

новая папка / Operative Standards for Cancer Surgery Volume I 1st Edition
.pdf12.Homer MJ, Pile-Spellman ER. Needle localization of occult breast lesions with a curved-end retractable wire: technique and pitfalls. Radiology 1986;161(2):547-548.
13.Kopans DB, Meyer JE, Lindfors KK, et al. Breast sonography to guide cyst aspiration and wire localization of occult solid lesions. AJR Am J Roentgenol 1984;143(3):489-492.
14.Landheer ML, Veltman J, van Eekeren R, et al. MRI-guided preoperative wire localization of nonpalpable breast lesions. Clin Imaging 2006;30(4):229-233.
15.Liberman L, Kaplan J, Van Zee KJ, et al. Bracketing wires for preoperative breast needle localization. AJR Am J Roentgenol
2001;177(3):565-572.
16.Kurniawan ED, Wong MH, Windle I, et al. Predictors of surgical margin status in breast-conserving surgery within a breast screening program. Ann Surg Oncol 2008;15(9):2542-2549.
17.Davis PS, Wechsler RJ, Feig SA, et al. Migration of breast biopsy localization wire. AJR Am J Roentgenol 1988;150(4):787-
18.Homer MJ. Transection of the localization hooked wire during breast biopsy. AJR Am J Roentgenol 1983;141(5):929-930.
19.McGhan LJ, McKeever SC, Pockaj BA, et al. Radioactive seed localization for nonpalpable breast lesions: review of 1,000 consecutive procedures at a single institution. Ann Surg Oncol 2011;18(11):3096-3101.
20.van der Ploeg IM, Hobbelink M, van den Bosch MA, et al. ‘Radioguided occult lesion localisation’ (ROLL) for non-palpable breast lesions: a review of the relevant literature. Eur J Surg Oncol 2008;34(1):1-5.
21.Barentsz MW, van Dalen T, Gobardhan PD, et al. Intraoperative ultrasound guidance for excision of non-palpable invasive breast cancer: a hospital-based series and an overview of the literature. Breast Cancer Res Treat 2012;135(1):209-219.
22.Fortunato L, Penteriani R, Farina M, et al. Intraoperative ultrasound is an effective and preferable technique to localize nonpalpable breast tumors. Eur J Surg Oncol 2008;34(12):1289-1292.
23.Lovrics PJ, Cornacchi SD, Vora R, et al. Systematic review of radioguided surgery for non-palpable breast cancer. Eur J Surg Oncol 2011;37(5):388-397.
24.Lovrics PJ, Goldsmith CH, Hodgson N, et al. A multicentered, randomized, controlled trial comparing radioguided seed localization to standard wire localization for nonpalpable, invasive and in situ breast carcinomas. Ann Surg Oncol
2011;18(12):3407-3414.
25. Ngo C, Pollet AG, Laperrelle J, et al. Intraoperative ultrasound localization of nonpalpable breast cancers. Ann Surg Oncol
2007;14(9):2485-2489.
26. Olsha O, Shemesh D, Carmon M, et al. Resection margins in ultrasound-guided breast-conserving surgery. Ann Surg Oncol
2011;18(2):447-452.
27.Rahusen FD, Bremers AJ, Fabry HF, et al. Ultrasound-guided lumpectomy of nonpalpable breast cancer versus wire-guided resection: a randomized clinical trial. Ann Surg Oncol 2002;9(10):994-998.
28.Britton PD SL, Yamamoto AK, Koo B, et al. Breast surgical specimen radiographs: how reliable are they? Eur J Radiol
2011;79(2):245-2459.
29. Cox CE, Furman B, Stowell N, et al. Radioactive seed localization breast biopsy and lumpectomy: can specimen radiographs
be eliminated? Ann Surg Oncol 2003;10(9):1039-1047.
30.Davis KM, Hsu CH, Bouton ME, et al. Intraoperative ultrasound can decrease the re-excision lumpectomy rate in patients with palpable breast cancers. Am Surg 2011;77(6):720-725.
31.Fisher CS, Mushawah FA, Cyr AE, et al. Ultrasound-guided lumpectomy for palpable breast cancers. Ann Surg Oncol
2011;18(11):3198-3203.
