Infectious and Inflammatory Diseases of the Spinal Cord
- •Syringomyelia and Syringobulbia
- •Diseases Mainly Affecting the Long Tracts of the Spinal Cord
- •Diseases of the Anterior Horns
- •8. Multiple Sclerosis and Other Myelinopathies
- •Fundamentals
- •Myelin
- •Multiple Sclerosis
- •Other Demyelinating Diseases of Unknown Pathogenesis
- •9. Epilepsy and Its Differential Diagnosis
- •Types of Epilepsy
- •Classification of the Epilepsies
- •Generalized Seizures
- •Partial (Focal) Seizures
- •Status Epilepticus
- •Episodic Neurological Disturbances of Nonepileptic Origin
- •Episodic Disturbances with Transient Loss of Consciousness and Falling
- •Episodic Loss of Consciousness without Falling
- •Episodic Movement Disorders without Loss of Consciousness
- •10. Polyradiculopathy and Polyneuropathy
- •Fundamentals
- •Polyradiculitis
- •Cranial Polyradiculitis
- •Polyradiculitis of the Cauda Equina
- •Polyneuropathy
- •Fundamentals
- •11. Diseases of the Cranial Nerves
- •Fundamentals
- •Disturbances of Smell (Olfactory Nerve)
- •Neurological Disturbances of Vision (Optic Nerve)
- •Visual Field Defects
- •Impairment of Visual Acuity
- •Pathological Findings of the Optic Disc
- •Disturbances of Ocular and Pupillary Motility
- •Fundamentals of Eye Movements
- •Oculomotor Disturbances
- •Supranuclear Oculomotor Disturbances
- •Lesions of the Nerves to the Eye Muscles and Their Brainstem Nuclei
- •Ptosis
- •Pupillary Disturbances
- •Lesions of the Trigeminal Nerve
- •Lesions of the Facial Nerve
- •Disturbances of Hearing and Balance; Vertigo
- •Neurological Disturbances of Hearing
- •Disequilibrium and Vertigo
- •The Lower Cranial Nerves
- •Accessory Nerve Palsy
- •Hypoglossal Nerve Palsy
- •Multiple Cranial Nerve Deficits
- •12. Diseases of the Spinal Nerve Roots and Peripheral Nerves
- •Fundamentals
- •Spinal Radicular Syndromes
- •Peripheral Nerve Lesions
- •Fundamentals
- •Diseases of the Brachial Plexus
- •Diseases of the Nerves of the Trunk
- •13. Painful Syndromes
- •Fundamentals
- •Painful Syndromes of the Head And Neck
- •IHS Classification of Headache
- •Approach to the Patient with Headache
- •Migraine
- •Cluster Headache
- •Tension-type Headache
- •Rare Varieties of Primary headache
- •Symptomatic Headache
- •Painful Syndromes of the Face
- •Dangerous Types of Headache
- •“Genuine” Neuralgias in the Face
- •Painful Shoulder−Arm Syndromes (SAS)
- •Neurogenic Arm Pain
- •Vasogenic Arm Pain
- •“Arm Pain of Overuse”
- •Other Types of Arm Pain
- •Pain in the Trunk and Back
- •Thoracic and Abdominal Wall Pain
- •Back Pain
- •Groin Pain
- •Leg Pain
- •Pseudoradicular Pain
- •14. Diseases of Muscle (Myopathies)
- •Structure and Function of Muscle
- •General Symptomatology, Evaluation, and Classification of Muscle Diseases
- •Muscular Dystrophies
- •Autosomal Muscular Dystrophies
- •Myotonic Syndromes and Periodic Paralysis Syndromes
- •Rarer Types of Muscular Dystrophy
- •Diseases Mainly Causing Myotonia
- •Metabolic Myopathies
- •Acute Rhabdomyolysis
- •Mitochondrial Encephalomyopathies
- •Myositis
- •Other Diseases Affecting Muscle
- •Myopathies Due to Systemic Disease
- •Congenital Myopathies
- •Disturbances of Neuromuscular Transmission−Myasthenic Syndromes
- •15. Diseases of the Autonomic Nervous System
- •Anatomy
- •Normal and Pathological Function of the Autonomic Nervous System
- •Sweating
- •Bladder, Bowel, and Sexual Function
- •Generalized Autonomic Dysfunction
- •Index
173
10 Polyradiculopathy and Polyneuropathy
Fundamentals . . . 173
Polyradiculitis . . . 173
Polyneuropathy . . . 176
Fundamentals
In this chapter, we will describe the characteristic syndromes produced by lesions affecting multiple nerve roots or peripheral nerves simultaneously (polyradiculopathy and polyneuropathy, respectively). If nerve roots and peripheral nerves are affected, the disorder is termed polyradiculoneuropathy. These very heterogeneous syndromes can be classified in various ways. Today, they are most commonly classified according to the following criteria:
Temporal course: polyradiculoneuropathy may present acutely with complete or partial remission, or it may take a chronically recurrent or chronically progressive course.
