

216 CHAPTER 6 Urological neoplasia
Management of localized prostate cancer: watchful waiting and active surveillance
More men die with prostate cancer than because of it, as most prostate cancers are slow growing and the majority of men diagnosed are often older with limited life expectancies, often with competing morbidities. This scenario forms the basis for less aggressive approaches to prostate cancer; some men diagnosed with nonmetastatic prostate cancer are offered no initial treatment.
Watchful waiting is based on the premise that some patients will not benefit from definitive treatment of the primary prostate cancer. The decision is made at the time of diagnosis to forgo definitive treatment and to instead provide palliative treatment for local or metastatic progression if and when it occurs.
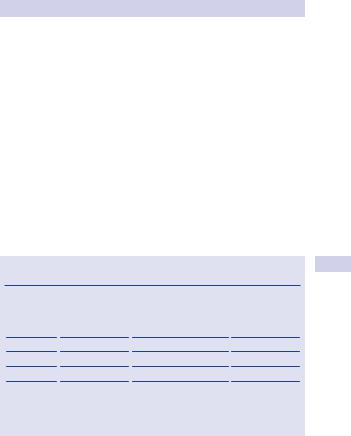
The risks of developing metastatic disease and of death due to prostate cancer after 10–15 years of watchful waiting can be considered using published data, according to biopsy grade. Table 6.4 summarizes these data.
In contrast, active surveillance is based on the concept that some, but not all, patients may derive benefit from treatment of their primary prostate cancer. There are several international trials attempting to answer this question, which will take many years to complete.
The goals of active surveillance are to provide definitive treatment for men with localized cancers that are likely to progress and to reduce the risk of treatment-related complications for men with cancers that are not likely to progress.
Advantages of active surveillance include avoidance of possible side effects and costs of definitive therapy that may be unnecessary, and maintaining quality of life.
Disadvantages include possibly missing an opportunity for cure, the risk of progression and/or metastases, increased anxiety, increased physician visits and tests, and causing subsequent treatment to be more aggressive.
Selection of patients for active surveillance and suggested protocols
There are many different opinions on the best approach to active surveillance. The following represents guidelines from the National Comprehensive Cancer Network (NCCN).1
Characteristics of the patient and disease state for whom active surveillance may be considered are the following:
•Low risk prostate cancer (T1–T2a and Gleason 2–6 and PSA <10 ng/ mL) regardless of life expectancy
•Intermediate risk prostate cancer T2b–T2c or Gleason 7 or PSA 10–20 ng/mL with <10 year life expectancy
1 National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Prostate Cancer V.2.2009. Available at: www.nccn.org (registration required).
MANAGEMENT OF LOCALIZED PROSTATE CANCER 217
Surveillance protocol (if life expectancy <10 years follow up may be less frequent) is as follows:
•Patients must have clinically localized disease and be candidates for definitive treatment and choose observation.
•DRE and PSA as often as every 6 months but at least every 12 months
•Repeat prostate needle biopsy within 6 months of diagnosis if initial biopsy was <10 cores
•Needle biopsy may be performed within 18 months if >10 cores obtained initially, then done periodically.
Cancer progression may have occurred if
•Primary Gleason grade 4 or 5 cancer is found on repeat prostate biopsy.
•Prostate cancer is found in a greater number of prostate biopsies or occupies a greater extent of prostate biopsies.
•PSA doubling time is <3 years or PSA velocity is >0.75.
•A repeat prostate biopsy is indicated for signs of disease progression by exam or PSA.
Table 6.4 Natural history of localized prostate cancer managed with no initial treatment
Biopsy |
% Risk of |
% Risk of prostate1 |
Estimated lost |
grade |
metastasis |
cancer death |
years of life |
|
(10 years) |
(15 years) |
|
|
|
|
|
2–4 |
19 |
4–7 |
<1 year |
5 |
42 |
6–11 |
4 |
6 |
42 |
18–30 |
4 |
7 |
42 |
42–70 |
5 |
8–10 |
74 |
56–87 |
6–8 |
|
|
|
|
1 Albertsen PC, Hanley JA, Gleason DF, et al. (1998). Competing risk analysis of men aged 55 to 74 years at diagnosis managed conservatively for clinically localized prostate cancer. JAMA 280:975–980.
218 CHAPTER 6 Urological neoplasia
Management of localized prostate cancer: radical prostatectomy
Radical (total) prostatectomy (RP) is excision of the entire prostate, including the prostatic urethra, with the seminal vesicles. It may be performed by open retropubic, perineal, laparoscopic, or robotically assisted laparoscopic approaches.
At most U.S. centers, the robotically assisted technique has replaced the laparoscopic approach. The perineal approach does not allow a simultaneous pelvic lymph node dissection and is also not commonly performed in the United States.
Following excision of the prostate, reconstruction of the bladder neck and vesicourethral anastomosis completes the procedure.