32. Silverstein MJ, Lagios MD, Recht A, et al. Image-detected breast cancer: state of the art diagnosis and treatment. J Am Coll Surg 2005;201(4):586-597.
P.15
33. Bathla L, Harris A, Davey M, et al. High resolution intra-operative two-dimensional specimen mammography and its impact on second operation for re-excision of positive margins at final pathology after breast conservation surgery. Am J Surg
2011;202(4):387-394.
34.Ciccarelli G, Di Virgilio MR, Menna S, et al. Radiography of the surgical specimen in early stage breast lesions: diagnostic reliability in the analysis of the resection margins. Radiol Med 2007;112(3):366-376.
35.Jakub JW, Gray RJ, Degnim AC, et al. Current status of radioactive seed for localization of non palpable breast lesions. Am J Surg 2010;199(4):522-528.
36.American Society of Breast Surgeons. Image confirmation of successful excision of image-localized breast lesion. https://www.breastsurgeons.org/new_layout/about/statements/QM/ASBrS_Image_confirmation_of_successful_excision_of_imagelocalized_breast_lesion.pdf. American Society of Breast Surgeons Web site. Accessed March 25, 2015.
37.Molina MA, Snell S, Franceschi D, et al. Breast specimen orientation. Ann Surg Oncol 2009;16(2):285-288.
38.Singh M, Singh G, Hogan KT, et al. The effect of intraoperative specimen inking on lumpectomy re-excision rates. World J Surg Oncol 2010;8:4.
39.Krawczyk JJ, Engel B. The importance of surgical clips for adequate tangential beam planning in breast conserving surgery and irradiation. Int J Radiat Oncol Biol Phys 1999;43(2):347-350.
40.Pezner RD, Tan MC, Clancy SL, et al. Radiation therapy for breast cancer patients who undergo oncoplastic surgery: localization of the tumor bed for the local boost. Am J Clin Oncol 2013;36(6):535-539.
41.Hunter MA, McFall TA, Hehr KA. Breast-conserving surgery for primary breast cancer: necessity for surgical clips to define the tumor bed for radiation planning. Radiology 1996;200(1): 281-282.
42.Dzhugashvili M, Tournay E, Pichenot C, et al. 3D-conformal accelerated partial breast irradiation treatment planning: the value of surgical clips in the delineation of the lumpectomy cavity. Radiat Oncol 2009;4:70.
43.Penninkhof J, Quint S, Boer H, et al. Surgical clips for position verification and correction of non-rigid breast tissue in simultaneously integrated boost (SIB) treatments. Radiother Oncol 2009;90(1):110-115.
P.16
Partial Mastectomy: Key Question
In patients undergoing breast conserving surgery, intraoperative margin assessment will reduce re-excision or positive
margin rates compared to no intraoperative assessment.
INTRODUCTION

The management of breast margins remains important. Although the size of the preferred margin is controversial, what is clear is that positive margins of excision, even with varied definitions, are associated with higher rates of local recurrence. Thus the intraoperative management of breast margins is important in reducing the morbidity, cost, and inefficiency associated with reoperation for inadequate margins. In this chapter, we review the evidence for techniques of intraoperative management of breast cancer margins.
