

Книги по МРТ КТ на английском языке / MRI for Orthopaedic Surgeons Khanna ed 2010
.pdf230 IV Spine
ficult. MRI provides soft-tissue visualization superior to that of conventional radiography or CT and is useful for the assessment of spinal cord injury, ligamentous injury, degree of spinal stenosis, and additional fracture evaluation. Occult fractures not visible on conventional radiographs or CT images may be detected by the presence of vertebral body edema on MR images. Although MRI is extremely sensitive in identifying cervical spine fractures, their characteristics and the exact appearance of the osseous components can be challenging; CT may be a better choice for assessing such details. In addition, MRI is useful for the evaluation of obtunded patients or those with cervical spine injury, neurologic deficits, or an unreliable physical examination.2–7
MRI is indicated specifically when neurologic deficit, vascular injury, or soft-tissue injury is suspected in the setting of trauma. It is also useful in assessing posttraumatic sequelae.8 Imaging spinal gunshot injuries is controversial. Theoretically, a ferrous gunshot fragment may become mobile, but most bullets are nonferrous, and therefore such patients can usually be imaged without consequences. Unfortunately, the exact composition of a gunshot fragment is seldom known, and therefore MRI remains controversial and dependent on the clinical need.9,10
It should be noted that there are obstacles to obtaining MRI studies in the trauma setting, especially with regard to cervical spine trauma, because patients may have clinically significant neurologic deficits. These obstacles include the following:
•Lack of availability of MRI capabilities on an urgent basis
•MR-incompatibility of some ventilators, traction devices, and other equipment
•Lack of clinical access to patients during the imaging study
MRI protocols vary by institution, but commonly used sequences in trauma evaluation include the following11:
•Sagittal T1-weighted images to assess the alignment of the cervical spine, vertebral body integrity, fractures, and spinal cord caliber
•Sagittal T2-weighted images to assess for the presence of cord edema, compression, and spondylotic changes
•Sagittal STIR images to assess for the presence of paraspinal ligamentous injury and bone marrow edema
•Axial T1-weighted and T2-weighted images to assess for the presence of posterior element fractures, to evaluate for spinal stenosis, to better define disc pathology, and to confirm the precise location of abnormalities detected on sagittal images
•Sagittal T2-weighted gradient-echo images (in some institutions) to assess for the presence of acute spinal cord hemorrhage and disc herniation (high signal in the disc even with severe osseous degeneration, which
Table 10.1 Evaluation of Cervical Spine Trauma
|
Anatomy |
Evaluation |
|
|
Spinal column/ |
Alignment |
|
|
vertebral bodies |
Vertebral body fracture |
|
|
|
Posterior element fracture |
|
|
|
Edema |
|
|
|
Degenerative change |
|
|
Ligaments |
Anterior longitudinal ligament |
|
|
|
Posterior longitudinal ligament |
|
|
|
Interspinous and supraspinous |
|
|
|
ligaments |
|
|
|
Ligamentum flavum |
|
|
|
Evaluation for edema/rupture |
|
|
Spinal cord |
Edema |
|
|
|
Hemorrhage |
|
|
|
Compression |
|
|
|
Syrinx |
|
|
Epidural space |
Hematoma |
|
|
|
Disc herniation |
|
|
|
Osseous fragment |
|
|
Vascular |
Vertebral artery |
|
|
|
|
|
Source: Takhtani D, Melhelm ER. MR imaging in cervical spine trauma. Magn Reson Imaging Clin N Am 2000;8:615–634. Modified with permission.
enables the distinction between bone fragments and a disc herniation)
Regardless of the specific institutional MRI protocol, a systematic approach (see Chapter 3) for the evaluation of cervical spine MRI should be used to avoid missing pathologic conditions (see Table 10.1 for important cervical spine structures to evaluate). In addition, it is essential that the interpretation of the MRI findings be performed in conjunction with that of the other available imaging modalities, including conventional radiographs (with flexion and extension views if clinically indicated) and CT (see Chapter 17).
