

CARDIS
4.THYROID DISEASE
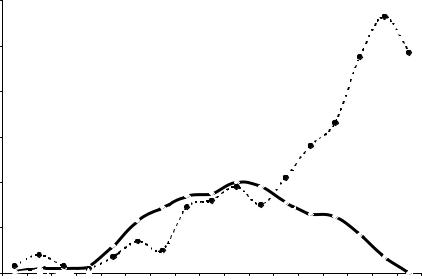
The main health effect of radiation from the accident observed to date is a dramatic increase in the incidence of thyroid cancer in young people, which started to be documented in 1991 in Belarus and continues until now in the most contaminated areas of Belarus, the Russian Federation and Ukraine [9, 15, 16]. Fig. 1 illustrates the temporal trends of childhood, adolescent and adult thyroid cancer in Belarus since the accident. The highest incidence of childhood thyroid cancer was about 40 per million children per year (compared to pre-accident rates which were of the order of 0.3–0.5 cases per million per year) in 1995. The childhood thyroid cancer rates have declined to zero as the population has aged (by 2002, none of those who were children at the time of the accident were children anymore) and parallel increases have been seen in the incidence of thyroid cancer in adolescents and then in young adults.
During the period 1986–2002 in Belarus, the Russian Federation and Ukraine, nearly 5000 cases of thyroid cancer were diagnosed among those who were children and adolescents (0–18 years) at the time of the accident (Table 3). Close to 4000 of these cases were children below the age of 15 at the time of exposure.
|
12 |
|
|
Incidence per 100 000 in Belarus |
|
|
|
11.3 |
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Adolescents |
|
|
10 |
|
|
|
|
|
|
|
|
|
9.5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9.7 |
000 |
8 |
|
|
|
|
|
|
|
|
|
|
|
100 |
|
|
|
|
|
|
|
|
|
|
Young adults |
|
|
|
|
|
|
|
|
|
|
|
|
|
6.9 |
per |
|
|
|
|
|
|
|
|
|
|
6.6 |
|
6 |
|
|
|
|
|
|
|
|
5.6 |
5.75.7 |
||
|
|
|
|
|
|
|
|
|
||||
Cases |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
4 |
|
|
4.9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.2 |
|
|
|
4 |
|
|
|
|
|
|
|
3.8 |
|
|
|
|
|
|
|
|
3.4 |
3.5 |
|
|
3.4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
2.9 |
|
3.8 |
3 |
3.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
2.3 |
2.9 |
3.2 |
|
2.6 |
|
2.5 |
|
|
|
|
|
|
|
|
2.1 |
|
|
|
||
|
|
|
|
|
|
1.9 |
|
|
|
Children |
||
|
|
|
|
|
|
|
|
|
|
1.7 |
||
|
|
|
|
|
|
|
|
|
2.6 |
|
||
|
2 |
|
|
|
|
|
|
|
|
|
||
|
|
|
1.2 |
1.4 |
|
|
1.4 |
|
|
|
||
|
|
|
|
1,0 |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
0.8 |
|
|
|
|
|
|
|
|
|
0.7 |
|
0.3 |
0.1 |
0.3 |
0.2 |
0.4 |
0.8 |
|
|
|
|
|
0 |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
0 |
|
|
|
|
|
|
|
|
|
|
|
1986 |
1987 |
1988 |
1989 |
1990 |
1991 |
1992 |
1993 |
1994 |
1995 |
1996 |
1997 |
1998 |
1999 |
2000 |
2001 |
2002 |
FIG. 1. Annual incidence of childhood, adolescent and adult thyroid cancer in Belarus among those who were children (below 15 years of age) at the time of the Chernobyl accident (courtesy of Yu. E. Demidchik).
84
SESSION 1
TABLE 3. NUMBER OF CASES OF THYROID CANCER BY COUNTRY AND AGE AT EXPOSURE (1986–2002). REPORTED NUMBER OF DEATHS ARE SHOWN IN ITALICS (PERSONAL COMMUNICATIONS, CANCER REGISTRIES OF BELARUS AND UKRAINE 2006, AND CANCER SUBREGISTRY OF THE RUSSIAN NATIONAL MEDICAL AND DOSIMETRIC REGISTRY 2006)
Age at exposure |
|
Belarus |
Russian |
Ukraine |
Overall |
|
Federationa |
||||
|
|
|
|
|
|
|
|
|
|
|
|
0–14 |
Cases |
1711 |
349 |
1762 |
3822 |
|
deaths |
8 |
1 |
6 |
15 |
15–18 |
Cases |
299 |
134 |
582 |
1015 |
|
|
|
|
|
|
Total |
|
2010 |
483 |
2344 |
4837 |
a Bryansk, Tula, Kaluga and Orel regions (1986–2000).
Given the rarity of thyroid cancer in young people, the large population with high doses to the thyroid and the magnitude of the radiation related risks estimates derived from epidemiological studies, it is most likely that a large fraction of thyroid cancers observed to date among those exposed in childhood is attributable to radiation exposure from the accident.
Although the impact on thyroid cancer risk of the accident is large, the prognosis of the disease is fortunately very good. Only 15 individuals of the cases of childhood cancer have been reported to have died (eight in Belarus, six in Ukraine and one in the Russian Federation).
