


470 CHAPTER 11 Infertility
Etiology and evaluation of male infertility
Definition of infertility
Infertility is failure of conception after at least 12 months of unprotected intercourse. The chance of a normal couple conceiving is estimated at 20–25% per month, 75% by 6 months, and 90% at 1 year. Up to 50% of infertility is due to male factors. Up to 25% of couples may be affected at some point in their reproductive years.
Pathophysiology
Failure of fertilization of the normal ovum is due to defective sperm development, function, or inadequate numbers. There may be abnormalities of morphology (teratospermia) or motility (asthenospermia), low sperm numbers (oligospermia), combined disorders (oligoasthenospermia), or absent sperm (azoospermia).
Abnormal epididymal function may result in defective spermatozoa maturation or transport, or induce cell death.
Etiology
•Idiopathic (25%)
•Varicocele (present in 40%)
•Cryptorchidism (undescended testes)
•Functional sperm disorders: immunological infertility (sperm antibodies); head or tail defects; Kartagener’s syndrome (immotile cilia); dyskinetic cilia syndrome
•Erectile or ejaculatory problems
•Testicular injury: orchitis (postpubertal, bilateral mumps orchitis); testicular torsion; trauma; radiotherapy
•Endocrine disorders: Kallmann’s syndrome (isolated gonadotrophin deficiency causing hypogonadism and anosmia); Prader–Willi syndrome (hypogonadism, short stature, hyperphagia, obesity); pituitary gland adenoma, radiation, or infection
•Hormone excess: excess prolactin (pituitary tumor); excess androgen (adrenal tumor, congenital adrenal hyperplasia, anabolic steroids); excess estrogens
•Genetic disorders: Kleinfelter’s syndrome (47XXY) involves azoospermia, iFSH/LH AND dtestosterone; XX male; XYY syndrome
•Male genital tract obstruction: congenital absence of vas deferens; epididymal obstruction or infection; Müllerian prostatic cysts; groin or scrotal surgery
•Systemic disease: renal failure; liver cirrhosis; cystic fibrosis
•Drugs: chemotherapy; alcohol; marijuana; sulfasalazine; smoking
•Environmental factors: pesticides; heavy metals; hot baths