METHODOLOGY
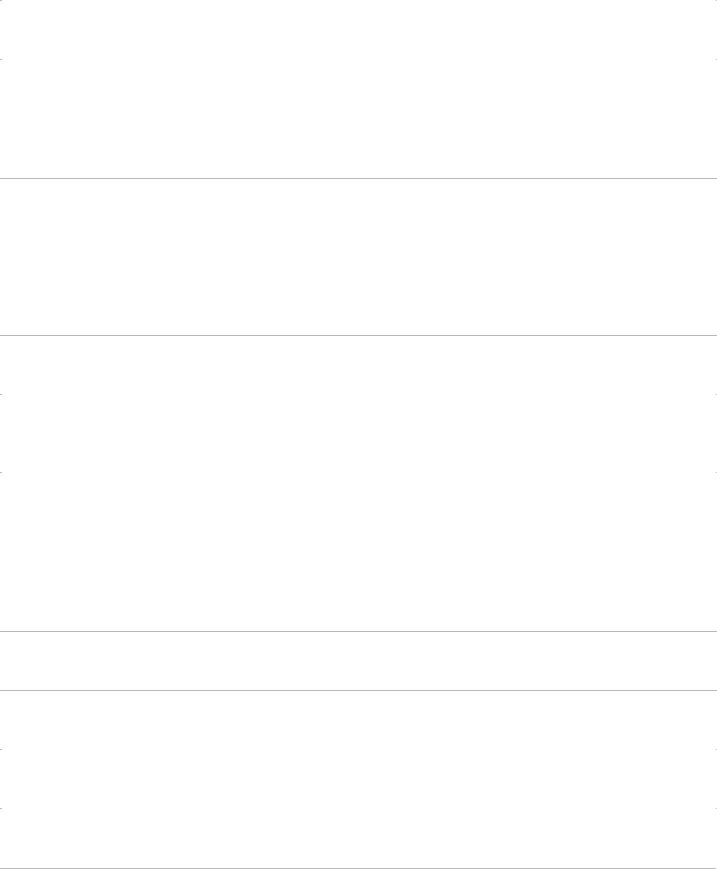
A Medline search was made with the assistance of a professional medical librarian of multiple keywords involving breast neoplasms, breast operations, and intraoperative techniques, including all papers from 1995 through November 2013. Three hundred seventynine abstracts were identified. Ninety-nine of these were duplicates, leaving 280 abstracts for review. The first 50 abstracts were reviewed by four reviewers, who then met to ensure consistent inclusion criteria. The subsequent abstracts and manuscripts were reviewed by one of these four reviewers. Of the abstracts reviewed, 121 had a focus on intraoperative management or techniques that influence margins, including rates of local recurrence, reoperation, and/or inadequate margins of excision. Eighty-six papers were included after the elimination of 35 manuscripts that either had no English language version available, did not truly address intraoperative margin management with actionable data, had too small of a sample size to reach conclusions, or reported redundant data from other included manuscripts (Fig. 1-6).
FINDINGS
Intraoperative Use of Localization Methods: (1) Ultrasound
Ultrasound (US) use intraoperatively to guide excision and/or to evaluate the margin distance in the resected specimen has been associated with a reduced rate of positive margins in randomized and cohort trials (Table 1-1). Two randomized trials and several cohort studies suggest that US be used instead of palpation guidance for palpable tumors among surgeons who have or can develop good US skills (Grade 1B). US-guided excision may also be able to reduce the rate of positive margins compared to wire localization for surgeons skilled in its use,
P.17
but although one randomized trial found such a reduction in re-excision rates, a larger cohort study failed to demonstrate any difference. This combined with fewer studies of US versus wire localization leads us to a less certain recommendation that surgeons skilled in US consider its use as an alternative to wire localization (Grade 2B).
FIGURE 1-6 Flow diagram for selection of publications for inclusion.
Intraoperative Use of Localization Methods: (2) Radioactive Seed Localization
Radioactive seed localization (RSL) has been consistently associated with lower rates of positive margins than wire localization (WL)

in multiple cohort series, metaanalyses, and small randomized controlled trials (Table 1-2). In the largest available randomized trial, however, RSL and WL did not significantly differ in positive margin rates. This trial had an unusually low rate of positive margins in the WL group, and the RSL group had a significantly higher incidence of multifocal disease. The data suggest that the value of RSL as an alternative to wire localization is likely dependent on the rate of inadequate margins of excision with WL. If these rates are near 12% or
P.18
less, there is no advantage in considering RSL (Grade 1B). If these rates are 20% or greater, RSL should be considered as an alternative to WL (Grade 2B).
