

6 курс / Кардиология / Джон_Кэмм_Болезни_сердца_и_сосудов_2011
.pdf25.Plein S., Kozerke S., Suerder D. et al. High spatial resolution myocardial perfusion cardiac magnetic resonance for the detection of coronary artery disease // Eur. Heart J. - 2008. - Vol. Jul 18.
26.Costa M.A., Shoemaker S., Futamatsu H. et al. Quantitative magnetic resonance perfusion imaging detects anatomic and physiologic coronary artery disease as measured by coronary angiography and fractional flow reserve // J. Am. Coll. Cardiol. - 2007. - Vol. 50. - P. 514-522.
27.Wolff S.D., Schwitter J., Coulden R. et al. Myocardial first-pass perfusion magnetic resonance imaging: a multicenter dose-ranging study // Circulation. - 2004. - Vol. 110. - P. 732-737.
28.Rosen B.D., Lima J.A., Nasir K. et al. Lower myocardial perfusion reserve is associated with decreased regional left ventricular function in asymptomatic participants of the multi-ethnic study of atherosclerosis // Circulation. - 2006. - Vol. 114. - P. 289-297.
29.Schwitter J., Wacker C.M., van Rossum A.C. et al. MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomography for the detection of coronary artery disease in a multicentre, multivendor, randomized trial // Eur. Heart J. - 2008. - Vol. 29. - P. 480489.
30.Fieno D.S., Shea S.M., Li Y. et al. Myocardial perfusion imaging based on the blood oxygen leveldependent effect using T2-prepared steady-state free-precession magnetic resonance imaging // Circulation. - 2004. - Vol. 110. - P. 1284-1290.
31.Plein S., Greenwood J.P., Ridgway J.P. et al. Assessment of non-ST-segment elevation acute coronary syndromes with cardiac magnetic resonance imaging // J. Am. Coll. Cardiol. - 2004. - Vol. 44. - P. 2173-2181.
32.Jahnke C., Nagel E., Gebker R. et al. Prognostic value of cardiac magnetic resonance stress tests: adenosine stress perfusion and dobutamine stress wall motion imaging // Circulation. - 2007. - Vol. 115. - P. 1769-1776.
33.Panting J.R., Gatehouse P.D., Yang G.Z. et al. Abnormal subendocardial perfusion in cardiac syndrome X detected by cardiovascular magnetic resonance imaging // N. Engl. J. Med. - 2002. - Vol. 346. - P. 1948-1953.
34.Lanza G.A., Buffon A., Sestito A. et al. Relation between stress-induced myocardial perfusion defects on cardiovascular magnetic resonance and coronary microvascular dysfunction in patients with cardiac syndrome X // J. Am. Coll. Cardiol. - 2008. - Vol. 51. - P. 466-472.
35.Kwong R.Y., Schussheim A.E., Rekhraj S. et al. Detecting acute coronary syndrome in the emergency department with cardiac magnetic resonance imaging // Circulation. - 2003. - Vol. 107. - P. 531-517.
36.Bassand J.P., Hamm C.W., Ardissino D. et al. Guidelines for the diagnosis and treatment of non-ST- segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non- ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology // Eur. Heart J. - 2007. - Vol. 28. - P. 1598-1660.
37.Plein S., Greenwood J.P., Ridgway J.P. et al. Assessment of non-ST-segment elevation acute coronary syndromes with cardiac magnetic resonance imaging // J. Am. Coll. Cardiol. - 2004. - Vol. 44. - P. 2173-2181.
38.Greenwood J.P., Younger J.F., Ridgway J.P. et al. Safety and diagnostic accuracy of stress cardiac magnetic resonance imaging vs exercise tolerance testing early after acute ST elevation myocardial infarction // Heart. - 2007. - Vol. 93. - P. 1363-138.
39.Ingkanisorn W.P., Kwong R.Y., Bohme N.S. et al. Prognosis of negative adenosine stress magnetic resonance in patients presenting to an emergency department with chest pain // J. Am. Coll. Cardiol. - 2006. - Vol. 47. - P. 1427-1432.
40.Cury R.C., Shash K., Nagurney J.T. et al. Cardiac magnetic resonance with T2-weighted imaging improves detection of patients with acute coronary syndrome in the emergency department // Circulation. - 2008. - Vol. 118. - P. 837-844.
41.Assomull R.G, Lyne JC, Keenan N, et al. The role of cardiovascular magnetic resonance in patients presenting with chest pain, raised troponin, and unobstructed coronary arteries // Eur Heart J. - 2007. - Vol. 28. - P. 1242-1249.
42.Abdel-Aty H., Zagrosek A., Schulz-Menger J. et al. Delayed enhancement and T2-weighted cardiovascular magnetic resonance imaging differentiate acute from chronic myocardial infarction // Circulation. - 2004. - Vol. 109. - P. 2411-2416.
