

Полезные материалы за все 6 курсов / Ответы к занятиям, экзаменам / 4. Пищеварительная
.pdfGasterointerstinal Physiology
Bilingual Version (ENG/DE)
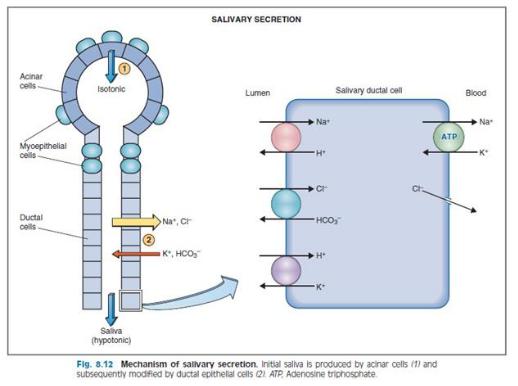
A final question is How does saliva, which was initially isotonic, become hypotonic as it flows through the ducts? The answer lies in the relative water impermeability of the ductal cells. As noted, there is net absorption of solute because more NaCl is absorbed than KHCO3 is secreted. Because ductal cells are water impermeable, water is not absorbed along with the solute, making the final saliva hypotonic.
Salivary secretion
Lysozymes → disrupt bacterial cell walls
• Lactoferrin → prevent bacterial growth
IgA antibody
Initial fluid similar to plasma (isotonic) • Same Na, Cl, K, HCO3concentration
•Ductal cells (impermeable to water): • Remove
Na, Cl
•Secrete K, HCO3- (bicarb raises pH → protects against acid)
Aldosterone
•Effects salivary glands similar to kidneys
•↑ Na absorption
•↑ K secretion
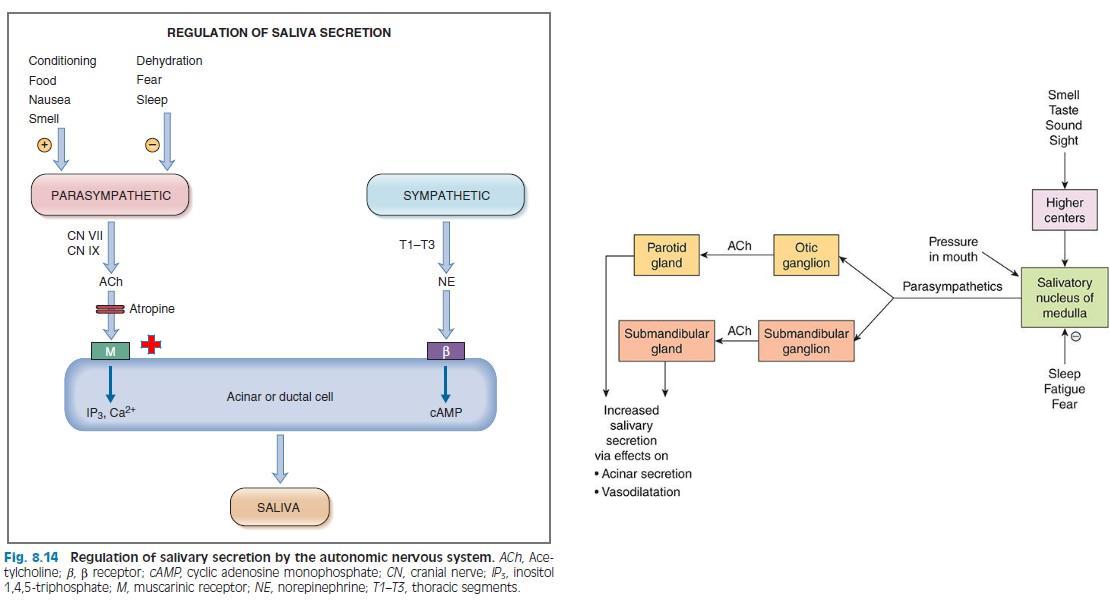
пилокарпин

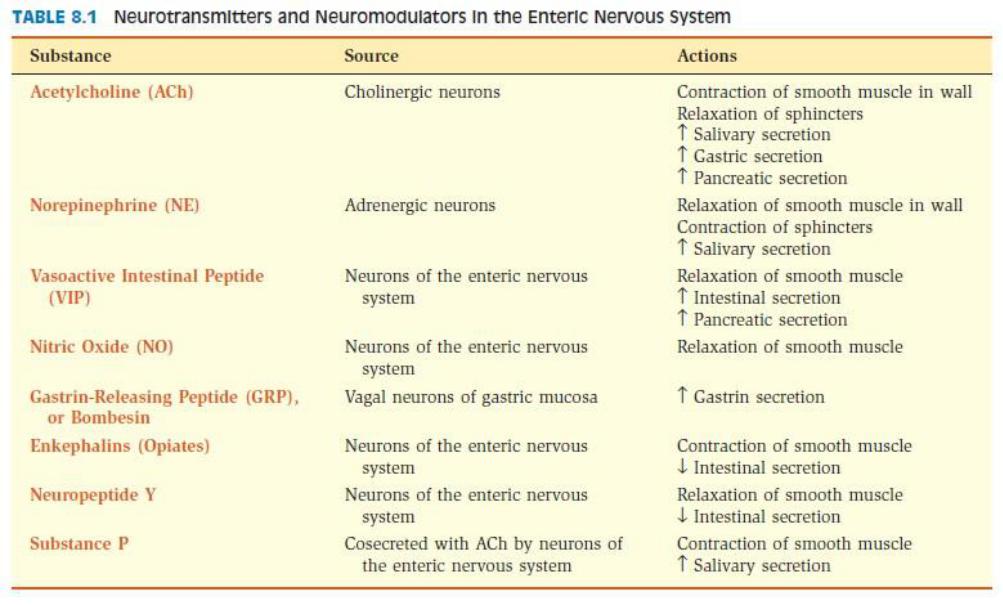
How regulated secreation of gastrin ?
M3
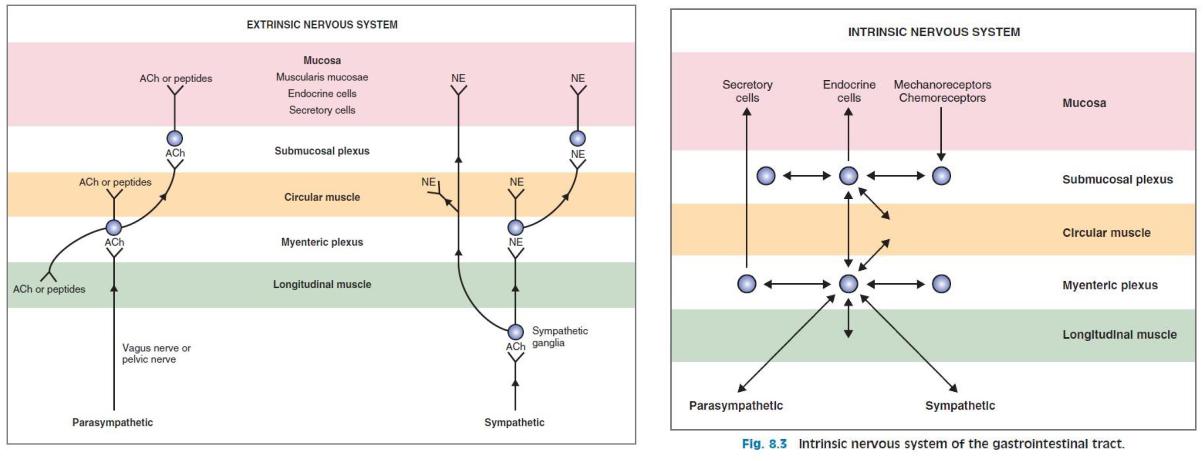
ACh is released from vagus nerves innervating the gastric mucosa and binds directly to muscarinic (M3) receptors on the parietal cells.