4.1. Thyroid cancer epidemiological studies
The Chernobyl experience has provided a unique opportunity to learn about the effects of exposure to doses from radioactive iodines on thyroid cancer risk. Careful epidemiological and dosimetry studies should provide important evidence for radiation protection measures.
A large number of epidemiological studies of thyroid cancer have been carried out in Belarus, the Russian Federation and Ukraine since the accident. The majority of studies are ecological or descriptive epidemiological studies, in which estimates of dose are available at the population rather than individual level. Only three analytical case control studies with individual dose estimates have been published at the time of this review.
It is important to consider the strengths and limitations of each study in interpreting results regarding the risk of thyroid cancer after Chernobyl.
85
CARDIS
Numerous ecological studies have been published [9, 16–21]. Most of these studies have clearly shown an association between thyroid cancer incidence in young people and average dose to the thyroid. Risk estimates have been derived in these studies — the most comprehensive, based on combined analyses of data from the three countries were presented by Jacob et al. [18]: EAR 2.1 per 10 000 Py–Gy (95% CI 1.0–4.5); ERR 23 per Gy (95% CI 8.6–82). The ERR is much larger than that reported in studies of populations exposed to external radiation in childhood (ERR 7.7 per Gy [22]). Results of ecological studies in areas with good dosimetry are more closely related to the radiation risk in the population. However, their results may be influenced by ecologic bias, related to the absence of data on potential confounding factors, in particular on the intensity of screening.
Results of analytical studies (e.g. case control and cohort studies) with good individual dose reconstruction provide more informative quantitative estimates of risk of thyroid cancer after the Chernobyl accident than ecological studies. Three studies have been published to date [23–25]. The most recent study was conducted in Belarus and the Russian Federation, covers 276 cases and 1300 controls, and provides direct estimates of the effects of I131 [25]. The ERR per Gy in that study ranges from 4.5 to 7.4, depending on the model used, slightly lower than, but consistent with, the estimates from studies of external exposures in children. Results of the first two case control studies [23, 24], although based on fewer cases and, for the Astakhova study, less detailed dosimetry are consistent with this.
No direct information is available at present to evaluate the pattern of thyroid cancer risk over time. Based on studies of other populations exposed to external radiation that have been followed-up for several decades [22], it is expected that thyroid cancer risk from Chernobyl will continue for many more years, although the long term magnitude of risk is difficult to quantify.
Large scale screening programmes were initiated in contaminated areas shortly after the accident [2]. Screening programmes, in general, increase the apparent incidence of thyroid cancer by advancing the time of diagnosis of tumours that would otherwise become clinically apparent only at some later date, and possibly by identifying tumours that would never become clinically manifest. Screening therefore has important implications in the areas of public health and thyroid cancer risk estimation, yet we lack quantitative data regarding their effects in either of these areas.
New studies indicate that iodine deficiency at the time of exposure may increase the risk of radiation-induced thyroid cancer [20, 25] and stable iodine supplementation in the years after exposure may reduce this risk [25]. Further studies are needed to replicate these findings.
86
SESSION 1
While the increased risk of thyroid cancer in those exposed in childhood and adolescence is clear, there is much less information on the effects of exposure as an adult.
4.2. Biology of thyroid cancer
Papillary cancer is the primary pathological type of thyroid cancer in those exposed as children and adolescents to fallout from the Chernobyl accident. There are a variety of subtypes of papillary cancer, and it appears that these may be related to latency and, therefore, change with time since exposure. It is not clear whether this change in morphology is related to clinical presentation or outcome.
At the molecular level, it would appear that the earlier suggestion that specific rearrangements of the ret oncogene may be a marker for radiation exposure has not been substantiated. Analysis of mutations in individual genes has not identified differences between radiation-associated thyroid cancers, and age matched non-irradiation related cancers of similar morphology. However, it is clear that there are major differences in the molecular biology and pathology of papillary cancers as a function of age at clinical presentation. From initial studies on multiple gene expression analysis, it is not clear that a radiation signature can be identified at this time.
The molecular biology and the pathomorphology of post-Chernobyl thyroid cancer is dynamic, and a considerable effort needs to be maintained in monitoring both of these features with time post-Chernobyl. Attention must also be paid to the interpretation of the molecular biology studies, in particular the sensitivities of the different techniques used.
4.3. Treatment of childhood thyroid cancer
Thyroid cancer in children is a rare disease, so the experience worldwide related to diagnosis, treatment and follow-up of this tumour disease is limited. Up to now, our knowledge about the natural course of radiation-induced thyroid carcinoma is sparse. At the time of diagnosis, many children present with extraglandular tumour spread, lymph node and distant metastases. Even in children with advanced tumour stages, treatment with thyroidectomy, followed by high dose radioiodine therapy and consecutive levothyroxine TSH-suppressive hormone replacement is effective. In general, the prognosis for young patients with papillary thyroid carcinoma can be considered as excellent. Concerning the side effects of treatment, our knowledge about the consequences of hypoparathyroidism frequently accompanying thyroidectomy
87