43.Friedrich M.G., Abdel-Aty H., Taylor A. et al. The salvaged area at risk in reperfused acute myocardial infarction as visualized by cardiovascular magnetic resonance // J. Am. Coll. Cardiol. - 2008. - Vol. 51. - P. 1581-1587.
44.Ricciardi M.J., Wu E., Davidson C.J. et al. Visualization of discrete microinfarction after percutaneous coronary intervention associated with mild creatine kinase-MB elevation // Circulation. - 2001. - Vol. 103. - P. 2780-2783.
45.Mollet N.R., Dymarkowski S., Volders W. et al. Visualization of ventricular thrombi with contrastenhanced magnetic resonance imaging in patients with ischemic heart disease // Circulation. - 2002. - Vol. 106. - P. 2873-2876.
46.Johnson K.R., Patel S.J., Whigham A. et al. Three-dimensional, time-resolved motion of the coronary arteries // J. Cardiovasc. Magn. Reson. - 2004. - Vol. 6. - P. 663-673.
47.Paetsch I., Jahnke C., Barkhausen J. et al. Detection of coronary stenoses with contrast enhanced, three-dimensional free breathing coronary MR angiography using the gadolinium-based intravascular contrast agent gadocoletic acid (B-22956) // J. Cardiovasc. Magn. Reson. - 2006. - Vol. 8. - P. 509-516.
48.Sakuma H., Ichikawa Y., Chino S. et al. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography // J. Am. Coll. Cardiol. - 2006. - Vol. 48. - P. 1946-1950.
49.le Polain de Waroux J.B., Pouleur A.C., Goffinet C. et al. Combined coronary and late-enhanced multidetector-computed tomography for delineation of the etiology of left ventricular dysfunction: comparison with coronary angiography and contrast-enhanced cardiac magnetic resonance imaging // Eur. Heart J. - 2008. - Vol. 29. - P. 2544-2551.
50.Kim W.Y., Danias P.G., Stuber M. et al. Coronary magnetic resonance angiography for the detection of coronary stenoses // N. Engl. J. Med. - 2001. - Vol. 345. - P. 1863-1869.
51.Kim W.Y., Astrup A.S., Stuber M. et al. Subclinical coronary and aortic atherosclerosis detected by magnetic resonance imaging in type 1. diabetes with and without diabetic nephropathy // Circulation. - 2007. - Vol. 115. - P. 228-235.
52.Taylor A.M., Thorne S.A., Rubens M.B. et al. Coronary artery imaging in grown up congenital heart disease: complementary role of magnetic resonance and x-ray coronary angiography // Circulation. - 2000. - Vol. 101. - P. 1670-1678.
53.Langerak S.E., Kunz P., Vliegen H.W. et al. MR flow mapping in coronary artery bypass grafts: a validation study with Doppler flow measurements // Radiology. - 2002. - Vol. 222. - P. 127-135.
54.Mavrogeni S., Papadopoulos G., Douskou M. et al. Magnetic resonance angiography is equivalent to X-ray coronary angiography for the evaluation of coronary arteries in Kawasaki disease // J. Am. Coll. Cardiol. - 2004. - Vol. 43. - P. 649-652.
55.Kim W.Y., Stuber M., Bornert P. et al. Three-dimensional black-blood cardiac magnetic resonance coronary vessel wall imaging detects positive arterial remodeling in patients with nonsignificant coronary artery disease // Circulation. - 2002. - Vol. 106. - P. 296-299.
56.Wilensky R.L., Song H.K., Ferrari V.A. Role of magnetic resonance and intravascular magnetic resonance in the detection of vulnerable plaques // J. Am. Coll. Cardiol. - 2006. - Vol. 47. (Suppl. 8). - P. C48-C56.
57.Keenan N.G., Locca D., Roughton M. et al. Magnetic resonance of carotid artery aging in healthy subjects // Atherosclerosis. - 2008. - Vol. Nov 27.
58.Corti R., Fuster V., Fayad Z.A. et al. Lipid lowering by simvastatin induces regression of human atherosclerotic lesions: two years’ follow-up by high-resolution noninvasive magnetic resonance imaging // Circulation. - 2002. - Vol. 106. - P. 2884-2887.
59.Sorenson M.B., Collins P., Ong P.J.L. et al. Long term use of contraceptive depot medroxyprogesterone acetate in young women impairs arterial endothelial function assessed by cardiovascular magnetic resonance // Circulation. - 2002. - Vol. 106. - P. 1646-1651.
60.Cai J.M., Hatsukami T.S., Ferguson M.S. et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging // Circulation. - 2002. - Vol. 106. - P. 1368-1373.
61.Yuan C., Zhang S.X., Polissar N.L. et al. Identification of fibrous cap rupture with magnetic resonance imaging is highly associated with recent transient ischemic attack or stroke // Circulation. - 2002. -
Vol. 105. - P. 181-185.
62.Rickers C., Wilke N.M., Jerosch-Herold M. et al. Utility of cardiac magnetic resonance imaging in the diagnosis of hypertrophic cardiomyopathy // Circulation. - 2005. - Vol. 112. - P. 855-861.
