

Liver and Gallbladder Major Maneuvers and Findings:
conventional teaching revisited
•Palpate the enlarged bottom of the gallbladder (Courvoisier's law): valuable sign of olden days (but may not apply to obese patients)
•Elicit and recognize Murphy's sign: specific for cholecystitis, but not highly sensitive
•Palpate lower edge of the liver at rest and deep inspiration: only helpful to assess the surface characteristics of the liver edge; not useful to assess hepatomegaly
•Palpation of the liver edge for consistence and surface characteristics: huge interobserver reliability
•Locate the dome of the liver by percussion: the only game in town for locating the upper liver edge
•Measure the width of hepatic dullness by percussion: probably unreliable in different hands (huge interobserver variability)
•Pulsatile liver and hepatojugular reflux: helpful maneuvers
•Scratch test: needs more validation, but overall an accurate maneuver to locate the lower liver edge
•Auscultation

Fig. 19
Palpation of the liver/spleen. A. Liver. B. Spleen.
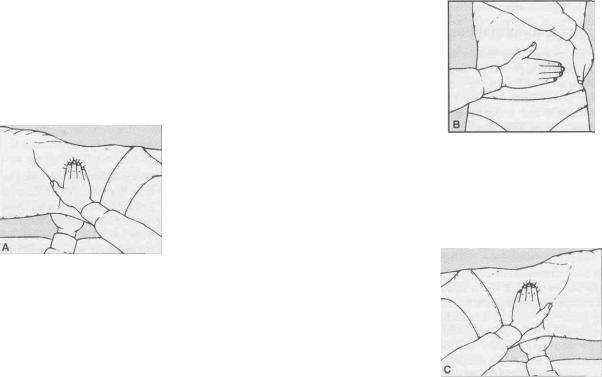
Fig. 20
Palpation of the kidneys.
A. Right kidney from right side. B. Left kidney from right side. C. Left kidney from left side.