

Topographic divisions of the abdomen.
Auscultatory signs of the liver disorders
•friction rubs
•arterial bruits
•A bruit associated with a rub is almost always a sign of neoplasia
•venous hums
•
Palpation of the liver allows assessment of characteristics of the lower liver edge, such as
•(1) consistency and contour
•(2) abnormalities of its surface (e.g., presence of nodules)
•(3) tenderness
•(4) presence of systolic pulsations
•(5) presence of frictions and thrills
Spleen Major Maneuvers and Findings:
conventional teaching revisited
•Palpation for splenomegaly: more specific than percussion, but less sensitive
•Percussion for splenomegaly: more sensitive than palpation, but less specific
•Auscultation for bruits and rubs: not too common; usually indicative of infarcts but also present in simple splenomegaly
Methods to palpate the spleen
•(1) bimanual palpation, (2) ballottement,
(3) palpation from above, and (4) one- hand hook technique.
The ways to percuss the spleen
•(1) Nixon's technique
•(2) Castell's technique
•(3) percussion of Traube's sernilunar space.

Abdominal venous patterns. A, Expected. B, Portal hypertension. C, Inferior vena cava obstruction. (From Seidel HM, Ball JW. Dains JE, Benedict GW: Mosby's Guide to Physical Examination, 3rd ed.
Si. Louis, Mosby, 1995, with permission.)
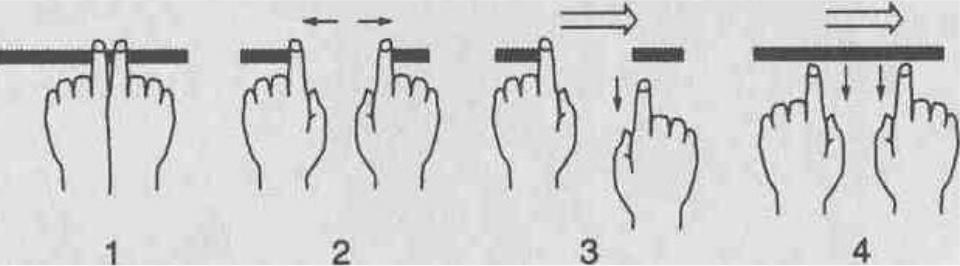
18. How can one demonstrate direction of flow in an engorged collateral vein?The examiner first should place his or her two index fingers over the engorged vein and collapse it, then slide the fingers apart, producing a 1-inch stretch of empty vein. By releasing first the pressure on the caudal end and then on the rostral end of the vein, the exami ner can see the direction of refilling (upward or downward, respectively).
Testing direction of blood flow in superficial veins. The examiner presses the blood from the veins with his 'ndex fingers in apposition (I). The index fingers are slid apart, milking the blood from the intervening seg-ttient of vein (2). Tlie pressure upon one end of the segment is then released (3) to observe The time of refilling from that direction. The procedure is repeated and the other end released first (4). The flow of blood is in Hie direction of the faster flow. (Adapted from De Gowin RL: De Gowin and De Gowin's Diagnostic Examination, 6th ed. New York, McGraw-Hill, 1994.)

A, Palpating the liver. Fingers are extended, wifh tips on right midclavicular line below the level of liver tenderness and pointing toward the head. B, Alternate method for liver palpation with fingers parallel to the costal margin. C, Palpating the liver with fingers hooked over the costal margin. (From

Technique for liver percussion. (Adapted from Swartz MH: Textbook of Physical Diagnosis, 3rd ed. Philadelphia, W.B. Saunders, 1997.)