63.Olivotto I., Maron M.S., Autore C. et al. Assessment and significance of left ventricular mass by cardiovascular magnetic resonance in hypertrophic cardiomyopathy // J. Am. Coll. Cardiol. - 2008. - Vol. 52. - P. 559-566.
64.Abdel-Aty H., Cocker M., Strohm O. et al. Abnormalities in T2-weighted cardiovascular magnetic resonance images of hypertrophic cardiomyopathy: regional distribution and relation to late gadolinium enhancement and severity of hypertrophy // J. Magn. Reson. Imaging. - 2008. - Vol. 28. - P. 242-245.
65.Moon J.C., Fisher N.G., McKenna W.J. et al. Detection of apical hypertrophic cardiomyopathy by cardiovascular magnetic resonance in patients with non-diagnostic echocardiography // Heart. - 2004. - Vol. 90. - P. 645-649.
66.Maron M.S., Hauser T.H., Dubrow E. et al. Right ventricular involvement in hypertrophic cardiomyopathy // Am. J. Cardiol. - 2007. - Vol. 100. - P. 1293-1298.
67.Crilley J.G., Boehm E.A., Blair E. et al. Hypertrophic cardiomyopathy due to sarcomeric gene mutations is characterized by impaired energy metabolism irrespective of the degree of hypertrophy // J. Am. Coll. Cardiol. - 2003. - Vol. 41. - P. 1776-1782.
68.Moon J.C.C., Reed E., Sheppard M.A. et al. The histological basis of late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy // J. Am. Coll. Cardiol. - 2004. - Vol. 43. - P. 2260-2264.
69.Moon J.C.C., McKenna W.J., McCrohon J.A. et al. Toward clinical risk assessment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance // J. Am. Coll. Cardiol. - 2003. - Vol. 41. - P. 1561-1567.
70.Adabag A.S., Maron B.J., Appelbaum E. et al. Occurrence and frequency of arrhythmias in hypertrophic cardiomyopathy in relation to delayed enhancement on cardiovascular magnetic resonance // J. Am. Coll. Cardiol. - 2008. - Vol. 51. - P. 1369-1374.
71.Petersen S.E., Jerosch-Herold M., Hudsmith L.E. et al. Evidence for microvascular dysfunction in hypertrophic cardiomyopathy: new insights from multiparametric magnetic resonance imaging // Circulation. - 2007. - Vol. 115. - P. 2418-2425.
72.Sachdev B., Takenaka T., Teraguchi H. et al. Prevalence of Anderson-Fabry disease in male patients with late onset hypertrophic cardiomyopathy // Circulation. - 2002. - Vol. 105. - P. 1407-1411.
73.Moon J.C.C., Sachdev B., Elkington A.G. et al. Gadolinium enhanced cardiovascular magnetic resonance in Anderson-Fabry disease: Evidence for a disease specific abnormality of the myocardial interstitium // Eur. Heart J. - 2003. - Vol. 24. - P. 2151-2155.
74.Hughes D.A., Elliott P.M., Shah J. et al. Effects of enzyme replacement therapy on the cardiomyopathy of Anderson-Fabry disease: a randomised, double-blind, placebo-controlled clinical trial of agalsidase alfa // Heart. - 2008. - Vol. 94. - P. 15315-15318.
75.McCrohon J.A., Moon J.C., Prasad S.K. et al. Differentiation of heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-enhanced cardiovascular magnetic resonance // Circulation. - 2003. - Vol. 108. - P. 54-59.
76.Assomull R.G., Prasad S.K., Lyne J. et al. Cardiovascular magnetic resonance, fibrosis, and prognosis in dilated cardiomyopathy // J. Am. Coll. Cardiol. - 2006. - Vol. 48. - P. 1977-1985.
77.Nazarian S., Bluemke D.A., Lardo A.C. et al. Magnetic resonance assessment of the substrate for inducible ventriclar tachycardia in nonischemic cardiomyopathy // Circulation. - 2005. - Vol. 112. -
P. 2821-2825.
78.Soriano C.J., Ridocci F., Estornell J. et al. Late gadolinium-enhanced cardiovascular magnetic resonance identifies patients with standardized definition of ischemic cardiomyopathy: a single centre experience // Int. J. Cardiol. - 2007. - Vol. 116. - P. 167-173.
79.Wu K.C., Weiss R.G., Thiemann D.R. et al. Late gadolinium enhancement by cardiovascular magnetic resonance heralds an adverse prognosis in nonischemic cardiomyopathy // J. Am. Coll. Cardiol. - 2008. - Vol. 51. - P. 2414-2421.
80.Neubauer S., Horn M., Cramer M. et al. Myocardial phosphocreatine to ATP ratio is a predictor of mortality in patients with dilated cardiomyopathy // Circulation. - 1997. - Vol. 96. - P. 2190-2196.