Classification of Cervical Spine Trauma
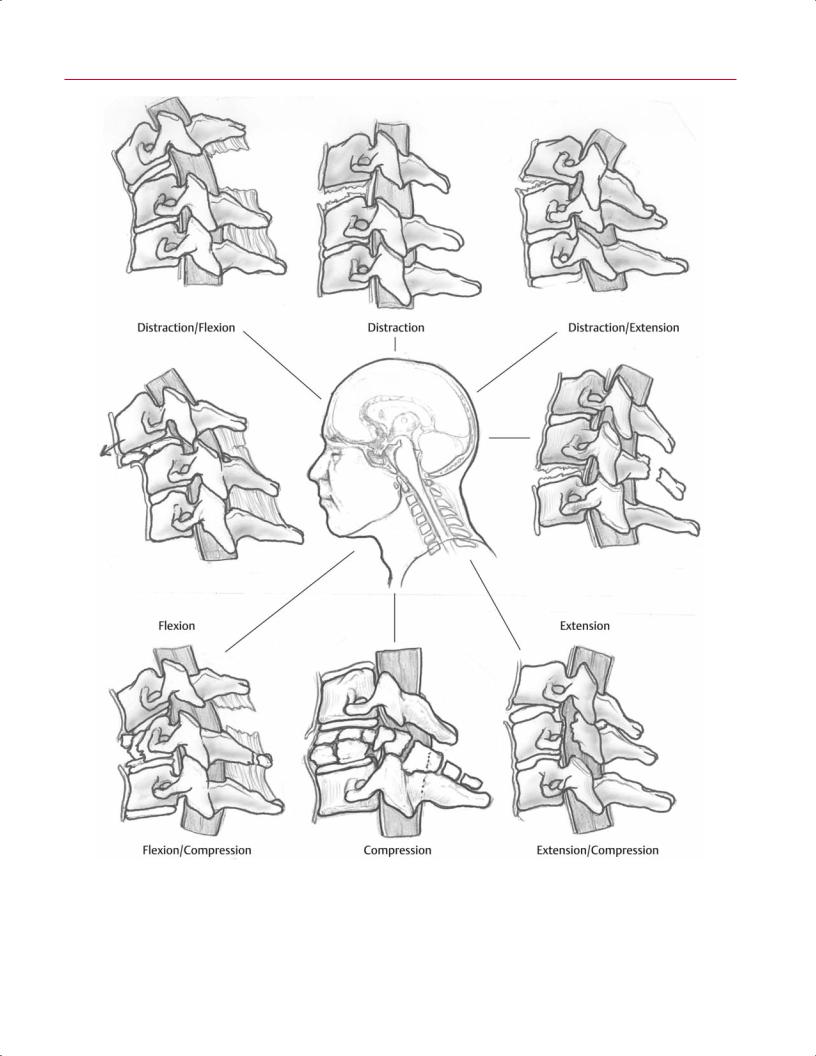
Cervical spine injuries can be classified based on the mechanism of injury. Although six categories have been described (vertical compression, compressive flexion, distractive flexion, lateral flexion, compressive extension, and distractive extension12) (Fig. 10.1), the classification scheme is simplified here into three broad categories:
•Hyperflexion
•Hyperextension
•Axial loading
In many instances, the mechanism of injury can be di cult to determine from an analysis of the clinical situation (in the absence of imaging findings), and therefore clinicians may choose to broadly classify cervical spine injuries as follows:
•Secondary to blunt trauma
•Secondary to penetrating trauma
10 The Cervical Spine 231


 B
B
 B
B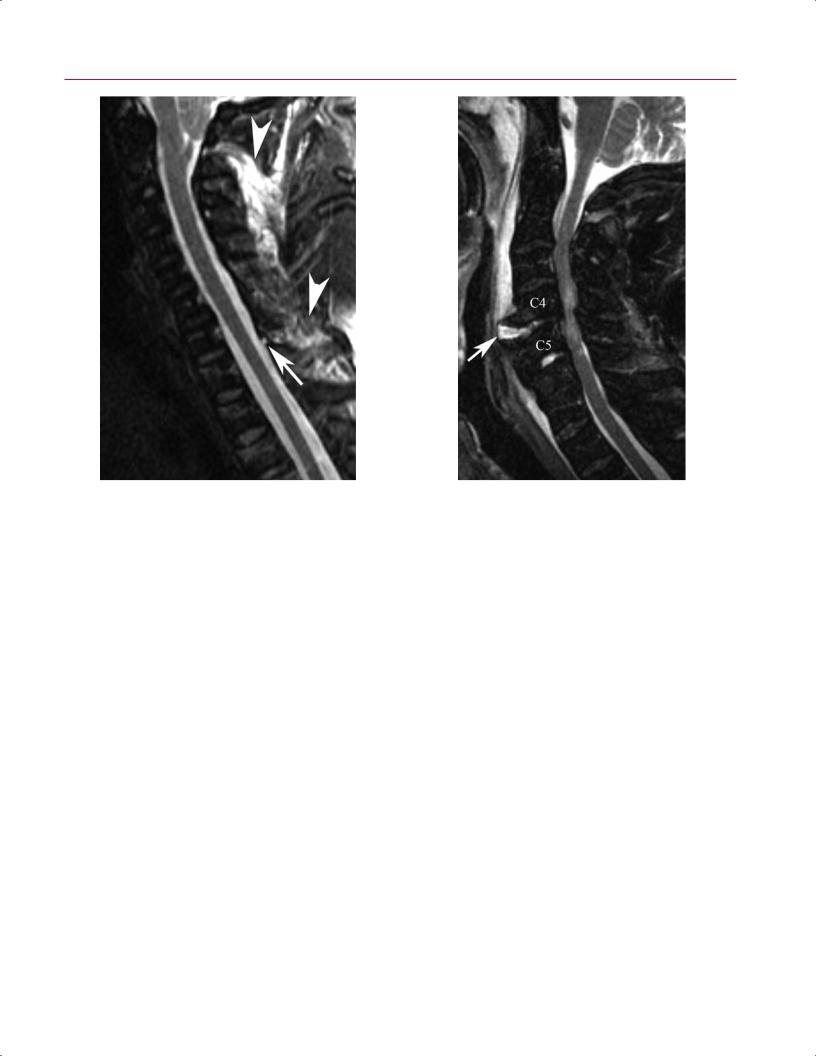

236 IV Spine
A |
B |
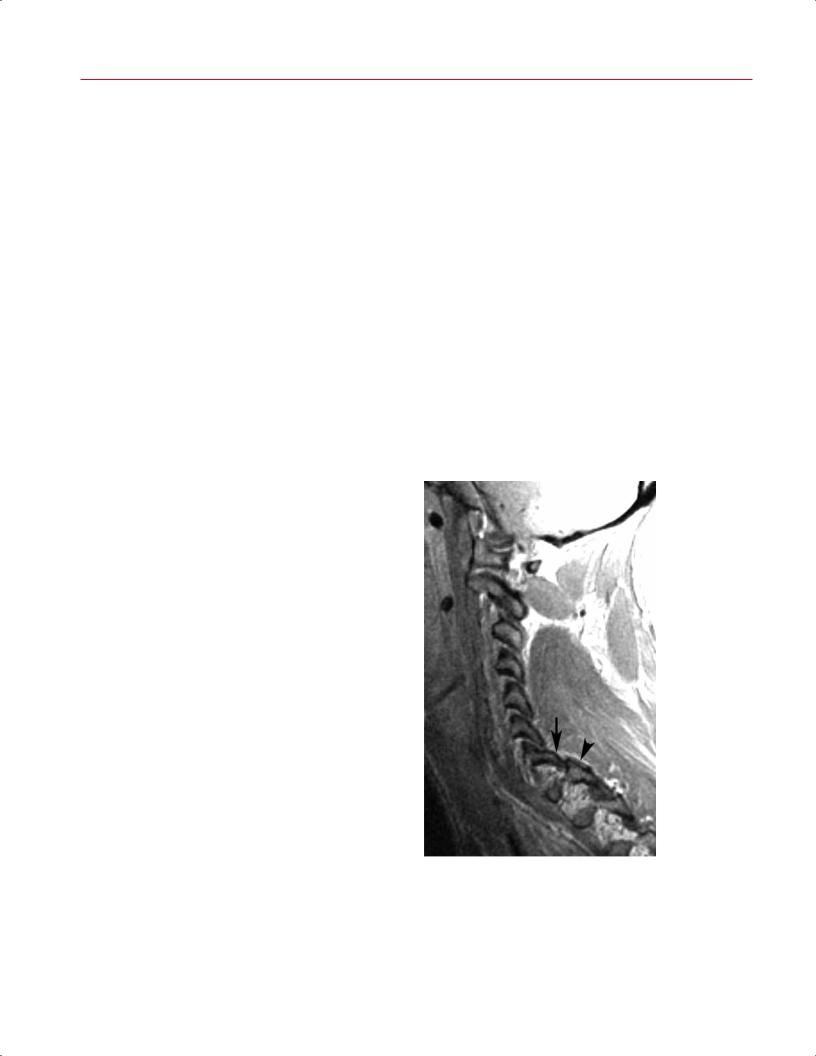
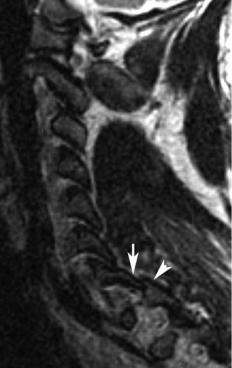
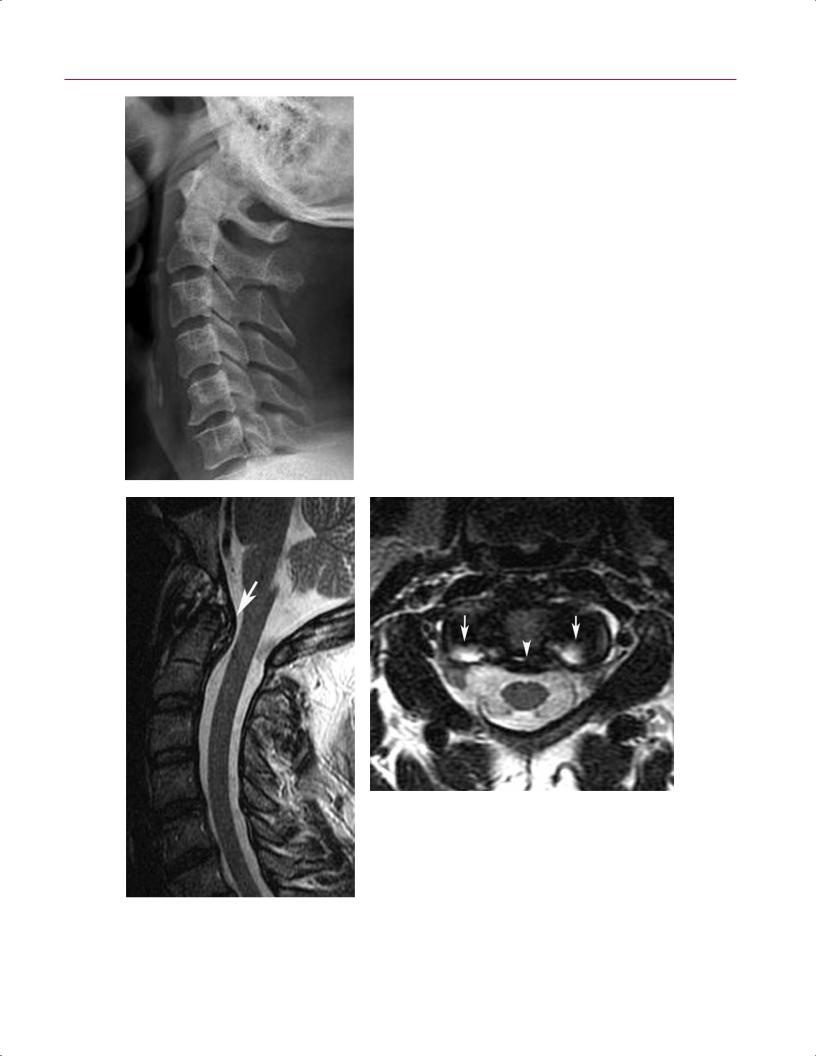
Fig. 10.7 Ankylosing spondylitis. (A) A T2-weighted image shows |
nondisplaced “fracture” or injury through the anterior column at C6 |