Etiology: polyradiculoneuropathy may be of metabolic, endocrine, toxic, genetic/hereditary, infectious, inflammatory, autoimmune, or paraneoplastic origin.
Pathology: the functioning of the nerve roots and/or peripheral nerves may be impaired either by demyelination or by axonal degeneration. Slowing of nerve conduction early in the course of the illness is a distinguishing feature of demyelinating polyradiculoneuropathy.
The general manifestations of polyradiculopathic and polyneuropathic disorders include:
paresis,
diminution or absence of reflexes,
muscle atrophy,
sensory deficits and positive sensory phenomena (paresthesia, dysesthesia),
pain (in some patients),
predominantly distal symptoms and signs in a symmetrical distribution, or, in other patients, asymmetrical severity,
usually beginning in the lower limbs,
with more or less rapid progression,
with variable involvement of the autonomic nervous system.
The extent, severity, and distribution of these manifestations vary from patient to patient. In addition, predominantly radiculopathic processes are clinically distinguishable from exclusively neuropathic processes. These two types of illness are, therefore, presented separately in the following sections.
Polyradiculitis
This term refers to an inflammatory process affecting many spinal nerve roots (most commonly the anterior ones), usually with simultaneous involvement of the proximal segments of the peripheral nerves. Inflammation of the nerve roots or nerves is usually not caused by infection, but rather by im- mune-mediated processes, e. g., an autoallergic radiculitis or neuritis following a prior, possibly asymptomatic viral or bacterial infection. Clinical variants of polyradiculitis are distinguished from one another by the degree of acuity and predominant localization of symptoms and signs. The acute form, Guillain−Barré syndrome, is the most common; the chronic form (CIDP = chronic inflammatory demyelinating polyradiculoneuropathy) is rarer, as is localized polyradiculoneuritis, which exclusively affect either the cranial nerves or the nerves of the cauda equina. Demyelinating processes are the main pathophysiological mechanism of polyradiculitis. Axonal degeneration is also present, to a varying degree, in CIDP, which explains its protracted course.
Classic Polyradiculitis (Landry−Guillain−
Barré−Strohl Syndrome)
Acute polyradiculitis is characterized by rapidly ascending paresis, accompanied by at most mild sensory disturbances. In severe cases, the cranial nerves and autonomic system can be involved. Weakness usually improves spontaneously in all involved muscles (those that became weak first recover last). The prognosis is favorable.
Epidemiology. This illness, usually called Guillain− Barré syndrome for short, can appear at any age. Its annual incidence is between 0.5 and 2 cases per 100 000 persons. It tends to appear in the spring or fall.
Etiology and pathogenesis. This syndrome probably has more than one cause. Often, no precipitating factor can be identified. In some patients, the illness is preceded by Mycoplasma pneumonia or by infection with varicella-zoster virus, paramyxoviruses (mumps),
Polyradiculopathy and Polyneuropathy
10
Mumenthaler / Mattle, Fundamentals of Neurology © 2006 Thieme All rights reserved. Usage subject to terms and conditions of license.