81.Modell B., Khan M., Darlison M. Survival in beta thalassaemia major in the UK: Data from the UK Thalassaemia Register // Lancet. - 2000. - Vol. 355. - P. 2051-2052.
82.Anderson L.J., Westwood M.A., Prescott E. et al. Development of thalassaemic iron overload cardiomyopathy despite low liver iron levels and meticulous compliance to desferrioxamine // Acta Haematol. - 2006. - Vol. 115. - P. 106-108.
83.Westwood M.A., Sheppard M.N., Awogbade M, et al. Myocardial biopsy and T2* magnetic resonance in heart failure due to thalassemia // Br. J. Haematol. - 2005. - Vol. 128. - P. 2.
84.Anderson L.J., Holden S., Davies B. et al. Cardiovascular T2* (T2. star) magnetic resonance for the early diagnosis of myocardial iron overload // Eur. Heart J. - 2001. - Vol. 22. - P. 2171-2179.
85.Westwood M., Anderson L.J., Firmin D.N. et al. A single breath-hold multiecho T2* cardiovascular magnetic resonance technique for diagnosis of myocardial iron overload // J. Magn. Reson. Imaging. - 2003. - Vol. 18. - P. 33-39.
86.Westwood M., Anderson L.J., Firmin D.N. et al. Interscanner reproducibility of cardiovascular magnetic resonance in the early diagnosis of myocardial iron overload // J. Magn. Reson. Imaging. - 2003. -
Vol. 18. - P. 616-620.
87.Westwood M.A., Firmin D.N., Gildo M. et al. Intercentre reproducibility of magnetic resonance T2* measurements of myocardial iron in thalassaemia // Int. J. Cardiovasc. Imaging. - 2005. - Vol. 21. - P. 531-538.
88.Tanner M.A., Galanello R., Dessi C. et al. Myocardial iron loading in patients with thalassemia major on deferoxamine chelation // J. Cardiovasc. Magn. Reson. - 2006. - Vol. 8. - P. 543-547.
89.Daar S., Pathare A.V., Jain R. et al. T2* cardiovascular magnetic resonance in the management of thalassemia patients in Oman // Haematologica. - 2009. - Vol. 94. - P. 140-141.
90.Au W.Y., Lam W.W., Chu W.W. et al. A cross-sectional magnetic resonance imaging assessment of organ specific hemosiderosis in 180. thalassemia major patients in Hong Kong // Haematologica. - 2008. - Vol. 93. - P. 784-786.
91.Aessopos A., Fragodimitri C., Karabatsos F. et al. Cardiac magnetic resonance imaging R2* assessments and analysis of historical parameters in patients with transfusion-dependent thalassemia // Haematologica. - 2007. - Vol. 92. - P. 131-132.
92.Westwood M.A., Anderson L.J., Maceira A.M. et al. Normalized left ventricular volumes and function in thalassemia major patients with normal myocardial iron // J. Magn. Reson. Imaging. - 2007. - Vol. 25. -
P. 1147-1151.
93.Westwood M.A., Wonke B., Maceira A.M. et al. Left ventricular diastolic function compared with T2* cardiovascular magnetic resonance for early detection of myocardial iron overload in thalassemia major // J. Magn. Reson. Imaging. - 2005. - Vol. 22. - P. 229-233.
94.Anderson L.J., Westwood M.A., Holden S. et al. Myocardial iron clearance during reversal of siderotic cardiomyopathy with intravenous desferrioxamine: a prospective study using T2* cardiovascular magnetic resonance // Br. J. Haematol. - 2004. - Vol. 127. - P. 348-355.
95.Pennell D.J., Berdoukas V., Karagiorga M. et al. Randomized controlled trial of deferiprone or deferoxamine in beta-thalassemia major patients with asymptomatic myocardial siderosis // Blood. - 2006. - Vol. 107. - P. 3738-3744.
96.Tanner M.A., Galanello R., Dessi C. et al. A randomized, placebo-controlled, double-blind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonance // Circulation. - 2007. - Vol. 115. - P. 1876-1884.
97.Tanner M.A., Galanello R., Dessi C. et al. Combined chelation therapy in thalassemia major for the treatment of severe myocardial siderosis with left ventricular dysfunction // J. Cardiovasc. Magn. Reson. - 2008. - Vol. 10. - P. 12.
98.Modell B., Khan M., Darlison M. et al. Improved survival of thalassaemia major in the UK and relation to T2* cardiovascular magnetic resonance // J. Cardiovasc. Magn. Reson. - 2008. - Vol. 10. - P. 42.
99.Borgna-Pignatti C., Cappellini M.D., De Stefano P. et al. Cardiac morbidity and mortality in deferoxamineor deferiprone-treated patients with thalassemia major // Blood. - 2006. - Vol. 107. - P. 3733-3737.
100.Telfer P., Coen P.G., Christou S. et al. Survival of medically treated thalassemia patients in Cyprus. Trends and risk factors over the period 1980-2004 // Haematologica. - 2006. - Vol. 91. - P. 1187-1192.