TABLE 1-1 Intraoperative Localization Methods: Intraoperative Ultrasound
|
Population |
Study |
Type of |
Outcome |
Margin |
|
Author |
Size (n) |
Design |
Intervention |
Measured |
Definition |
Summary of Key Findings |
Rahusen |
49 |
RCT |
Intraoperative |
Margin |
1 mm |
89% adequate margins vs. 59% |
et al, |
|
|
ultrasound |
status, |
|
with wire localization (P = .007). No |
200226 |
|
|
|
volume, |
|
differences in tissue volume or time |
|
|
|
|
and time |
|
of operation. |
Krekel et |
142 |
RCT |
Intraoperative |
Margin |
No ink on |
US reduced positive margin rate (11 |
al, |
|
|
ultrasound |
status and |
tumor |
vs. 28%, P = .031) and total volume |
201327 |
|
|
|
volume |
|
of specimen versus palpation |
|
|
|
|
|
|
guidance. |
Moore et |
51 |
RCT |
Intraoperative |
Margin |
No ink on |
Positive margin rate (3.5% vs. 29%, |
al, |
|
|
ultrasound |
status |
tumor |
P < .05) for palpation-guided |
200128 |
|
|
|
|
|
excision with no intraoperative |
|
|
|
|
|
|
evaluation of margins |
Additional studies: Davis et al, 201129; Olsha et al, 201130; Eichler et al, 201231; Barentsz et al, 201232; Harlow et al,
199933; James et al, 2009.34
RCT, randomized controlled trial; US, ultrasound.
Intraoperative Use of Localization Methods: (3) Radioguided Occult Lesion Localization
Radioguided occult lesion localization (ROLL) is a technique utilized largely by European surgeons that has also been associated with lowered rates of positive margins compared to WL in most studies. However, as with RSL, the largest randomized trial failed to show a difference in positive margin rate, with the WL cohort having only a 12% rate of positive margins (Table 1-3). Thus, if the rates of inadequate margins are near 12% or less with WL, there is no advantage in considering ROLL (Grade 1B), but if these rates are 20% or greater, ROLL should be considered as an alternative to WL (Grade 2B). Only one trial compared RSL and ROLL, and this failed to demonstrate a difference in adequate margin rates between these two techniques.
P.19
TABLE 1-2 Intraoperative Localization Methods: Radioactive Seed Localization
|
Population |
Study |
Type of |
Outcome |
Margin |
Summary of Key |
|
Author |
Size (n) |
Design |
Intervention |
Measured |
Definition |
Findings |
Comments |
Gray et |
97 |
RCT |
RSL |
Final |
1 mm |
Initial specimen |
Randomized |
al, |
|
|
|
margin |
|
had lower rate of |
vs. wire |
200135 |
|
|
|
status |
|
involved margins |
localization |
|
|
|
|
|
|
for RSL patients |
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
(26% vs. 57%, P |
|
|
|
|
|
|
|
= .02), despite the |
|
|
|
|
|
|
|
mean volume |
|
|
|
|
|
|
|
being similar (56 |
|
|
|
|
|
|
|
mL vs. 74 mL, P = |
|
|
|
|
|
|
|
.48). |
|
Lovrics |
305 |
Multicenter |
RSL |
Final |
No ink on |
No significant |
More cases |
et al, |
|
RCT |
|
margin |
tumor for |
difference in |
of multifocal |
201136 |
|
|
|
status |
positive |
positive margin |
disease in |
|
|
|
|
|
and <1 |
rates for RSL |
the RSL |
|
|
|
|
|
mm for |
(11%) and WL |
group (15% |
|
|
|
|
|
close |
(12%, P = .99) or |
vs. 6%; P |
|
|
|
|
|
|
for positive or |
=.013) |
|
|
|
|
|
|
close margins |
|
|
|
|
|
|
|
(RSL 19% and |
|
|
|
|
|
|
|
WL 22%; P =.61). |
|
|
|
|
|
|
|
Mean operative |
|
|
|
|
|
|
|
time (min) was |
|
|
|
|
|
|
|
shorter for RSL |
|
|
|
|
|
|
|
(19 vs. 22; P |
|
|
|
|
|
|
|
<.001). Specimen |
|
|
|
|
|
|
|
volume, weight, |
|
|
|
|
|
|
|
reoperation, and |
|
|
|
|
|
|
|
localization times |
|
|
|
|
|
|
|
were similar. |
|
Ahmed |
8 studies |
Meta- |
RSL |
Final |
Not stated |
RSL had lower |
1 RCT and |
et al, |
|
analysis |
|
margin |
|
risk of positive |
7 cohort |
201337 |
|
|
|
status and |
|
margins (OR, |
studies |
|
|
|
|
spec |
|
0.51; 95% CI, |
compared to |
|
|
|
|
volume |
|
0.36-0.72; z = |
wire |
|
|
|
|
|
|
3.88; P = .0001); |
localization |
|
|
|
|
|
|
reoperation for |
|
|
|
|
|
|
|
margins (OR, |
|
|
|
|
|
|
|
0.47; 95% CI, |
|
|
|
|
|
|
|
0.33-0.69; z = |
|
|
|
|
|
|
|
3.96; P < .0001) |
|
|
|
|
|
|
|
and shorter |
|
|
|
|
|
|
|
operative time |
|
Additional studies: Cox et al, 200339; Gobardhan et al, 201340; Gray et al, 200441; Hughes et al, 200842; Murphy et al,
201343; Donker et al, 2013.44
CI, confidence interval; OR, odds ratio; RCT, randomized controlled trial; RSL, radioactive seed localization; WL, wire localization.