174 10 Polyradiculopathy and Polyneuropathy
a |
b |
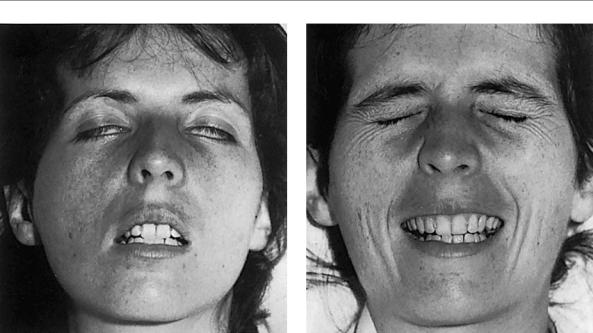
Fig. 10.1 Bilateral peripheral facial nerve palsy in Guillain−Barré polyradiculitis: a acute phase, b after recovery. (From: Mumenthaler, M.: Didaktischer Atlas der klinischen Neurologie, 2nd edn, Springer, Heidelberg, 1986.)
HIV, Epstein−Barr virus (infectious mononucleosis), or Campylobacter jejuni. The last-named organism often produces axonal lesions and is associated with a particularly severe form of the illness. Immunological processes play an important role in pathogenesis; in particular, there is an elevated concentration of antimyelin antibodies. Finally, anti-GD1a antibodies are found in the rarer forms of the illness that involve axonal degeneration, but not in the more common, demyelinating forms (see above).
Clinical manifestations. The first sign is weakness of the lower limbs, beginning distally, occasionally some time after a preceding upper respiratory or gastrointestinal infection. There is no fever. Weakness ascends within a few hours or days, so that the patient becomes unable to walk. Distal paresthesiae and sensory disturbances are present in most patients, but are much less disturbing to the patient than the weakness.
Though the weakness ascends rapidly, its ultimate extent is variable. In very severe cases, the upper limbs, diaphragm, and accessory muscles of respiration are affected, as well as the muscles of the head and neck that are supplied by the cranial nerves. Dysphagia and bilateral facial palsy result (Fig. 10.1). Respiratory failure often develops rapidly and is a life-threatening condition requiring prompt treatment with intubation and artificial ventilation. In addition, involvement of the autonomic nervous system can cause life-threatening abnormalities of blood pressure regulation, cardiac rhythm, central respiratory drive, and, rarely, bladder function.
Diagnostic evaluation. The diagnosis is generally made from the clinical findings and confirmed by the charac-
teristic finding of albumino-cytologic dissociation in the CSF. This term refers to an elevation of the CSF protein concentration without any accompanying elevation of the cell count; the finding may not be present, however, until two or three weeks after the onset of illness. Electrophysiological studies usually reveal focal demyelination with conduction block, or, less commonly, axonal lesions.
Treatment. In severe cases, with profound weakness and rapidly progressive respiratory dysfunction, an intravenous infusion of immunoglobulins is indicated (0.4 g/kg body weight for five consecutive days). Another course can be given in four weeks, if necessary. Plasmapheresis, too, is effective and is recommended for all patients with rapidly ascending paresis and impending respiratory failure, even if the patient can still walk. Such patients should be hospitalized in an intensive care unit, so that their circulatory and respiratory function can be closely monitored and they can be intubated at once, if necessary. In milder cases, general supportive care often suffices: routine nursing, prophylaxis against venous thromboses, urinary catheterization if needed, and, later, physical therapy.
Prognosis. The prognosis is generally favorable. Intensive care may be needed in the acute phase, but, once this is past, the weakness usually resolves in all affected muscles (those that became weak first recover last). Recovery may take several months, however, or even up to two years in very severe cases. Most of the deaths caused by Guillain−Barré syndrome are complications of prolonged immobility (pneumonia, pulmonary embolism) or of autonomic dysfunction (respiratory failure, sudden cardiac death).