101.Sen-Chowdhry S., Prasad S.K., Syrris P. et al. Cardiovascular magnetic resonance in arrhythmogenic right ventricular cardiomyopathy revisited Comparison with Task Force Criteria and genotype // J. Am. Coll. Cardiol. - 2006. - Vol. 48. - P. 2132-2140.
102.Tandri H., Saranathan M., Rodriguez E.R. et al. Noninvasive detection of myocardial fibrosis in arrhythmogenic right ventricular cardiomyopathy using delayed-enhancement magnetic resonance imaging // J. Am. Coll. Cardiol. - 2005. - Vol. 45. - P. 98-103.
103.Iannuzzi M.C., Rybicki B.A., Teirstein A.S. Sarcoidosis // N. Engl. J. Med. - 2007. - Vol. 357. - P. 2153-2165.
104.Smedema J.P., Snoep G., van Kroonenburgh M.P. et al. Evaluation of the accuracy of gadoliniumenhanced CMR in the diagnosis of cardiac sarcoidosis // J. Am. Coll. Cardiol. - 2005. - Vol. 45. - P. 16831690.
105.Vignaux O., Dhote R., Duboc D. et al. Clinical significance of myocardial magnetic resonance abnormalities in patients with sarcoidosis: a 1-year follow-up study // Chest. - 2002. - Vol. 122. - P. 18951901.
106.Shah K.B., Inoue Y., Mehra M.R. Amyloidosis and the // Heart: a comprehensive review // Arch. Intern. Med. - 2006. - Vol. 166. - P. 1805-1813.
107.Maceira A.M., Joshi J., Prasad S.K. et al. Cardiovascular magnetic resonance in cardiac amyloidosis // Circulation. - 2005. - Vol. 111. -
P. 186-193.
108.Vogelsberg H., Mahrholdt H., Deluigi C.C. et al. Cardiovascular magnetic resonance in clinically suspected cardiac amyloidosis: noninvasive imaging compared to endomyocardial biopsy // J. Am. Coll. Cardiol. - 2008. - Vol. 51. - P. 1022-1030.
109.Kohli S.K., Pantazis A.A., Shah J.S. et al. Diagnosis of left-ventricular non-compaction in patients with left-ventricular systolic dysfunction: time for a reappraisal of diagnostic criteria? // Eur. Heart J. - 2008. - Vol. 29. - P. 89-95.
110.Petersen S.E., Selvanayagam J.B., Wiesmann F. et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging // J. Am. Coll. Cardiol. - 2005. - Vol. 46. - P. 101-105.
111.Friedrich M.G., Strohm O., Schulz-Menger J. et al. Contrast media enhanced magnetic resonance imaging visualises myocardial changes in the course of viral myocarditis // Circulation. - 1998. - Vol. 97. - P. 1802-1809.
112.Mahrholdt H., Goedecke C., Wagner A. et al. Cardiovascular magnetic resonance assessment of human myocarditis: a comparison to histology and molecular pathology // Circulation. - 2004. - Vol. 109. - P. 1250-1258.
113.Mahrholdt H., Wagner A., Deluigi C.C. et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis // Circulation. - 2006. - Vol. 114. - P. 1581-1590.
114.Assomull R.G., Lyne J.C., Keenan N. et al. The role of cardiovascular magnetic resonance in patients presenting with chest pain, raised troponin, and unobstructed coronary arteries // Eur. Heart J. - 2007. - Vol. 28. - P. 1242-1249.
115.Kilner P.J., Gatehouse P.D., Firmin D.N. Flow measurement by magnetic resonance: a unique asset worth optimising // J. Cardiovasc. Magn. Reson. - 2007. - Vol. 9. - P. 723-728.
116.Baltes C., Hansen M.S., Tsao J. et al. Determination of peak velocity in stenotic areas: echocardiography versus k-t SENSE accelerated MR Fourier velocity encoding // Radiology. - 2008. - Vol. 246. - P. 249-257.
117.Oosterhof T., van S.A., Vliegen H.W. et al. Preoperative thresholds for pulmonary valve replacement in patients with corrected tetralogy of Fallot using cardiovascular magnetic resonance // Circulation. - 2007. - Vol. 116. - P. 545-551.
118.Kozerke S., Schwitter J., Pedersen E.M. et al. Aortic and mitral regurgitation: quantification using moving slice velocity mapping // J. Magn. Reson. Imaging. - 2001. - Vol. 14. - P. 106-112.
119.Caruthers S.D., Lin S.J., Brown P. et al. Practical value of cardiac magnetic resonance imaging for clinical quantification of aortic valve stenosis: comparison with echocardiography // Circulation. - 2003. - Vol. 108. - P. 2236-2243.