multilevel ankylosis of the cervical spine and ossification of the poste- |
(arrow) and posterior column injury; both injuries manifested as re- |
rior longitudinal ligament posterior to the body of C2 but no specific |
gions of increased signal intensity with the use of this fluid-sensitive |
evidence of fracture. (Conventional radiographs and CT images also |
pulse sequence. |
showed no evidence of fracture.) (B) A sagittal STIR image shows a |
|
Axial Load Injuries |
decompression and fusion that is often performed for pa- |
|
Axial load injuries are caused by the axial transmission of |
tients with cervical burst fractures. |
|
|
||
force through the skull, through the occipital condyles, and |
|
|
into the spine. This force transmission can cause a Je erson |
Occipitocervical Junction Injuries |
|
burst fracture or burst fractures of the subaxial cervical |
Although injury to the occipitocervical junction occurs in |
|
spine. MRI is useful for the assessment of C1 compression |
||
fractures and associated pathologies such as lateral mass |
a small percentage of blunt trauma victims (0.8% in one |
|
displacement on coronal images, atlantodental interval in- |
study26), recognition of such injuries is crucial because of |
|
crease on sagittal images, and transverse ligament disrup- |
their devastating e ects.27–30 A detailed discussion of occipi- |
|
tion on axial images.11 For burst fractures, MRI is useful |
tocervical craniotomy and the various measurement tech- |
|
for diagnosing associated spinal cord injury caused by an |
niques for evaluation of occipitocervical pathology is beyond |
|
acute herniated disc or retropulsion of osseous fragments |
the scope of this chapter, but presented here is an overview |
|
(Fig. 10.8). Because a purely axial force subjects the poste- |
of the major types of occipitocervical traumatic findings as |
|
rior capsuloligamentous structures to compression only, |
seen on MRI. It is important to keep in mind that MRI studies |
|
these posterior structures should remain intact.11,20 How- |
of the occipitocervical junction should be reviewed in con- |
|
ever, there often is some degree of spine flexion during the |
junction with conventional radiographic and CT imaging. |