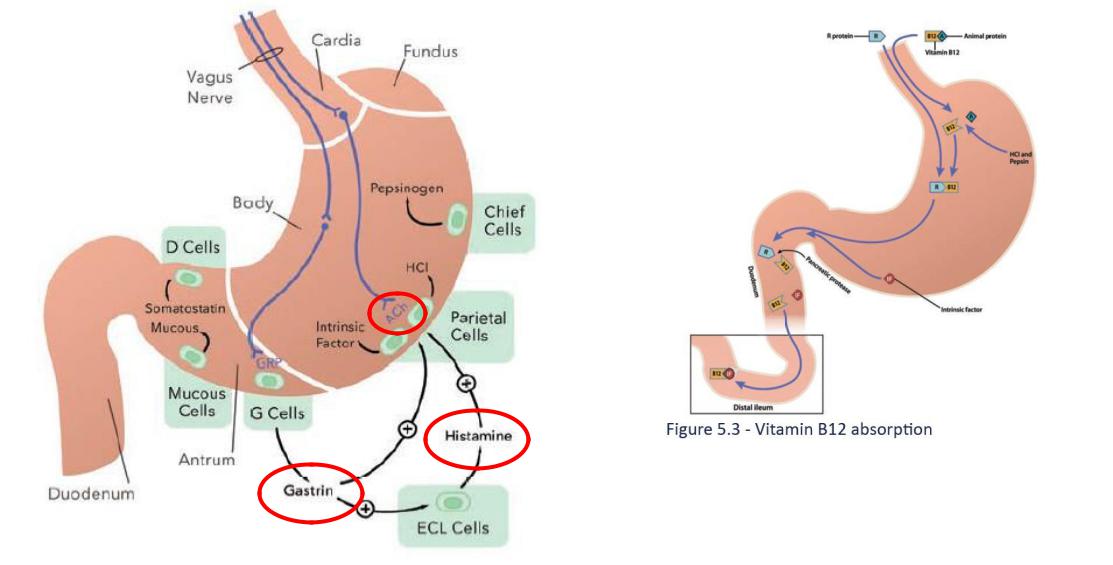
Intrinsic Factor
•Necessary for vitamin B12 absorption
•Released by parietal cells (along with H+)
The second messengers for ACh are IP3/Ca2+. When ACh binds to muscarinic receptors, phospholipase C is activated. Phospholipase C liberates diacylglycerol and IP3 from membrane phospholipids, and IP3 then releases Ca2+
from intracellular stores. Ca2+ and diacylglycerol activate protein kinases that produce the final physiologic action: H+ secretion by the parietal cells.
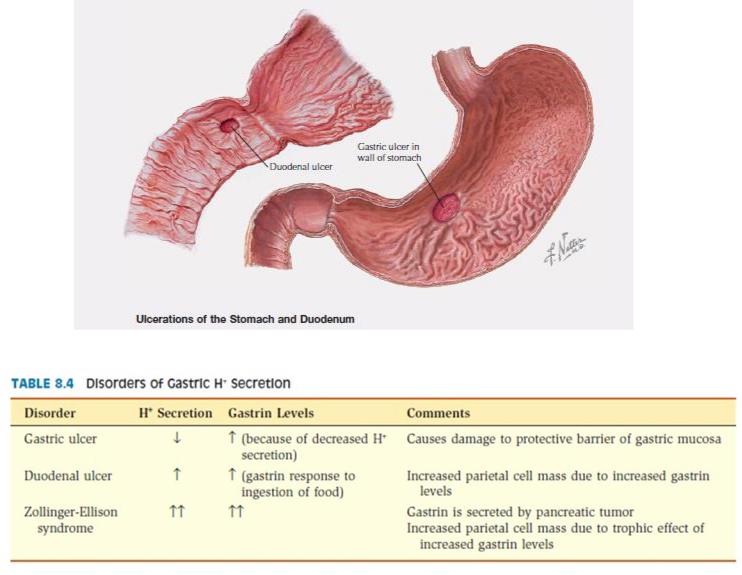
Thus for a peptic ulcer to be created, there must be (1) loss of the protective mucous barrier, (2) excessive H+ and pepsin secretion, or (3) a combination of the two.
Damaging factors, in addition to H+ and pepsin, are Helicobacter pylori infection, nonsteroidal antiinflammatory drugs (NSAIDs), stress, smoking, and alcohol consumption.
