
ACLS ALGORITHMS |
305 |
|
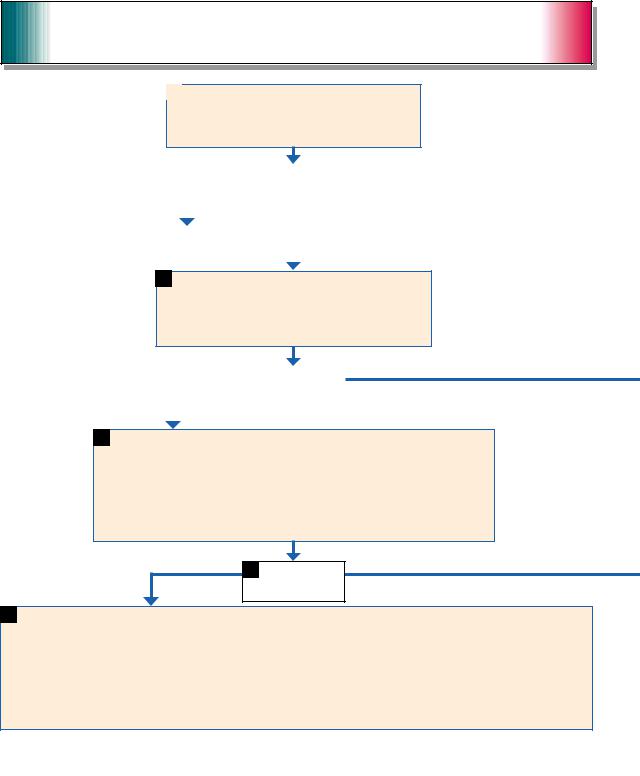
Not shockable
9 |
Asystole or pulseless electrical activity (PEA) |
|
|
|
|
|
|
|
10 |
Resume CPR immediately for five cycles. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
When I.V./I.O. available, give vasopressor |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
• epinephrine 1 mg I.V./I.O. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Repeat every 3 to 5 minutes. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
or |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
• May give 1 dose of vasopressin 40 units I.V./I.O. to replace |
|
|
|
|||||||||
|
|
|
|
|
|
|
first or second dose of epinephrine. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Consider atropine 1 mg I.V./I.O. for asystole of slow PEA rate; |
|
|
During CPR |
|||||||||
|
|
|
|
|
|
|
repeat every 3 to 5 minutes (up to three doses). |
|
|
|
|
|
|||||||
|
Not shockable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Push hard and fast (100/ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Give five cycles of CPR.* |
|
minute). |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Ensure full chest recoil. |
|
|
|
|
|
|
|
|
|
11 |
|
Check rhythm. |
|
|
|
|
|
|
• Minimize interruptions in |
|
|
|
|
|
|
|
|
Not shockable |
Shockable rhythm? |
|
Shockable |
|
|
chest compressions. |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• One cycle of CPR: 30 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
compressions then 2 breaths; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
five cycles = 2 minutes. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Avoid hyperventilation. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Secure airway and confirm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
placement. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Rotate compressors |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
every two minutes with rhythm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
• If asystole, go to Box 10. |
|
|
|
|
|
|
13 |
Go to Box 4. |
|
checks. |
||||
Not shockable |
|
• If electrical activity, check |
|
|
|
|
|
|
|
|
|
|
• Search for and treat possible |
||||||
|
|
|
|
|
|
|
|
|
|
|
contributing factors, such as: |
||||||||
|
pulse. If no pulse, go to Box 10. |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
– hypovolemia |
|||||||
|
|
|
• If pulse present, begin |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
– hypoxia |
||||||
|
|
|
postresuscitation care. |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
– hydrogen ion (acidosis) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– hypokalemia/hyperkalemia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– hypoglycemia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– hypothermia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– toxins |
* After an advanced airway is placed, rescuers no longer deliver “cycles” of CPR. Give continuous chest |
|
– tamponade, cardiac |
|||||||||||||||||
compressions without pauses for breaths. Give 8 to 10 breaths/minute. Check rhythm every 2 minutes. |
|
– tension pneumothorax |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– thrombosis (coronary or |
Reproduced with permission, “2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation |
|
pulmonary) |
|||||||||||||||||
and Emergency Cardiovascular Care: Part 7.2-Management of Cardiac Arrest,” Circulation 2005: 112(suppl IV): |
|
– trauma. |
|||||||||||||||||
IV–58–IV–66. © 2005, American Heart Association. |
|
|
|
|
|
|
|
|
|
|
|
||||||||