

- •Operative Cranial Neurosurgical Anatomy
- •Contents
- •Foreword
- •Preface
- •Contributors
- •1 Training Models in Neurosurgery
- •2 Assessment of Surgical Exposure
- •3 Anatomical Landmarks and Cranial Anthropometry
- •4 Presurgical Planning By Images
- •5 Patient Positioning
- •6 Fundamentals of Cranial Neurosurgery
- •7 Skin Incisions, Head and Neck Soft-Tissue Dissection
- •8 Techniques of Temporal Muscle Dissection
- •9 Intraoperative Imaging
- •10 Precaruncular Approach to the Medial Orbit and Central Skull Base
- •11 Supraorbital Approach
- •12 Trans-Ciliar Approach
- •13 Lateral Orbitotomy
- •14 Frontal and Bifrontal Approach
- •15 Frontotemporal and Pterional Approach
- •16 Mini-Pterional Approach
- •17 Combined Orbito-Zygomatic Approaches
- •18 Midline Interhemispheric Approach
- •19 Temporal Approach and Variants
- •20 Intradural Subtemporal Approach
- •21 Extradural Subtemporal Transzygomatic Approach
- •22 Occipital Approach
- •23 Supracerebellar Infratentorial Approach
- •24 Endoscopic Approach to Pineal Region
- •25 Midline Suboccipital Approach
- •26 Retrosigmoid Approach
- •27 Endoscopic Retrosigmoid Approach
- •29 Trans-Frontal-Sinus Subcranial Approach
- •30 Transbasal and Extended Subfrontal Bilateral Approach
- •32 Surgical Anatomy of the Petrous Bone
- •33 Anterior Petrosectomy
- •34 Presigmoid Retrolabyrinthine Approach
- •36 Nasal Surgical Anatomy
- •37 Microscopic Endonasal and Sublabial Approach
- •38 Endoscopic Endonasal Transphenoidal Approach
- •39 Expanded Endoscopic Endonasal Approach
- •41 Endoscopic Endonasal Odontoidectomy
- •42 Endoscopic Transoral Approach
- •43 Transmaxillary Approaches
- •44 Transmaxillary Transpterygoid Approach
- •45 Endoscopic Endonasal Transclival Approach with Transcondylar Extension
- •46 Endoscopic Endonasal Transmaxillary Approach to the Vidian Canal and Meckel’s Cave
- •48 High Flow Bypass (Common Carotid Artery – Middle Cerebral Artery)
- •50 Anthropometry for Ventricular Puncture
- •51 Ventricular-Peritoneal Shunt
- •52 Endoscopic Septostomy
- •Index

52 Endoscopic Septostomy
Stefania Acerno, Filippo Gagliardi, Elena V. Colombo, Cristian Gragnaniello, Anthony J. Caputy, and Pietro Mortini
52.1 Introduction
The endoscopic septostomy is a minimally invasive, intraventricular endoscopic procedure. It allows creating a communication between both the lateral ventricles by opening the septum pellucidum. It is indicated in case of obstructive mono-ventric- ular hydrocephalus.
Surgical access to the lateral ventricle is just lateral as compared to the standard approach for the placement of an external ventricular shunt.
52.2 Indications
•Mono-ventricular hydrocephalus due to tumoral or membranous (infammatory, post-hemorrhagic) obstruction in the region of foramina of Monro or fornix.
•Cysts of the septum pellucidum.
•Multi-loculated cystic hydrocephalus.
52.3 Patient Positioning (Fig. 52.1)
•Position: The patient is positioned supine with the head fxed to a three pins Mayfeld head-holder.
•Body: The body is placed parallel to the horizontal plane in neutral position.
•Head: The head is fexed 30° and the neck is kept in straight position.
52.4 Skin Incision (Fig. 52.1)
•Linear incision
○Incision is located just in front of the coronal suture, according to the selected entry point (see burr hole).
○The incision is 3 cm long.
•C-shaped incision
○The C-shaped incision is based toward the superfcial temporal artery.
○It is preferred if a cerebro-spinal fuid (CSF) reservoir needs to be implanted.
52.4.1 Critical Structures
• None
52.5 Soft Tissue Dissection
•Galea capitis and periosteum
○The galea capitis and periosteum are cut according to the shape of the skin incision.
Fig. 52.1 Patient positioning and landmarks. Abbreviations: Coronal suture (blue line).