P.20
TABLE 1-3 Intraoperative Localization Methods: Radioguided Occult Lesion Localization (ROLL)
|
Population |
Study |
Type of |
Outcome |
Margin |
Summary of Key |
|
Author |
Size (n) |
Design |
Intervention |
Measured |
Definition |
Findings |
Comments |
Postma |
314 |
RCT |
ROLL |
Final margin |
No ink on |
Positive margins |
|
|
|
|
|
|
|
|
|

et al, |
|
|
|
status, |
tumor |
among 14% of |
201345 |
|
|
|
complication, |
|
ROLL patients vs. |
|
|
|
|
and cost |
|
12% of WL (P = |
|
|
|
|
|
|
.644). Total costs |
|
|
|
|
|
|
were similar for |
|
|
|
|
|
|
ROLL and WL |
|
|
|
|
|
|
(+26 per patient, |
|
|
|
|
|
|
95% CI -250 to + |
|
|
|
|
|
|
311). The risk of |
|
|
|
|
|
|
complications was |
|
|
|
|
|
|
higher for ROLL |
|
|
|
|
|
|
than for WL (30% |
|
|
|
|
|
|
vs. 17%, P = |
|
|
|
|
|
|
.006). |
Medina- |
16 |
RCT |
ROLL |
Final margin |
Not stated |
Negative margins |
Franco |
|
|
|
status |
|
were achieved in |
et al, |
|
|
|
|
|
89% vs. 63% for |
200846 |
|
|
|
|
|
WL (P = .04) |
Sajid et |
449 |
Meta- |
ROLL |
Final margin |
Variable |
Lower risk of |
al, |
|
analysis |
|
status, |
|
positive margin |
201247 |
|
of 4 |
|
complication, |
|
with ROLL vs. WL |
|
|
RCTs |
|
and volume |
|
(OR, 0.47; 95% |
|
|
|
|
of tissue |
|
CI, 0.22-0.99; z = |
|
|
|
|
|
|
1.99; P <.05). |
Surgical time less with ROLL (P <.00001). The weight of the specimen is similar (P = .27).
Additional studies: Audisio et al, 200548; Belloni et al, 201149; Duarte et al, 200750; Lavoue et al, 200851; Nadeem et al, 200552; Zgajnar et al, 200553; Donker et al, 2013.44
CI, confidence interval; OR, odds ratio; RCT, randomized controlled trial; ROLL, radioguided occult lesion localization; WL, wire localization.
P.21
Intraoperative Pathology
(1) Gross exam
There are only a few, relatively small studies of limited quality that examine the effect of gross pathologic examination of a specimen intraoperatively on positive margin rates.1,2,3 The limited data available, however, suggests that gross pathology likely lowers the rate of reoperation for margins and should be considered where intraoperative pathology is available (Grade 2B). One trial showed that intraoperative inking of the specimen resulted in fewer reoperations when compared to postoperative inking,4 but there is too little data to make a recommendation for this technique.