120.Reant P., Lederlin M., Lafitte S. et al. Absolute assessment of aortic valve stenosis by planimetry using cardiovascular magnetic resonance imaging: comparison with transesophageal echocardiography, transthoracic echocardiography, and cardiac catheterization // Eur. J. Radiol. - 2006. - Vol. 59. - P. 276283.
121.Tanaka K, Makaryus A.N., Wolff S.D. Correlation of aortic valve area obtained by the velocityencoded phase contrast continuity method to direct planimetry using cardiovascular magnetic resonance // J. Cardiovasc. Magn. Reson. - 2007. - Vol. 9. - P. 799-805.
122.Yap S.C., van Geuns R.J., Meijboom F.J. et al. A simplified continuity equation approach to the quantification of stenotic bicuspid aortic valves using velocity-encoded cardiovascular magnetic resonance // J. Cardiovasc. Magn. Reson. - 2007. - Vol. 9. - P. 899-906.
123.Kon M.W., Myerson S.G., Moat N.E. et al. Quantification of regurgitant fraction in mitral regurgitation by cardiovascular magnetic resonance: comparison of techniques // J. Heart Valve Dis. - 2004. July. - Vol. 13. - P. 600-607.
124.Shellock F.G. Prosthetic heart valves and annuloplasty rings: assessment of magnetic field interactions, heating, and artifacts at 1.5. Tesla // J. Cardiovasc. Magn. Reson. - 2001. - Vol. 3. - P. 317324.
125.Masci P.G., Dymarkowski S., Bogaert J. Valvular heart disease: what does cardiovascular MRI add? // Eur. Radiol. - 2008. - Vol. 18. - P. 197-208.
126.Boxt L.M., Rozenshtein A. MR imaging of congenital heart disease // Magn. Reson. Imaging Clin. N. Am. - 2003. - Vol. 11. - P. 27-48.
127.Korperich H., Gieseke J., Barth P. et al. Flow volume and shunt quantification in pediatric congenital heart disease by real-time magnetic resonance velocity mapping: a validation study // Circulation. - 2004. - Vol. 109. - P. 1987-1993.
128.Prasad S.K., Soukias N., Hornung T. et al. Role of magnetic resonance angiography in the diagnosis of major aortopulmonary collateral arteries and partial anomalous pulmonary venous drainage // Circulation. - 2004. - Vol. 109. - P. 207-214.
129.Frigiola A., Tsang V., Bull C. et al. Biventricular response after pulmonary valve replacement for right ventricular outflow tract dysfunction: is age a predictor of outcome? // Circulation. - 2008. -
Vol. 118. (Suppl.14). - P. S182-S190.
130.Woodard P.K., Bhalla S., Javidan-Nejad C. et al. Cardiac MRI in the management of congenital heart disease in children, adolescents, and young adults // Curr. Treat. Options Cardiovasc. Med. - 2008. -
Vol. 10. - P. 419-424.
131.Kramer C.M., Barkhausen J., Flamm S.D. et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for cardiovascular magnetic resonance: board of trustees task force on standardized protocols // J. Cardiovasc. Magn. Reson. - 2008. - Vol. 10. - P. 35.
132.Ho V.B. ACR appropriateness criteria on suspected congenital heart disease in adults // J. Am. Coll. Radiol. - 2008. - Vol. 5. - P. 97-104.
133.Crean A. Cardiovascular MR and CT in congenital heart disease // Heart. - 2007. - Vol. 93. - P. 16371647.
134.Narváez J., Narváez J.A., Nolla J.M. et al. Giant cell arteritis and polymyalgia rheumatica: usefulness of vascular magnetic resonance imaging studies in the diagnosis of aortitis. Rheumatology. - 2005. -
Vol. 44. - P. 479-483.
135.Weinsaft J.W., Kim H.W., Shah D.J. et al. Detection of left ventricular thrombus by delayedenhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction // J. Am. Coll. Cardiol. - 2008. - Vol. 52. - P. 148-157.
136.Shiga T., Wajima Z., Apfel C.C. et al. Diagnostic accuracy of transesophageal echocardiography, helical computed tomography, and magnetic resonance imaging for suspected thoracic aortic dissection: systematic review and meta-analysis // Arch. Intern. Med. - 2006. - Vol. 166. - P. 1350-1356.
137.Ersoy H., Goldhaber S.Z., Cai T. et al. Time-resolved MR angiography: a primary screening examination of patients with suspected pulmonary embolism and contraindications to administration of iodinated contrast material // Am. J. Roentgenol. - 2007. - Vol. 188. - P. 1246-1254.
138.Masui T., Finck S., Higgins C.B. Constrictive pericarditis and restrictive cardiomyopathy: evaluation with MR imaging // Radiology. - 1992. - Vol. 182. - P. 369-373.
139.Fieno D.S., Saouaf R., Thomson L.E. et al. Cardiovascular magnetic resonance of primary tumors of the heart: a review // J. Cardiovasc. Magn. Reson. - 2006. - Vol. 8. - P. 839-853.