52.5.1 Critical Structures
• None
52.6 Craniotomy/
Craniectomy (See Chapter 50)
•Single burr hole
○Burr hole is usually 10 mm wide.
○It is placed 5 to 7 cm away from the midline, on the side of the dilated ventricle, just anterior to the coronal suture according to the procedure:
-Pure septostomy: Hole is placed 5-7 cm paramedian in order to achieve the more perpendicular route to the septum pellucidum.
-Septostomy and endoscopic tumor procedures (biopsy or endoscopic excision) in the area of the foramina of
Monro: burr hole is placed 5 cm paramedian.
-Septostomy and endoscopic third ventriculostomy:
Hole is performed 4 cm away from the midline.
52.6.1 Critical Structures
• None
327
VII Ventricular Shunts Procedures
52.7 Dural Opening
•Cross-shaped fashion
○A cortical exposure of 5-7 mm is needed to put the endoscope in place.
52.7.1 Critical Structures
• None
52.8 Intradural Procedure
•Intradural procedure comprises the following steps:
○Leptomeningeal and cortex bipolar coagulation and incision.
○Ventricle tap with a standard catheter to verify accuracy of the planned trajectory and to sample CSF when needed for laboratory testing.
○Peel away or endoscopic sheath freehand positioning (with a dynamic reference frame on it, if neuro-navigation tools are used) and fxation on a pneumatic/mechanic holder covered by a sterile drape (see Chapter 27).
○Endoscope placement through the sheath.
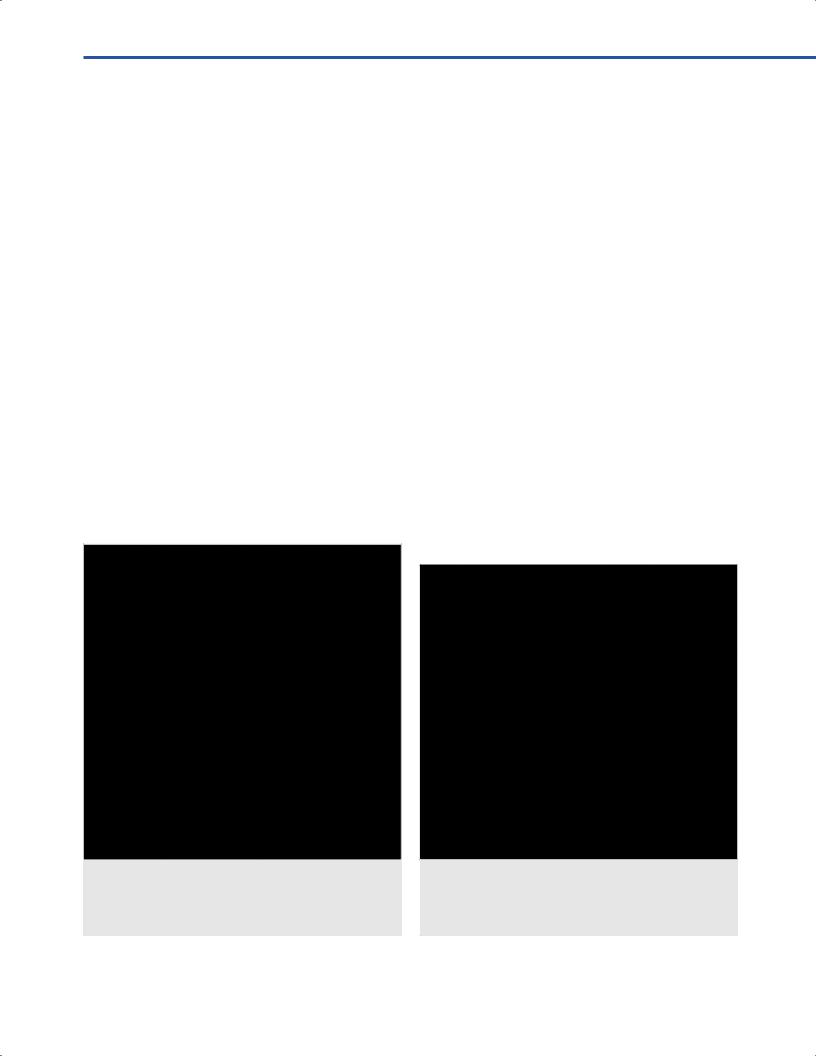
○Inspection of the ventricular cavity and identifcation of the local anatomy and landmarks (Fig. 52.2).