(2) Frozen section analysis
Most surgeons do not use frozen section analysis for margin management.5 No randomized trial has been performed on frozen section analysis, but a large number of cohort trials have consistently shown that this technique is associated with a lower rate of reoperations for inadequate margins (Table 1-4). Because frozen section analysis involves added cost, its cost-effectiveness necessarily depends on the rate of positive margins (and therefore reoperations) without its use. Frozen section analysis has been shown to be cost-effective when positive margin rates are >25%. Based purely on the effect on margin management, frozen section

analysis should be considered unless reoperation rates are already low (<15%) (Grade 2B).
(3) Imprint cytology
Few surgeons ultilize imprint cytology intraoperatively.5 Like frozen section analysis, no randomized trial has shown this technique to improve the rates of positive margins, but a number of cohort trials have demonstrated that imprint cytology is associated with lower rates of positive margins and perhaps lower local recurrence risk (Table 1-4). Imprint cytology is dependent on the availability of cytology expertise. When such expertise is available, imprint cytology should be considered for intraoperative margin management (Grade 2C) and appears to be at least as reliable as intraoperative frozen section analysis (Grade 2C).
Cavity Shave Margins
Cavity shave margins is a technique of resecting an additional margin of tissue at each of the margins intraoperatively (or in some cases, selected margins) after excision of the main lumpectomy specimen for postoperative pathologic evaluation. Cavity shave margins have been associated with a lower rate of positive margins in multiple cohort studies, but many of these trials had a high rate of positive margins in the control group (Table 1-5). Cavity shave margins should be considered to reduce the rate of positive margins in breast-conserving surgery if the rate of positive margins is otherwise >25% (Grade 2C) and may be particularly valuable where intraoperative pathology is unavailable.
Specimen Radiography
The use of specimen radiography does not clearly improve the rates of reoperation for margins.3,6,7,8,9,10,11,12 Specimen radiography may be helpful in judging the adequacy of
P.22
P.23
P.24
P.25
margins of excision for lesions associated with microcalcifications. The addition of specimen radiography for the purpose of improving the rates of inadequate margins of excision cannot currently be recommended based on the available evidence (Grade 2C) but remains important for documenting removal of the targeted lesion.
TABLE 1-4 Intraoperative Pathology Methods and Margins
|
Population |
Study |
Type of |
Outcome |
Margin |
Summary of |
|
Author |
Size (n) |
Design |
Intervention |
Measured |
Definition |
Key Findings |
Comments |
Esbona |
37 cohort |
Systematic |
Frozen |
Margin |
Not |
The reoperation |
No |
et al, |
studies; |
review |
section |
status |
defined |
rate for margins |
difference |
201254 |
10,489 |
|
analysis and |
|
|
with frozen |
in |
|
tumors |
|
imprint |
|
|
section analysis |
reoperation |
|
|
|
cytology vs. |
|
|
(10 ± 6%) was |
rate, |
|
|
|
permanent |
|
|
significantly |
sensitivity, |
|
|
|
histology |
|
|
lower than with |
or |
|
|
|
|
|
|
permanent |
specificity |
|
|
|
|
|
|
histology only |
of frozen |
|
|
|
|
|
|
(35 ± 3%, P = |
section vs. |
|
|
|
|
|
|
.0001). The |
imprint |
|
|
|
|
|
|
final re-excision |
cytology |
|
|
|
|
|
|
rate of IC (11 ± |
|
|
|
|
|
|
|
4%) was also |
|
|
|
|
|
|
|
significantly |
|
|
|
|
|
|
|
lower than |
|
|
|
|
|
|
|
control (35 ± |
|
|
|
|
|
|
|
3%, P = .001). |
|
Osborn |
N/A |
Mathematical |
Frozen |
Cost of |
Not stated |
The cost to the |
Compared |
et al, |
|
modeling |
section |
frozen |
|
provider is less |
to |
201155 |
|
|
analysis |
section |
|
by doing |
permanent |

|
|
|
|
analysis |
|
intraoperative |
histology |
|
|
|
|
strategy |
|
frozen section |
only |
|
|
|
|
|
|
analysis when |
|
|
|
|
|
|
|
the reoperation |
|
|
|
|
|
|
|
rate was >36% |
|
|
|
|
|
|
|
without frozen |
|
|
|
|
|
|
|
section. The |
|
|
|
|
|
|
|
cost to the |
|
|
|
|
|
|
|
payer was less |
|
|
|
|
|
|
|
when the re- |
|
|
|
|
|
|
|
excision rate |
|
|
|
|
|
|
|
was >26%. |
|
Camp |
257 |
Case series |
Frozen |
Margin |
2 mm |
Reoperation |
|
et al, |
|
|
section |
status and |
|
rate for margins |
|
200556 |
|
|
analysis of |
LR |
|
5.8% vs. 33% |
|
|
|
|
shave |
|
|
without frozen |
|
|
|
|
margins |
|
|
section of shave |
|
|
|
|
|
|
|
margins (P = |
|
|
|
|
|
|
|
.001). No |
|
difference in LR rates.