Mumenthaler / Mattle, Fundamentals of Neurology © 2006 Thieme All rights reserved. Usage subject to terms and conditions of license.
Polyradiculitis
Chronic Inflammatory Demyelinating
(Recurrent) Polyneuropathy (CIDP)
CIDP, a chronic form of polyradiculitis, has a similar pathophysiological mechanism to Guillain−Barré syndrome, the corresponding acute form. The weakness and autonomic dysfunction are usually less severe, but they last longer. The clinical manifestations fluctuate in severity, often taking a relapsing and remitting or chronically progressive course.
Pathogenesis. The idiopathic form of this condition is presumed to have an immunological basis. Immunoglobulins are found in the CSF and immunoglobulin deposits are seen in biopsy specimens of the sural nerve. There are also forms of CIDP associated with HIV or systemic lupus erythematosus.
Clinical manifestations. CIDP differs from classic, benign Guillain−Barré polyradiculitis in the following ways:
chronic or relapsing-remitting course (more than four weeks),
possibly subacute course,
pain is common,
asymmetrical distribution of neurological deficits,
recurrent cranial nerve involvement,
marked elevation of CSF protein concentration, often combined with an elevated IgG index and pleocytosis,
central nervous manifestations are more common than in Guillain−Barré syndrome,
electroneurography reveals evidence of focal demyelination or axonal damage.
Diagnostic evaluation. Electrophysiological studies reveal slowing of nerve conduction, partial conduction blocks, and a delayed F wave.
Treatment. CIDP is treated with corticosteroids or immunosuppressive agents (cyclophosphamide) for a long period. Immunoglobulins and plasmapheresis are also used, sometimes in combination with immune suppression.
!Although corticosteroids are indicated in the treatment of CIDP, they are only of questionable benefit in Guillain−Barré syndrome.
Prognosis. The prognosis is unfavorable: 10 % of patients die of the disease, 25 % remain severely disabled, and 5 to 10 % have recurrences.
Multifocal Motor Neuropathy (MMN)
This is a special form of CIDP (see above).
Clinical manifestations. MMN is characterized by asymmetrical, slowly or rapidly progressive weakness with muscle atrophy and, sometimes, fasciculations (which may make MMN difficult to distinguish from ALS). There may also be dysarthria and sensory deficits. Some reflexes are lost.
Diagnostic evaluation. Electrophysiological studies reveal sporadic, circumscribed conduction blocks, and laboratory testing often reveals elevated anti-GM1 titers.
Treatment. MMN is treated like other forms of CIDP.
Cranial Polyradiculitis
Polyradiculitis of the cranial nerves may be a component of ascending polyradiculitis, in which case it generally arises only after the limbs have become paretic. Sometimes, however, it is the first, predominant, or only clinical manifestation of polyradiculitis. The differential diagnosis of such patients must always include borreliosis and chronic meningitis (p. 112).
Miller Fisher Syndrome
Clinical manifestations. This special form of cranial polyradiculitis, which mainly affects younger male patients, is characterized by
ophthalmoplegia,
ataxia,
areflexia,
(sometimes) pupillary involvement (e. g., Adie pupil),
(sometimes) facial nerve palsy,
elevated CSF protein concentration,
(sometimes) accompanying brainstem signs.
Treatment. Miller Fisher syndrome has a favorable prognosis and generally needs no specific treatment.
Polyradiculitis of the Cauda Equina
This rare type of polyradiculitis, also called Elsberg syndrome, is characterized by isolated involvement of the sacral roots, producing distal weakness and areflexia of the lower limbs and sphincter dysfunction. Many patients are presumably due to borreliosis or a herpes virus infection.
175
Polyradiculopathy and Polyneuropathy
10
Mumenthaler / Mattle, Fundamentals of Neurology © 2006 Thieme All rights reserved. Usage subject to terms and conditions of license.