○Pulsated manual irrigation with lactate Ringer’s solution
36-37°C (always check that there is always one irrigation port unlocked to prevent dangerous spikes of intracranial pressure).
Fig. 52.2 Anatomic view.
Abbreviations. ASV = anterior septal vein; ChP = choroid plexus; CN = caudate nucleus; F = fornix; FH = frontal horn; MF = Monro foramen; SCV = superior choroidal vein; SP = septum pellucidum; SV = septal vein; T = thalamus; TSV = thalamostriate vein.
52.9 Septosotomy
•Identifcation of the adequate site of the septostomy (any area of the septum, according to each case, can be fenestrated).
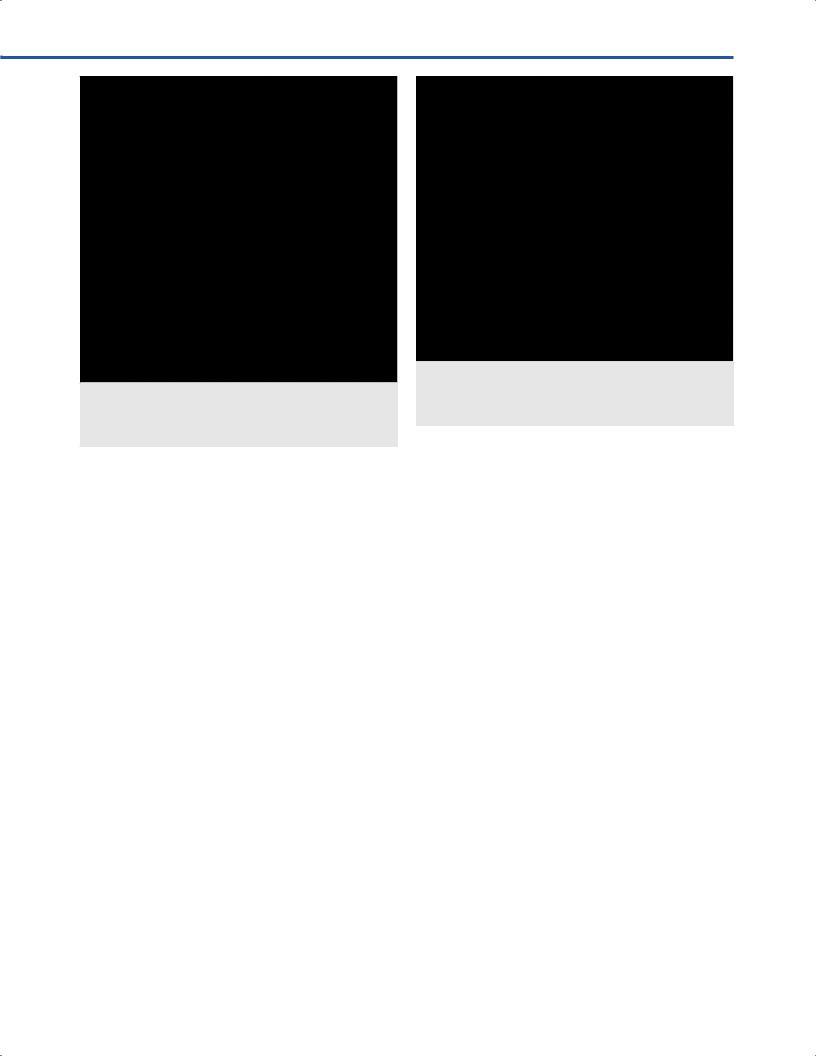
•“Ideal” zone to prevent injury to the fornix is the area 5 to
10 mm posterior to the foramen of Monro, midway between the corpus callosum and the fornix, carefully avoiding contact with the septal veins (Fig. 52.3).
•Bipolar/monopolar coagulation of the interest area in circumferential way.
•Cutting residual septum tissue with endoscopic scissors and grabbing the fap away with endoscopic forceps.
•Dilatation of the fenestration with a Fogarthy balloon
(3 French) until the size of 7 to 10 mm at least in diameter, to decrease chances of occlusion of the opening by scar formation (Fig. 52.4).