|
traumatic event that may cause injury to the posterior spinal |
|
|
elements, which can be detected by MRI.20 It is important |
Atlantooccipital Dissociation |
|
to carefully scrutinize the fat-suppressed T2-weighted and |
||
|
||
other images for evidence of injury to the posterior ligamen- |
Atlantooccipital dissociation is any separation of the atlan- |
|
tous and osseous structures because such injury will lead to |
tooccipital articulation. The skull may displace anteriorly, |
|
consideration of posterior fusion in addition to the anterior |
posteriorly, or superiorly, and may be complete (disloca- |
10 The Cervical Spine 237
A B
|
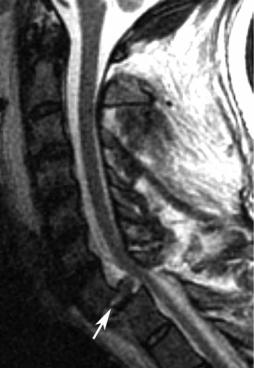
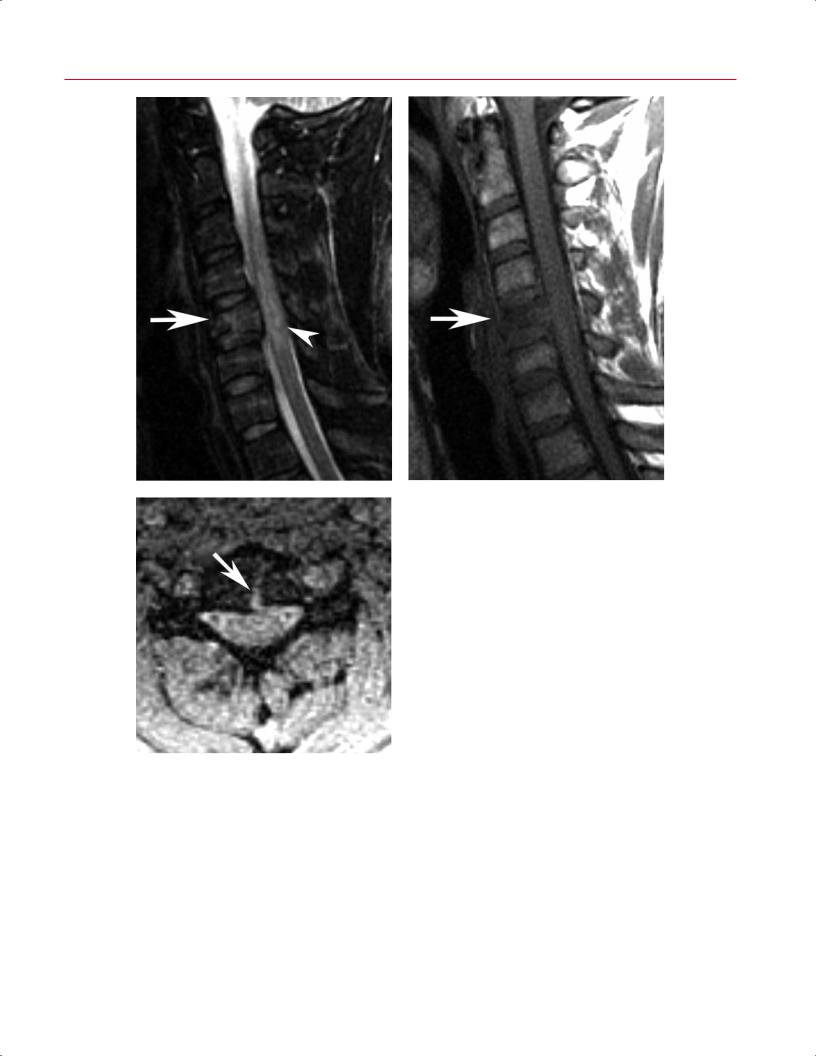
Fig. 10.8 Cervical burst fracture. Sagittal fat sup- |
|
pressed T2-weighted (A) and T1-weighted (B) images |
|
showing a C5 burst fracture (arrow on each) with |
|
moderate loss of height, retropulsion, and spinal cord |
|
contusion (arrowhead on A). (C) Axial T2-weighted |
C |
gradient-echo image shows the sagittal component |
of the fracture (arrow). |
tion) or partial (subluxation). Atlantooccipital dissociation |
occipital dissociation, whereas MRI is better at detecting in- |
|
can be a devastating injury.27–30 The primary injury is to |
jury to the cervicocranial ligaments (e.g., transverse, apical, |
|
the ligaments that provide structural support to the cervi- |
cruciate, atlantooccipital membrane and capsular ligaments, |
|
cocranial junction. In addition, even without frank disloca- |
tectorial membrane), brainstem, or spinal cord.11,19,31 |
|
tion, the occiput–C1 junction may be injured, as indicated by |
|
|
postmortem studies.27,28 Although this injury may be fatal, |
Trauma to the Atlas |
|
improvement in resuscitative and medical treatment has |
||
|
||
increased survival rates. CT imaging may be used to assess |
Axial load to the occipitocervical junction at the atlas may re- |
|
associated fractures or relationships among the basion, dens, |
sult in a burst fracture of the atlas. The injury is visualized on |
|
occipital condyles, and atlas in conjunction with atlanto- |
open-mouth odontoid radiographs or coronal CT images.32,33 |
 B
B