

Полезные материалы за все 6 курсов / Ответы к занятиям, экзаменам / 4. Пищеварительная
.pdfGastrinoma
Diagnosis
•Fasting serum gastrin level
•>10 times upper limit of normal in gastrinomas
•Secretin test
•Differentiate gastrinomas from other causes ↑ gastrin
•Normal G cells inhibited by secretin (leads to ↓ gastric pH)
•Gastrinomas stimulated by secretin
•Gastrin level will rise after secretin administration
Treatment
•High dose proton pump inhibitors • Omeprazole, lansoprazole, pantoprazole
•Octreotide (somatostatin) • Inhibits gastrin release for some patients
•Surgical excision

Vagotomy & Atropine
•Vagotomy • Old therapy for gastric ulcers
•Surgical disruption of vagus nerve to stomach
•Result: decreased acid production
•Atropine • Muscarinic blocker
•Blunts parietal cell stimulation by ACh
•Does not block stimulation by vagus → gastrin → HCL

Pernicious Anemia
•Autoimmune gastritis
•Loss of parietal cells → loss of intrinsic factor
•Cannot absorb vitamin B12
•High gastrin levels typical finding
•Also G-cell hyperplasia
Die atrophische Gastritis (Typ A) ist eine Autoimmunerkrankung, bei der
Autoantikörper gegen Belegzellen und Intrinsic Factor gebildet werden. Der dadurch
bedingte Vitamin-B12-Mangel führt zur Entstehung einer perniziösen Anämie, bei
der die Betroffenen neben den allgemeinen Anämiesymptomen (S.180) an gastrointestinalen Symptomen (z. B. „Hunter-Glossitis“ = glatte rote Zunge und Zungenbrennen
aufgrund einer Atrophie der Zungenpapillen) und an verschiedenen neurologischen Symptomen, wie z. B.
Störungen des Vibrationsempfindens,
Gangunsicherheit (spinale Ataxie), schmerzhafte
Missempfindungen (Parästhesien) an Händen und Füßen und Lähmungserscheinungen, leiden können.
Die Therapie besteht in der lebenslangen, meist parenteralen Substitution von Vitamin B12.

Stimuli for Acid Secretion
•#1: Gastrin (direct)
•Hormone from G cells of antrum (distal) stomach
•Binds CCKb receptor on parietal cells
•#2: Gastrin (indirect)
•Activates ECL cells
•Histamine released → stimulation
•#3: Vagus nerve
•ACh muscarinic (M3) receptors
•Also activates G cells → Gastrin
•Not via ACh; uses gastrin releasing peptide (GRP)
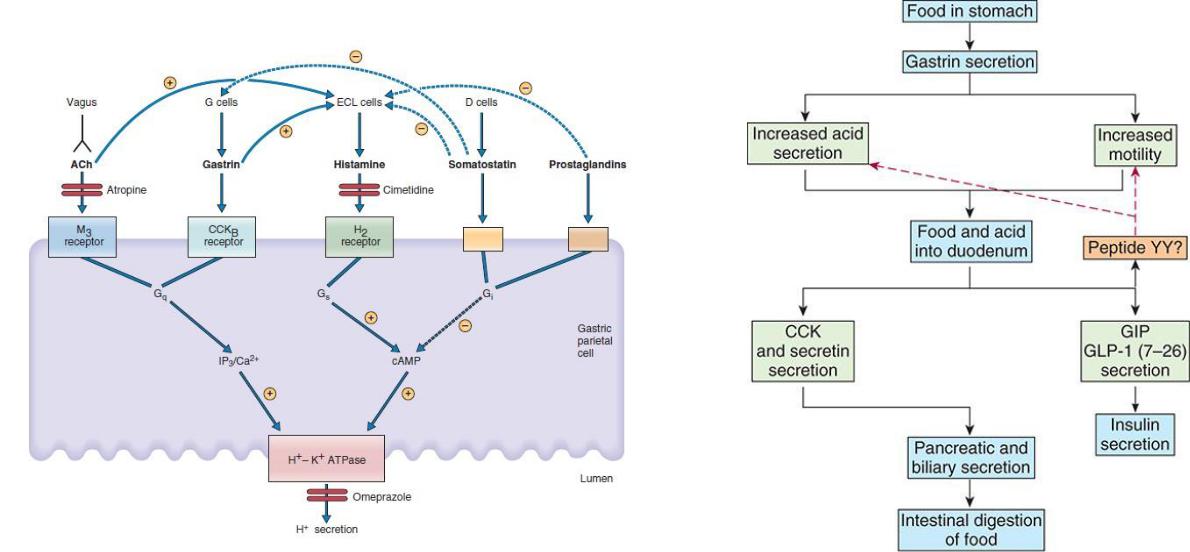