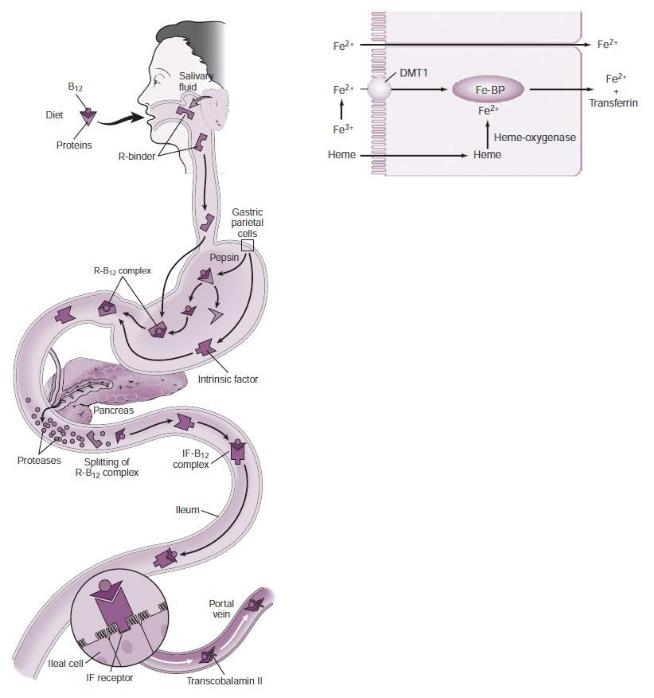
Gramnegative anaerobic bacterial overgrowth in the small intestine are associated with B12 deficiency.
bacteria bind to the vitamin B12–intrinsic factor complex, preventing its absorption
inhibitors of H/K-ATPase - suppress acid production in the parietal cells and do not affect intrinsic factor secretion
Free iron then binds to apoferritin and is transported across the basolateral membrane into the blood.
In the circulation, iron is bound to a β-globulin called transferrin, which transports it from the small intestine to storage sites in the liver - to the bone marrow
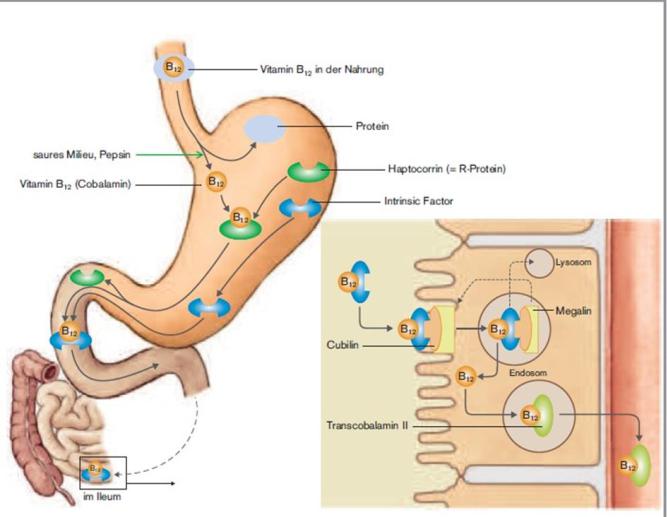
•Vitamin B12 ein Kofaktor der Methylmalonyl- CoA-Mutase. Ein Mangel erhöht die
Konzentration von Methylmalonylvorstufen und führt dadurch zu vermehrter Bildung unphysiologischer Fettsäuren. Diese sollen durch Einlagerung in Zellmembranen zur Ausbildung der neurologischen Symptome bei Vitamin-B12-Mangel führen (z. B.
Hinterstrangataxie mit Gangunsicherheit).
•Bei Vitamin-B12-Mangel akkumulieren die Zellen THF in Form von N5-Methyl-THF (dieses kann nur in Anwesenheit von Vitamin B12 weiterverstoffwechselt werden) wodurch die N5,N10-Methyl-THF-Spiegel fallen, so dass die DNA-Synthese abnimmt. Dies erklärt, warum ein Vitamin-B12-Mangel (z. B. bei Morbus Crohn oder atrophischer Gastritis) ebenfalls zu einer megaloblastären Anämie führt.