

456 CHAPTER 10 Trauma to the urinary tract
Penile injuries
Penile fracture
This involves rupture of the tunica albuginea of the erect penis (i.e., rupture of one or both corpora cavernosa and/or rupture of the corpus spongiosum and urethra). The tunica albuginea is 2 mm thick in the flaccid penis and thins to 0.25 mm during erection, which makes it vulnerable to rupture if the penis is forcibly bent (e.g., during vigorous sexual intercourse).
In general, the diagnosis of penile fracture is straightforward and based on the presence of classic history and physical findings. Delay in diagnosis is common, as many men are initially too embarrassed, ashamed, or frightened to present immediately for medical attention. Penile imaging is not needed to diagnose penile fracture, although MRI has been reported to be accurate in equivocal cases.
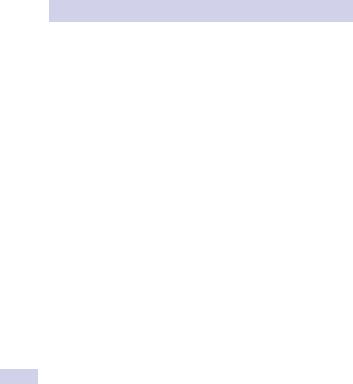
The patient usually reports a sudden “snapping” sound or “popping” sensation, with sudden penile pain and detumescence of the erection. The penis immediately becomes markedly swollen and bruised, a classic appearance known as the “eggplant” deformity (Fig. 10.16).
A tender, palpable defect may be felt over the site of the tear in the tunica albuginea. If Buck fascia has ruptured, bruising extends onto the lower abdominal wall and into the perineum and scrotum; otherwise, the discoloration is contained along the penile shaft.
If the urethra is damaged, there may be blood at the meatus or hematuria (dipstick/microscopic or macroscopic) and pain on voiding or urinary retention. Arrange a retrograde urethrogram or flexible cystoscopy in such cases. Immediate primary urethral repair is warranted for concomitant urethral injuries.
Treatment
Immediate surgical repair has been repeatedly associated with a lower complication rate (e.g., reduced impotence, penile deformity and scar tissue formation, prolonged penile pain) than that of conservative treatment of penile fracture.
The fracture site in the tunica albuginea is exposed via a circumcision incision, the hematoma evacuated, and the defect in the tunica closed with interrupted 2–0 absorbable sutures. Deep stitches in the underlying erectile tissue are unnecessary and possibly harmful; only tunical closure is warranted.
A self-adhesive compressive bandage, application of cold compresses to the penis, analgesics and anti-inflammatory drugs, and abstinence from sexual activity for 6–8 weeks are prudent adjunct measures to promote optimal healing.
Surgical repair of penile fracture
Expose the fracture site by degloving the penis via a circumcising incision around the subcoronal sulcus or by an incision directly over the defect if palpable. A degloving incision allows better exposure of the urethra for associated urethral injuries.
Alternatively, use a midline incision extending distally from the midline raphe of the scrotum, along the shaft of the penis. This latter incision,
PENILE INJURIES 457
A
B
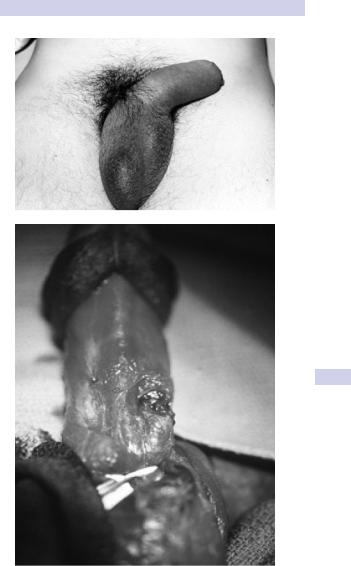
Figure 10.16 A) Typical “eggplant deformity” appearance of fractured penis. B) Intraoperative appearance of penile fracture—a transverse defect in the tunica albuginea in the midshaft.
458 CHAPTER 10 Trauma to the urinary tract
along with a degloving incision, allows excellent exposure of both corpora cavernosa so that an unexpected bilateral injury can be repaired easily, as can a urethral injury should this have occurred.
Close the defect in the tunica albuginea with absorbable 2–0 sutures. Cover the knots with Buck fascia or bury them so that the patient is unable to palpate them. Leave a urethral catheter overnight (voiding can be difficult immediately postoperatively). Repair a urethral rupture, if present, with a spatulated single or two-layer urethral anastomosis, and splint repair with a urethral catheter for 2 weeks.
Amputation
Place the amputated penile remnant, if found, in a wet gauze pad inside a plastic bag, which is then placed inside another bag containing ice (bag in a bag). It can survive for 24 hours.
Blood loss can be severe; resuscitate the shocked patient and crossmatch blood. Consider psychiatric consultation if the wound was selfinflicted.
Knife and gunshot wounds
Associated injuries are common (e.g., scrotum, major vessels of the lower limb). Most corporal injuries, other than minor ones, should undergo primary repair to prevent long-term disturbance of erectile function.
Remove debris from wound (e.g., particles of clothing) and débride necrotic tissue sparingly. Repair as for penile fractures (see Box 10.7).
PENILE INJURIES 459
Box 10.7 Treatment of penile injuries
Surgical reimplantation of amputated penis
Repair the urethra first, over a catheter, to provide a stable base for subsequent neurovascular repair. Concomitant suprapubic urinary diversion is usually recommended. Close the tunica albuginea of the corpora with 2–0 absorbable sutures.
Cavernosal artery repair is not recommended, since it is technically very difficult and does not improve penile viability.
Microsurgical anastomosis (via plastic surgical consultation) is then performed on the dorsal artery of the penis, the dorsal vein to provide venous drainage, and, finally, the dorsal penile nerve and skin. In the absence of microsurgical expertise availability, a “macroreplantation” of the urethra, corpora, and skin is acceptable.
Penile bites and skin loss injuries
Clean the wound copiously. Give broad-spectrum antibiotics (e.g., cephalosporin and amoxycillin). If skin loss has occurred via degloving injury, a loose primary closure with 3–0 chromic is recommended.
Zipper injuries
If the penis is still caught in the zipper, use lubricant jelly and gently attempt to open it. The zipper bar may have to be cut with orthopedic cutters or pried apart with a pair of surgical clamps on either side of the zipper.