Vagus nerves innervate parietal cells directly, where they release ACh as the neurotransmitter. Vagus nerves also innervate G cells, where they release GRP as the neurotransmitter.
Vagal stimulation releases gastrin from the G cells, and gastrin enters the systemic circulation and is delivered back to the stomach to stimulate H+ secretion by the parietal cells. One consequence of this dual action of vagal stimulation is that muscarinicblocking agents such as atropine do not block HCl secretion completely. Atropine will block the direct
vagal effects on the parietal cells, which are mediated by ACh, but it will not block the vagal effects on gastrin secretion because the neurotransmitter at the synapses on G cells is GRP, not ACh.

Диагностический тест на H. pylori основан на его уреазной активности. В ходе теста пациент пьет раствор, содержащий 13C-мочевину, которая превращается в 13CO2 иNH3 в желудке; 13CO2 всасывается в кровь, выдыхается легкими и измеряется вдыхательном тесте. Удивительно, но у людей с язвой желудка чистая скорость секреции H+ ниже нормы, потому что часть секретируемого H+ просачивается в поврежденную слизистую оболочку. При язвенной болезни желудка секреция скорость гастрина увеличивается в результате снижения чистой секреции H+. (Напомним, что секреция гастрина ингибируется H+.)
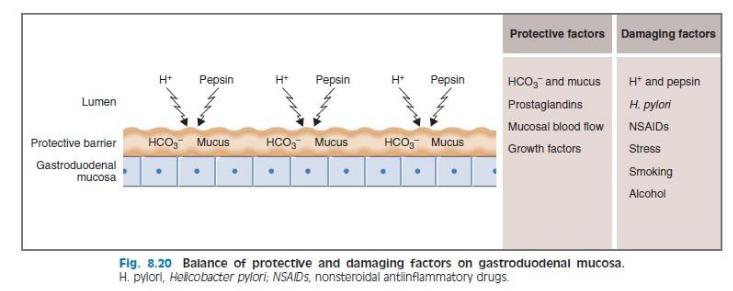
H. pylori colonizes the gastric mucus (often in the antrum), attaches to gastric epithelial cells, and releases cytotoxins (e.g., CagA toxin) that break down the protective mucous
barrier and the underlying cells. H. pylori is allowed to colonize the gastric mucus because it contains the enzyme urease, which converts urea to NH3.
The NH3 generated alkalinizes the local environment, permitting the bacteria to survive in the otherwise acidic gastric lumen. Because the local environment is hospitable, the bacteria bind to the gastric epithelium
instead of being shed.
A diagnostic test for H. pylori is based on its urease activity. In the test, the patient drinks a solution containing 13C-urea, which is converted to 13CO2 and NH3 in the stomach; the 13CO2 is absorbed into blood, expired by the lungs, and measured in a breath test. Surprisingly, in persons with gastric ulcers, net H+ secretory rates are lower than normal because some of the secreted H+ leaks into the damaged mucosa. In gastric ulcer disease, the secretion
rate of gastrin is increased as a result of the reduced net H+ secretion. (Recall that gastrin secretion is inhibited by H+.)

H. Pylori colonizes gastric mucus. One consequence of this
colonization is to inhibit somatostatin secretion from D cells in the gastric antrum.
Because somatostatin normally inhibits gastrin secretion from G cells, “inhibition of inhibition” results in increased gastrin secretion, which leads to increased H+ secretion by gastric parietal cells. In this way, there is an increased H+ load delivered to the duodenum.
Желудочная инфекция H. pylori распространяется на двенадцатиперстную кишку и ингибирует дуоденальный HCO3− секреция. В норме дуоденальный HCO3− достаточно для нейтрализации Н+ нагрузка, доставляемая из желудка. Однако в этом случае в двенадцатиперстную кишку поступает не только избыток H+, но и меньше HCO3− выделяется для его нейтрализации. Таким образом, нейтрализация H+ в двенадцатиперстной кишке недостаточна, содержимое двенадцатиперстной кишки становится аномально кислым, и наблюдается эрозивное действие H+ и пепсина на слизистую оболочку двенадцатиперстной кишки.
У лиц с язвой двенадцатиперстной кишки исходный уровень гастрина может быть нормальным, но секреция гастрина в ответ на прием пищи увеличивается. Повышенный уровень гастрина также оказывает трофическое действие на желудок, что увеличивает массу париетальных клеток.