•Endoscopic inspection of contralateral ventricular camera to ensure the size is adequate and no bleeding problem in the opposite ventricle is ongoing (Fig. 52.5).
52.9.1 Suggestions
•When minor bleeding occurs, simple and continuous irrigation, for a few minutes, usually clears up the view.
•Bipolar diathermy can also be used to coagulate the vessel.
•In cases of sustained hemorrhage forced irrigation or CSF aspiration, in order to create a “dry feld,” can help in identifying the bleeding source and obtain hemostasis.
•Major bleeding problem can induce abortion of the procedure leaving in place a ventricular catheter to allow CSF to clear.
Fig. 52.3 Ident tion of landmarks in the ventricular cavity for septostomy.
Abbreviations: ChP = choroid plexus; CN = caudate nucleus;
FH = frontal horn; MF = Monro foramen; SP = septum pellucidum; T = thalamus.
328
52 Endoscopic Septostomy
Fig. 52.4 Endoscopic view after septostomy. Abbreviations: ChP = choroid plexus; LFH = left frontal horn;
LMF = left Monro foramen; LT = left thalamus; RFH = right frontal horn; RMF = right Monro foramen; SP = septum pellucidum.
52.9.2 Critical Structures
•Septal vein.
•Fornix.
•Contralateral thalamus.
52.10 Pearls
•Endoscopic septostomy should be performed only if the anatomy of the region of interest is clearly identifable both preoperatively by the neuroimaging and during the surgical procedure.
•Frameless neuro-navigation could be crucial to obtain the optimal entry point according to the procedure/s.
•When a simultaneous endoscopic tumor procedure is planned it is better to start with septostomy to prevent that bleeding from the tumor bed precludes the fenestration.
•In acute/subacute hydrocephalus the septum pellucidum is thick and highly fexible and could be difcult to coagulate and perforate; intermittent forced irrigation helps in identifying the thinnest part to perform safe and bloodless stomy.
Fig. 52.5 Endoscopic view of the controlateral ventricle. Abbreviations: ChP = choroid plexus; LCN = left caudate nucleus; LFH = left frontal horn; LMF = left Monro foramen; LT = left thalamus; SP = septum pellucidum.
•Water-jet dissection and endoscopic ultrasound probes, when available, could be an interesting variant in performing septostomy.
•The surgical feld should always be prepared and draped to allow a rapid switch to micro-neurosurgery in case of major hemorrhagic complication.
References
1Aldana PR, Kestle JR, Brockmeyer DL, Walker ML. Results of endoscopic septal fenestration in the treatment of isolated ventricular hydrocephalus. Pediatr Neurosurg 2003; 38(6):286–294.
2Miki T, Wada J, Nakajima N, Inaji T, Akimoto J, Haraoka J.
Operative indications and neuroendoscopic management of symptomatic cysts of the septum pellucidum. Childs
Nerv Syst 2005;21(5):372–381.
3Oertel JM, Schroeder HW, Gaab MR. Endoscopic stomy of the septum pellucidum: indications, technique, and results. Neurosurgery 2009;64(3):482–491, discussion 491–493.
4Schroeder HW. General principles and intraventricular neuroendoscopy: endoscopic techniques. World Neurosurg 2013;79(2, Suppl):S14.e23–14.e28.
329

53 Endoscopic Third Ventriculostomy and Biopsy of Pineal
Region
Joanna Kemp, Elena V. Colombo, and Samer K. Elbabaa
53.1 Indications
•Endoscopic third ventriculostomy (ETV)
○Symptomatic obstructive hydrocephalus.
○Patent subarachnoid spaces with adequate space between the clivus and the brainstem.
○Thinned/bowed foor of the third ventricle on sagittal MRI:
-Indicates likelihood of safe fenestration of the foor.
-Absence of this fnding is not an absolute contraindication.
•Pineal region biopsy
○Presence of a lesion in the pineal region or posterior third ventricle where pathologic diagnosis will signifcantly impact treatment options.
○Confrmation of absence of vascular lesion that would make biopsy contraindicated.
53.2 Patient Positioning
•Position: The patient is positioned supine with the head placed on a gel donut or Mayfeld horseshoe headrest.
•Body: The body is placed supine with the arm boards or arms tucked at the side; a bilateral shoulder roll has
to be used if head extension is desired for pineal region biopsy.
•Head: The head is kept neutral or with a slight fexion.