Additional studies: Caruso et al, 201163; Cendan et al, 200564; Chen et al, 201265; Noguchi et al, 199566; Riedl et al, 200967; Weber et al, 199768; Cox et al, 199769; Creager et al, 200270; Mannell, 200571; Valdes et al, 2007.72
IC, imprint cytology; LR, local recurrence.
TABLE 1-5 Intraoperative Cavity Shave Margins
|
|
|
|
|
|
Summary of |
|
|
Population |
Study |
Type of |
Outcome |
Margin |
Key |
|
Author |
Size (n) |
Design |
Intervention |
Measured |
Definition |
Findings |
Comments |
Fukamachi |
122 |
Case |
Cavity shave |
Final |
5 mm |
Decreased |
Time of |
et al, 201073 |
|
series |
margins with |
margin |
|
positive |
process |
|
|
|
frozen |
status |
|
margin rate |
was mean |
|
|
|
section |
|
|
from 27% to |
of 53 |
|
|
|
|
|
|
10% (P |
minutes. |
|
|
|
|
|
|
<.001). |
|
|
|
|
|
|
|
Frozen |
|
|
|
|
|
|
|
section |
|
|
|
|
|
|
|
sensitivity |
|
|
|
|
|
|
|
78.6%, |
|
|
|
|
|
|
|
specificity |
|
|
|
|
|
|
|
100%, PPV |
|
|
|
|
|
|
|
100%, NPV |
|
|
|
|
|
|
|
94%, 0% LR |
|
|
|
|
|
|
|
rate over |
|
|
|
|
|
|
|
61.4 months. |
|
Janes et al, |
217 |
Case |
Superior and |
Final |
5 mm = |
Close |
Compared |
200674 |
|
series |
inferior cavity |
margin |
close |
margins |
to group |
|
|
|
shave |
status |
|
reduced: OR |
with cavity |
|
|
|
|
|
|
|
|

|
|
|
margins |
|
|
0.17 (95% CI |
shaves |
|
|
|
|
|
|
0.08-0.48, P |
based on |
|
|
|
|
|
|
= .001). |
specimen |
|
|
|
|
|
|
|
radiograph |
Hequet et al, |
294 |
Multicenter |
Cavity shave |
Final |
2 mm |
25% rate of |
|
201375 |
|
cohort |
margins |
margin |
|
reoperation |
|
|
|
|
|
status |
|
for margins. |
|
|
|
|
|
|
|
Cavity |
|
|
|
|
|
|
|
shaving |
|
|
|
|
|
|
|
avoided the |
|
|
|
|
|
|
|
need for |
|
|
|
|
|
|
|
reexcision in |
|
|
|
|
|
|
|
25%. LR rate |
|
|
|
|
|
|
|
3.7% after |
|
|
|
|
|
|
|
follow-up |
|
|
|
|
|
|
|
range of 4-9 |
|
|
|
|
|
|
|
years. |
|
Hewes et al, |
957 |
Case |
Cavity shave |
Final |
1 mm |
Concordance |
|
200976 |
|
series |
margins |
margin |
|
between |
|
|
|
|
|
status, LR, |
|
original |
|
|
|
|
|
and OS |
|
resection |
|
|
|
|
|
|
|
margins and |
|
|
|
|
|
|
|
cavity biopsy |
|
|
|
|
|
|
|
was only |
|
|
|
|
|
|
|
32%; a |
|
|
|
|
|
|
|
negative |
|
|
|
|
|
|
|
margin |
|
|
|
|
|
|
|
carried an |
|
|
|
|
|
|
|
11% risk of |
|
|
|
|
|
|
|
residual |
|
|
|
|
|
|
|
disease. |
|
|
|
|
|
|
|
Positive |
|
|
|
|
|
|
|
cavity biopsy |
|
|
|
|
|
|
|
associated |
|
|
|
|
|
|
|
with reduced |
|
|
|
|
|
|
|
OS and |
|
|
|
|
|
|
|
DSS. LR rate |
|
|
|
|
|
|
|
was 1.8% 5 |
|
|
|
|
|
|
|
years. |
|
Kobbermann |
533 |
Matched |
Cavity shave |
Final |
2 mm |
Reoperation |
|
et al, 201178 |
|
cohort |
margins |
margin |
|
rate for |
|
|
|
|
|
status |
|
margins was |
|
|
|
|
|
|
|
22% for |
|
|
|
|
|
|
|
cavity shave |
|
|
|
|
|
|
|
margin |
|
|
|
|
|
|
|
patients vs. |