RP is indicated for the treatment of men in good health with localized prostate cancer whose life expectancy exceeds 10 years, with curative intent. The indications of radical prostatectomy have been expanded as benefits to the multimodality approach to prostate cancer have become more accepted. As an example, the use of adjuvant radiation therapy following radical prostatectomy with positive surgical margins has allowed more patients with clinical non-organ-confined disease to be offered this surgical option.
Patients with Gleason score 2–4 disease appear to do as well with watchful waiting as with any other treatment. The patient should consider all available treatment options and the complications of RP prior to proceeding.
The surgeon should take part in multidisciplinary team discussion of each case. The most recent AUA guidelines no longer recommend absolute age as a cutoff for recommending treatment options. They recommend using life expectancy and overall health as factors to consider.
Stages in the open retropubic procedure
•The patient is under anesthetic, catheterized, and positioned supine with the middle of the table separated to open up entry to the pelvis.
•Through a lower midline incision, staying extraperitoneal, the retropubic space is opened.
•Obturator fossa lymphadenectomy is recommended for a PSA >10 or Gleason score t7. Others consider this to be essential, as many patients will be clinically understaged on the basis of Gleason grading.
•Incisions in the endopelvic fascia on either side allow access to the prostatic apex and membranous urethra.
•Division and hemostatic control of the dorsal vein complex passing under the pubic arch allow access to the membranous urethra, which is divided at the prostatic apex.
•The prostate is mobilized retrogradely from apex to base, taking Denonvilliers fascia on its posterior surface.
•If cavernous nerve sparing is undertaken, the apical and posterior dissection is modified to allow preservation of the neurovascular bundles as they course posterior–laterally between the rectum and prostate.
MANAGEMENT OF LOCALIZED PROSTATE CANCER 219
•Denonvilliers fascia is incised at the prostatic base, allowing access to the vasa (divided) and seminal vesicles (excised).
•The bladder neck is divided, freeing the prostate.
•The bladder neck is reconstructed to the approximate diameter of the membranous urethra.
•A sutured vesicourethral anastomosis is stented by a urethral catheter, typically for 2 weeks.
•The wound is closed, leaving pelvic drains, typically for 48 hours.
The nerve-sparing modification aims to reduce the risk of postoperative erectile dysfunction. The surgeon seeks to minimize injury to the cavernosal nerves passing from the autonomic pelvic plexus on either side in the groove between prostate and rectum, during mobilization of the prostate. This should not be attempted in the presence of palpable disease as it may compromise cancer control. The tips of the seminal vesicles may also be spared in cases with low risk of cancer involvement, potentially reducing bleeding and cavernosal nerve injury.
Stages in the robotically assisted laparoscopic prostatectomy
•The patient is given a general anesthetic and positioned in a low lithotomy position with either Allen stirrups or spreader bars, and an orogastric tube and sterile bladder catheter are placed.
•Through a 1-inch supraumbilical incision, pneumoperitoneum is established up to 15 mmHg with a Veress needle, and 4 to 5 additional working ports (4 total robotic and 1–2 for an assistant) are placed in the lower abdomen and pelvis.
•The patient is placed in a steep Trendelenburg position and the robot is rolled in and docked to the patient.
•The vasa deferentia are dissected posterior to the bladder bilaterally to the level of the seminal vesicles, and these structures are ligated individually, with the vasa divided and the seminal vesicles excised.
•Denonvilliers fascia is incised at the posterior border of the prostate to reveal perirectal fat.
•Anteriorly, bilateral obliterated umbilical ligaments are divided and an inverted U incision is made in the urachus and, using the vasa deferentia as the lateral and posterior border, the bladder is dropped posteriorly to enter the space of Retzius.
•The endopelvic fascia is incised bilaterally to reveal the entire lateral border of the prostate up to the level of the apex, where the puboprostatic ligaments are divided.
•The bladder neck is incised anteriorly to the level of the bladder catheter, which is retracted superiorly so that the bladder neck can be incised posteriorly and the bladder peeled off the prostate.
•The vasa deferentia and seminal vesicles are located and divided, if not done so at the beginning of the procedure, and retracted cephalad and superiorly so that the prostate can be dissected antegrade.
220CHAPTER 6 Urological neoplasia
•If cavernous nerve sparing is undertaken, the posterior and apical dissections are modified to allow preservation of the neurovascular bundles as they course posterior–laterally between the rectum and the prostate.
•The dorsal venous complex is ligated and divided, and the distal urethra is divided, freeing the prostate, which is placed in a laparoscopic entrapment bag and moved out of the field.
•Obturator fossa lymphadenectomy is recommended for a PSA >10 or Gleason score t7. Others consider this to be essential because many patients will be clinically understaged on the basis of Gleason grading.
•If needed, the bladder neck is reconstructed to approximate the diameter of the membranous urethra.
•A sutured vesicourethral anastomosis is completed over a fresh bladder catheter that is left in for 7–10 days.
•A pelvic drain is placed through one of the working ports under direct vision and left in for approximately 24 hours.
•The robot is rolled away and the specimen is delivered out of the supraumbilical port site, which is increased in size to accommodate the prostate.
•The port sites are all closed.
This page intentionally left blank