ETIOLOGY AND EVALUATION OF MALE INFERTILITY 471
History
•Sexual: duration of problem; frequency and timing of intercourse; previous successful conceptions; previous birth control; erectile or ejaculatory dysfunction
•Developmental: age at puberty; history of cryptorchidism; gynecomastia
•Medical and surgical: detailed assessment for risk factors—recent febrile illness; postpubertal mumps orchitis; varicocele; testicular torsion, trauma, or tumor; sexually transmitted diseases; genitourinary surgery; radiotherapy; respiratory diseases associated with ciliary dysfunction; diabetes
•Drugs and environmental: previous chemotherapy; exposure to substances that impair spermatogenesis or erectile function; alcohol consumption; smoking habits; hot baths
•Family: hypogonadism; cryptorchidism
Examination
Perform a full assessment of all systems, with attention to general appearance (evidence of secondary sexual development; signs of hypogonadism; gynecomastia).
Urogenital examination should include assessment of the penis (Peyronie’s plaque, phimosis, hypospadias); measurement of testicular consistency, tenderness, and volume with a Prader orchidometer (normal >20 mL; varies with race); palpation of epididymis (tenderness, swelling) and spermatic cord (vas deferens present or absent, varicocele); and digital rectal examination of the prostate.
472 CHAPTER 11 Infertility
Lab investigation of male infertility
Basic investigations
Semen analysis
Obtain 2 or 3 specimens over several weeks, collected after 2–7 days of sexual abstinence. Deliver specimens to the laboratory within 1 hour. Ejaculate volume, liquefaction time, and pH are noted (Table 11.1).
Microscopy techniques measure sperm concentration, total numbers, morphology, and motility (Table 11.2).
The mixed agglutination reaction (MAR test) is used to detect antiperm antibodies. The presence of leukocytes or round cells in the ejaculate (>1 x 106/mL of semen) suggests infection, and cultures should be requested.
Hormone measurement
Obtain serum FSH, LH, and testosterone (Table 11.3). Elevated serum FSH levels (2 x normal) suggest irreversible testicular failure. In cases of isolated low testosterone level, it is recommended that morning and free testosterone levels be tested.
Elevated prolactin is associated with sexual dysfunction and low serum testosterone levels, and usually indicates the presence of a pituitary adenoma.
Special investigations
•Chromosome analysis is indicated for clinical suspicion of an abnormality (azoospermia or oligospermia, small atrophic testes with iFSH).
•Fructose is produced in the seminal vescle and is a major source of energy for sperm metabolism. If semen fructose is low, an ejaculatory duct obstruction or seminal vesical abnormality should be suspected.
•Testicular biopsy is performed for azoospermic patients with normal FSH levels, to differentiate between idiopathic (e.g., maturation arrest, Sertoli cell only syndrome) and obstructive causes. It may also be used for sperm retrieval.
Sperm function tests
Postcoital test
Cervical mucus is taken just before ovulation and within 8 hours of intercourse, and microscopy is performed. Normal results shows >10 sperm per high-powered field, the majority demonstrating progressive motility. Abnormal results indicate inappropriate timing of the test; cervical mucus antisperm antibodies; abnormal semen; or inappropriately performed coitus.
Sperm penetration test
A sample of semen is placed directly onto preovulatory cervical mucus on a slide and the penetrative ability of spermatozoa is observed.
Sperm-cervical mucus test
A specimen of semen (control) and one mixed with cervical mucus are placed separately on a slide and observed for 30 minutes. More than 25% exhibiting jerking movements in the mixed sample (but not the control) is a positive test for antisperm antibodies.
|
|
LAB INVESTIGATION OF MALE INFERTILITY |
473 |
|
|
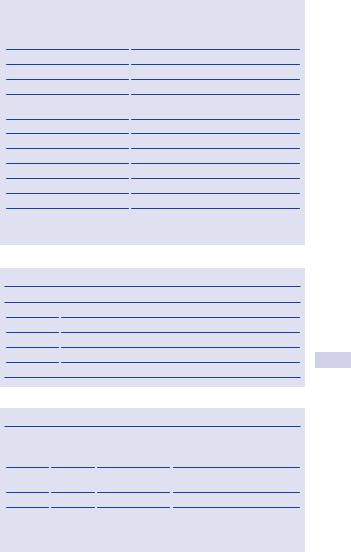
Table 11.1 Semen analysis: normal parameters* |
|||
|
|
|
|
|
|
Semen analysis |
Normal values |
||
|
|
|
|
|
|
Semen volume |
>2.0 mL |
||
|
pH |
7.2–7.8 |
||
|
Total sperm count |
>40 x106/ejaculate |
||
|
Sperm concentration |
>20 x106/mL |
||
|
Sperm motility |
>50% with progressive motility (grades >2); |
||
|
|
or >25% grade 4 |
||
|
Sperm morphology |
>15% normal forms |
||
|
Viability |
>75% viable sperm |
||
|
Time to liquefy |
5–25 minutes |
||
|
White blood cells |
<1 x106 WBC/mL |
||
|
MAR test (for antisperm Ab) |
Negative (<10% with adherent particles) |
||
|
Zinc |
>2.4 mol/ejaculate |
||
|
Semen fructose |
120–145 mg/dL |
||
|
|
|
|
|
*Adapted from World Health Organization (WHO) reference values for semen analysis.
Table 11.2 Grading of sperm motility
Grade |
Type of sperm motility |
0No motility
1Sluggish; no progressive movement
2Slow, meandering forward progression
3Moving in a straight line with moderate speed
4Moving in a straight line at high speed
Table 11.3 Clinical diagnosis on hormone assay
FSH* |
LH** |
Testosterone |
Diagnosis |
i |
Normal |
Normal |
Seminiferous tubule damage |
|
|
|
(defective spermatogenesis) |
Normal |
Normal |
Normal |
Normal; or bilateral genital tract |
|
|
|
obstruction |
i |
i |
Normal/d |
Testicular failure |
d |
d |
d |
Hypogonadotrophism |
|
|
|
|
* Follicle stimulation hormone. ** Luteinizing hormone.

474 CHAPTER 11 Infertility
Imaging
Scrotal ultrasound
This is used to confirm a varicocele and assess testicular abnormalities.
Transrectal ultrasound
TRUS is indicated for low ejaculate volumes, to investigate seminal vesicle obstruction (>1.5 cm width) or absence and ejaculatory duct obstruction (>2 .3 mm).
Vasography
Vas deferens is punctured at the level of the scrotum and injected with contrast toward the prostate, never toward the epdidymis. Vasography is performed at the time of planned reconstruction.
A normal test shows the passage of contrast along the vas deferens, seminal vesicles, ejaculatory duct, and into the bladder, which rules out obstruction—indigo carmine is commonly used to confirm patency.
Formal radiographic vasography is only indicated to localize obstructions proximal to the inguinal ring.
Venography
This is used to diagnose and treat varicoceles (embolization).
This page intentionally left blank