|
|
|
|
|
|
|
42.0% in a |
|
|
|
|
|
|
|
match cohort |
|
|
|
|
|
|
|
(P = .011). |
|
Malik et al, |
543 |
Case |
Cavity shave |
Final |
No ink on |
Shave |
|
199979 |
|
series |
margins |
margin |
tumor |
margins |
|
|
|
|
|
status |
|
positive in |
|
|
|
|
|
|
|
37%. |
|
|
|
|
|
|
|
Reoperation |
|
|
|
|
|
|
|
needed in |
|

|
|
|
|
|
|
15%. LR rate |
|
|
|
|
|
|
2% at |
|
|
|
|
|
|
median 53 |
|
|
|
|
|
|
months. |
Rizzo et al, |
320 |
Case |
Cavity shave |
Final |
1 mm |
Negative |
201080 |
|
series |
margins |
margin |
|
margin rate |
|
|
|
|
status and |
|
was 85% |
|
|
|
|
LR |
|
with addition |
|
|
|
|
|
|
of cavity |
|
|
|
|
|
|
shave |
|
|
|
|
|
|
margins vs. |
|
|
|
|
|
|
57% for |
|
|
|
|
|
|
patients that |
|
|
|
|
|
|
did not (P |
|
|
|
|
|
|
<.05). |
Tengher- |
107 |
Case |
Cavity shave |
Final |
3 mm |
Shave |
Barna et al, |
|
series |
margins |
margin |
|
margins |
200981 |
|
|
|
status |
|
positive in |
|
|
|
|
|
|
35% and |
prevented reoperation in 20%. 30% reoperation rate for margins.
CI, confidence interval; LR, Local recurrence; NPV, negative predictive value; OS, overall survival; PPV, positive predictive value.
MISCELLANEOUS TECHNIQUES
Individual trials have investigated the use of intraoperative magnetic resonance imaging and cryo-assisted localization,13,14 and there are several reports in the literature of emerging technologies to assess margins in a more comprehensive or automated
fashion.15,16,17,18,19,20,21,22,23 The Marginprobe device was recently approved for use in the United States, and although it did not reduce overall reoperation rates (including mastectomy), its use significantly reduced lumpectomy re-excision rates with a larger
effect in nonpalpable tumors.24,25 There is insufficient evidence to make recommendations regarding these techniques and devices.
CONCLUSIONS
Surgeons have many intraoperative tools available to help lower the rates of positive margins of excision among breast cancer patients. Although the available literature for these tools is often not of the highest quality, the accumulated evidence provides substantial guidance as to which techniques are best applied and will have the most impact on a given surgeon’s breast cancer practice. This evidence is especially helpful in devising alternative or adjuvant strategies that can be applied and should be considered if reoperation rates are significant (i.e., ≥20%).
REFERENCES
1.Balch GC, Mithani SK, Simpson JF, et al. Accuracy of intraoperative gross examination of surgical margin status in women undergoing partial mastectomy for breast malignancy. Am Surg 2005;71(1):22-27; discussion 27-28.
2.Fleming FJ, Hill AD, McDermott EW, et al. Intraoperative margin assessment and re-excision rate in breast conserving surgery. Eur J Surg Oncol 2004;30(3):233-237.