•The operating table is rotated 90 or 180° from anesthesia.
•Monitors are placed at the foot of the bed for the operating surgeon and assistant.
•A connection to the operating table for a pneumatic arm for the endoscope may be made.
53.3 Skin Incision
•Desired entry points are identifed
○Laterality: Right side is preferred in most cases; though if one lateral ventricle is larger than the other, the larger ventricle is utilized.
○ETV: 1 cm anterior to the coronal suture at the mid-pupil- lary line. In infants with a patent anterior fontanelle, this can be marked at the junction of the fontanelle and the ipsilateral coronal suture
○Pineal region biopsy: Depending on the anatomy of the third ventricle and location of the lesion, a more anterior entry may be required. Simultaneous ETV and pineal region biopsy may require multiple burr holes or a single hole midway between both trajectories
○Neuronavigation: Particularly useful in pineal region biopsy to identify target intraoperatively and defne entry, or to plan trajectory in patients with small ventricles or abnormal ventricular morphology. It can be used in any case for optimization of entry point
•C-shaped or linear incision large enough to accommodate one or multiple burr holes is made (Fig. 53.1).
53.3.1 Critical Structures
•Identifcation of the midline.
•Coronal suture.
•Anterior fontanelle.
53.4 Soft Tissue Dissection
•Skin is opened sharply.
•Subcutaneous fat and galea may be opened sharply or with monopolar electrocautery.
•Pericranium is opened with monopolar in the location of the entry point.
•Care is taken to avoid injury to the anterior fontanelle when present.
•Skin fap is retracted with suture or a self-retaining retractor.
Fig. 53.1 Patient positioned supine on a Ma ld horseshoe head holder. Note the marking of midline and the C-shaped incision at the mid pupillary line.
330

53 Endoscopic Third Ventriculostomy and Biopsy of Pineal Region
53.4.1 Critical Structures |
- Veins: Internal cerebral veins. |
|
|
- Recesses: Optic, infundibular, pineal, prepontine cistern. |
|
• Coronal suture. |
- |
Clivus. |
• Anterior fontanelle. |
- |
Cerebral aqueduct. |
53.5 Craniotomy
•Entry point identifcation
○Repeat identifcation and update entry with neuronavigation, if utilized.
○Entry point is always identifed anterior to the coronal suture.
•Burr holes
○With patent anterior fontanelle, the entry point can be created using Kerrison punches at the anterolateral edge of the fontanelle.
○Without patent anterior fontanelle, the entry point is created with a pneumatic drill, Hudson brace, or hand twist drill with hole large enough to accommodate peel away sheath and endoscope.
53.6 Dural Opening
•Dura is opened in a cruciate fashion.
•Bipolar electrocautery is used to coagulate dural edges
○Good hemostasis is important to prevent run down of blood products that would obscure view with endoscope.
53.8 Pearls
•ETV (Fig. 53.5–53.7)
○0° Rigid endoscope is the most often utilized.
-30° Endoscope should be available if visualization is inadequate with the 0° scope.
-Flexible scopes may be useful in cases of difcult trajectory, though optics are lower quality.
○Fenestration is performed anterior to the mammillary bodies and basilar apex at the midline.
○Basilar apex can be identifed through thinned foor (tuber cinereum).
○If the foor is opaque, attempts at hydrodissection or endoscopic coring of the foor may still allow visualization and safe fenestration.
○Endoscope, blunt forceps, monopolar, laser, and Fogarty balloon have all been described as instruments used to make initial fenestration.
-Use of monopolar and laser must be used cautiously due to risk of thermal injury to the underlying basilar artery.
○Widening of the fenestration can be done with infation of a Fogarty balloon or spreading of blunt forceps.
53.7 Intradural Exposure
•Cannulation of ventricle (Fig. 53.2)
○The determination of depth is based on the measurement of cortical mantle on MRI preoperatively.
○Peel away sheath is inserted to depth adequate to just enter the ependyma of the lateral ventricle.
○The inner cannula is removed to confrm cerebrospinal fuid (CSF) fow.
-CSF is sampled if a specimen is desired.
-Endoscope is inserted for initial confrmation of ventricular access.
-Sheath is peeled away to the appropriate depth and stapled to skin and/or drapes.
○Confrmation of side of entry.
-Neuronavigation.