ГЛАВА 06. КОМПЬЮТЕРНАЯ ТОМОГРАФИЯ СЕРДЦА
Pim J. de Feyter, Stephan Achenbach и Koen Nieman
РЕЗЮМЕ
Нативная компьютерная томография (КТ), визуализирующая обызвествления в венечных артериях, вне зависимости от факторов риска может спрогнозировать неблагоприятные коронарные события, потому что эти обызвествления являются маркером коронарного атеросклероза.
Контрастная КТ-коронарография служит надежным неинвазивным диагностическим методом исключения значимой обструкции венечных артерий у больных с низкой и средней степенью риска ИБС и синусовым сердечным ритмом. КТ-визуализация сосудистой стенки дает возможность оценить ранние проявления атеросклероза венечных артерий. Обширные обызвествления венечных артерий и нарушения ритма сердца значительно затрудняют оценку этих сосудов, при этом увеличивая лучевую нагрузку на пациента.
При КТ очень точно можно диагностировать ТЭЛА и острое расслоение аорты, поэтому КТ считают "золотым стандартом" диагностики данной патологии. При помощи КТ можно получить изображения магистральных сосудов груди, оценить функцию клапанов сердца, выявить опухоли сердца, тромбы в его полостях или заболевания перикарда Однако в качестве первостепенных методов диагностики следует рассматривать ЭхоКГ и МРТ сердца как методы, не связанные с использованием ионизирующих излучений.
ВВЕДЕНИЕ
Развитие рентгеновской КТ в 1970-х годах считают одним из крупных успехов в диагностике из-за ее способности неинвазивно получать изображение внутренних структур организма с беспрецедентной точностью. Нет другого метода, позволяющего сканировать большие области тела с сопоставимым пространственным разрешением и контрастностью при очень небольшом времени исследования. Высокого пространственного и тканевого разрешения КТ удается достичь из-за того, что коллимированный пучок рентгеновских лучей выборочно проходит через определенное поперечное сечение исследуемого объекта, сводя к минимуму наложение структур, расположенных выше и ниже этого слоя. Также, в силу снижения рентгеновского рассеивания, улучшается контрастность изображения. Наконец, при КТ используют очень чувствительные детекторы, способные распознавать незначительные различия в контрастном разрешении (‹0,1%). Контрастная электронно-лучевая КТ-коронарография в 1995 г была описана и впоследствии продемонстрирована в качестве метода, неинвазивно определяющего гемодинамически значимые стенозы венечной артерии со средней степенью точности.
В 1990-х годах была представлена "спиральная" КТ, сочетающая непрерывное вращение рентгеновской трубки с непрерывным движением стола с пациентом вдоль оси Z. В отличие от электронно-лучевой КТ-коронарографии, этот метод развивался чрезвычайно быстро, так что за последние несколько лет зарекомендовал себя надежным неинвазивным способом отображения сердечно-сосудистой системы.
ОСНОВЫ КОМПЬЮТЕРНОЙ ТОМОГРАФИИ
КТ - это метод исследования, использующий рентгеновское излучение для создания поперечных томографических изображений. Рентгеновские лучи возникают в рентгеновской трубке и коллимируются в веерообразный или конусообразный пучок, который проходит через объект от источника излучения к приемнику излучения (рис. 6.1).

Рис. 6.1. Принцип работы сканера мультиспирального компьютерного томографа. Вращающаяся рентгеновская трубка производит конусовидный пучок лучей, который проходит через пациента, находящегося в гентри. Ослабленные рентгеновские лучи собираются множественными рядами детекторов.
После частичного поглощения и рассеяния остающиеся рентгеновские лучи регистрируются детекторами на противоположной стороне сканера (рис. 6.2). Профиль ослабления, зарегистрированный детекторами, является результатом суммарного ослабления излучения тканями. Собирая большое количество профилей ослабления при вращении трубки и детекторов, можно вычислить вклад ослабления рентгеновского излучения локального участка ткани в поперечном сечении. Минимальное количество профилей, требуемых для выполнения этого вычисления, получают при вращении рентгеновской трубки и датчиков на 180°. Количественно степень ослабления излучения в КТ, выраженная в единицах Хаунсфилда (HU), может быть вычислена следующим образом:
где µtissue - коэффициент ослабления ткани; µwater - коэффициент ослабления воды.
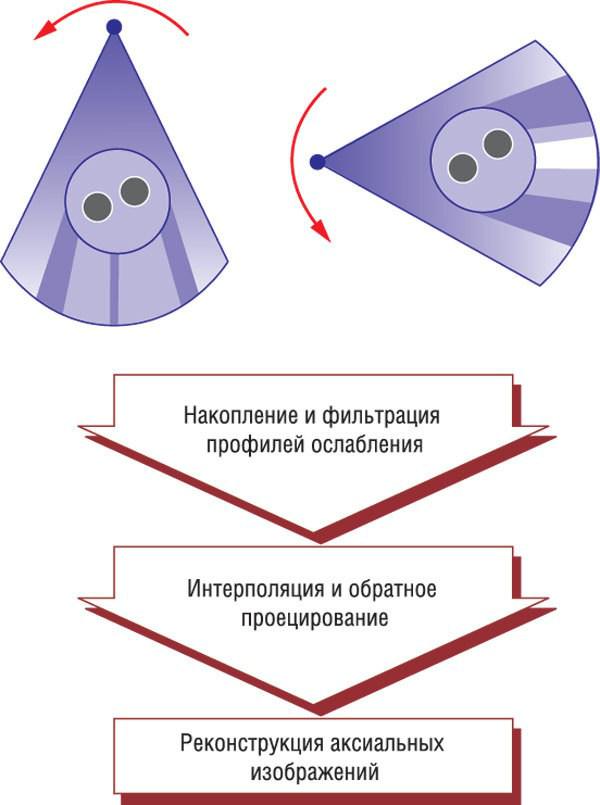
Рис. 6.2. Принцип работы компьютерного томографа. Многократные профили ослабления от различных углов получены во время вращения системы датчика и рентгеновской трубки на 180 градусов. В случае спиральной компьютерной томографии профили ослабления интерполируются по продольной оси, создавая полные наборы данных для каждого аксиального среза. Аксиальные изображения создаются из интерполированных наборов данных, используя алгоритм обратных проекций.
По определению, относительная рентгеновскакя плотность воды составляет 0 HU, у воздуха (слабое ослабление) относительная рентгеновская плотность составляет около -1000 HU. Кость, так же как металл (высокое ослабление), имеет относительную рентгеновскую плотность более

1000 HU и будет отображаться на экране монитора белым цветом; ткани с низким ослаблением, такие как воздух или легкие, будут черными. У мягких тканей относительная рентгеновская плотность может достигать 150 HU, у жировой ткани - ниже 0. Относительная рентгеновская плотность крови после контрастного усиления должна быть около 200-500 HU. В матрице изображения заранее определенного размера (512×512 или 1024×1024) каждый элемент (пиксель) отражает среднее значение рентгеновской плотности ткани в этой локализации, которое может быть показано с использованием шкалы яркости. Поскольку человеческий глаз может дифференцировать только ограниченное количество оттенков серого, параметры электронного окна должны быть настроены таким образом, чтобы показать и дифференцировать интересующие структуры (рис. 6.3).
Рис. 6.3. Аксиальная компьютерная томограмма груди. Аксиальное изображение груди на уровне левой главной венечной артерии. Одно и то же изображение показано с использованием "легочного" окна (используется для оценки паренхимы легкого, А) и "кардиального" окна (используется для оценки сердечных структур, Б). Изображение показано таким образом, как будто мы смотрим на пациента со стороны ног.
КОМПЬЮТЕРНАЯ ТОМОГРАФИЯ СЕРДЦА
СИНХРОНИЗАЦИЯ С ЭКГ
Возможности получения изображения маленьких извилистых и непрерывно двигающихся венечных артерий ограничиваются техническими возможностями современной КТ. Необходимо получить изображения настолько быстро, чтобы "заморозить" движение венечных артерий, при этом все сканирование должно быть выполнено за комфортное время задержки дыхания. Для обнаружения и полуколичественного определения обструкции венечных артерий необходимо высокое пространственное разрешение. Контрастное вещество, вводимое в/в, необходимо для того чтобы отдифференцировать просвет сосуда от его стенки и окружающих тканей, которые имеют сходные коэффициенты ослабления при нативном сканировании.
Возможности продольного сканирования современных 64-срезовых компьютерных томографов недостаточны, для того чтобы получить изображение всего сердца за один сердечный цикл. По этой причине необходимые данные получают в течение нескольких сердечных циклов. Чтобы получить изображения в одной и той же фазе сердечного сокращения, полученные данные или реконструированные изображения должны быть синхронизированы по сердечному ритму. В основном есть два способа сканирования сокращающегося сердца. Пошаговое сканирование с использованием ЭКГ-триггера ("шаг - выстрел") осуществляется с заранее заданной задержкой, которая отсчитывается от предыдущего сердечного сокращения (рис. 6.4). После получения изображения стол перемещается к другой позиции для следующего цикла сканирования. Спиральное сканирование с ЭКГ-синхронизацией комбинирует постоянное движение стола с непрерывным сканированием в течение всего сердечного цикла и синхронной записью ЭКГ (рис. 6.5). Последующая реконструкция изображений осуществляется путем ретроспективного
выбора данных в определенную фазу сокращения сердца из имеющегося полного набора данных на основе записанной ЭКГ (рис. 6.6). Возможность реконструкции изображений в различных фазах сердечного сокращения (поиск фазы с минимальными артефактами от движения), устойчивость к неправильному ритму, возможность редакции данных ЭКГ и способность к реконструкции изображений с перекрытием по толщине делают спиральную КТ с ЭКГ-синхронизацией