-Anatomic landmarks.
•Navigation of endoscope
○Identifcation of landmarks within the lateral ventricle
(Fig. 53.3).
-Foramen of Monro
-Fornix
-Choroid plexus
-Septum pellucidum
-Veins: Septal and thalamostriate
○Identifcation of landmarks within the third ventricle
(Fig. 53.4)
-Neural structures: Optic chiasm, tuber cinereum, hypothalamus, thalamus, inter-thalamic adhesion, habenular commissure, posterior commissure.
-Arteries: Basilar artery, perforating branches.
Fig. 53.2 Initial insertion of the endoscope after cannulation of the ventricle through a peel away sheath.
331
VII Ventricular Shunts Procedures
Fig. 53.3 View from the endoscope after cannulation of the right lateral ventricle.
Abbreviations: CP = choroid plexus; F = fornix; MB = mammillary body; MF = Monro foramen; SP = septum pellucidum; SV = septal vein; T = thalamus; TSV = thalamostriate vein.
Fig. 53.4 View of t |
he third ventricle through the right |
foramen of Monro. |
|
Abbreviations: AC = anterior commissure; BA = basilar artery; F = fornix; IR = infundibular recess; MB = mammillary body; OR = optic recess; PCA = posterior cerebral artery; PCom = posterior communicating artery; TC = tuber cinereum.
Fig. 53.5 Fenestration of t he third ventricle using a Fogarty balloon anterior to the basilar apex and posterior to the infundibular recess.
Abbreviations: BA = basilar artery; FC = Fogarty catheter; IR = infundibular recess; MB = mammillary body; PCA = posterior cerebral artery; PCom = posterior communicating artery.
Fig. 53.6 Floor of the third ventricle after the fenestration. Abbreviations: BA = basilar artery; F = fornix; FE = fenestration; IR = infundibular recess; MB = mammillary body; PCA = posterior cerebral artery; PCom = posterior communicating artery.
332

53 Endoscopic Third Ventriculostomy and Biopsy of Pineal Region
○Inspection of the cistern is required to ensure adequate opening of arachnoid adhesions or the membrane of Liliequist which may be present deep to the tuber cinereum.
•Pineal region biopsy
○If ETV and pineal biopsy are planned in the same setting, the ETV should be performed frst to ensure treatment of hydrocephalus prior to the added potential for bleeding or decreased visualization that may come along with biopsy.
○May require the use of rigid 0 or 30° endoscopes, or fexible endoscope depending on ventricular size, trajectory, and entry point.
○Neuronavigation is helpful to identify the most appropriate site for biopsy, particularly in cases when the lesion does not clearly breach the ependyma.
○Minimization of cautery aids in improving likelihood of achieving pathologic diagnosis.
○Samples are taken with a blunt cup forceps through the working channel of the endoscope.
○Small venous hemorrhages from the capsule or tumor can be controlled with irrigation, Fogarty balloon tamponade, or electrocautery.
•Complication management and avoidance
○Trajectory and entry point should be chosen to reduce the risk of traction on the fornix.
○Sweeping motions of the endoscope are more likely to produce traction and pressure on the fornix and cause injury.
Fig. 53.7 Explicative case.(A) View from the endoscope after cannulation of the right lateral ventricle. (B) View of the floor of the third ventricle through the right foramen of Monro. (C) Fenestration of the floor of the third ventricle using a Fogarty balloon. (D) Floor of the third ventricle after the fenestration.
Abbreviations: BA = basilar artery; CP = choroid plexus; F = fornix;
FC = Fogarty catheter; FE = fenestration; IR = infundibular recess; MB = mammillary body; MF = Monro foramen; OR = optic recess; PCA = posterior cerebral artery; SP = septum pellucidum; T = thalamus;
TC = tuber cinereum; TSV = thalamostriate vein.
○Venous bleeding can most often be controlled with irrigation, balloon tamponade, or cautery.
○In cases where bleeding makes visualization impossible, the surgeon must be prepared to abort and leave behind an external ventricular drain (EVD).
○Communication with the anesthesia team is necessary during fenestration, as the patient can experience bradycardia.
○Arterial hemorrhage or basilar injury is rare but best avoided with good identifcation of landmarks prior to proceeding with fenestration.
References
1.Bouramas D, Paidakakos N, Sotiriou F, Kouzounias K, Sklavounou M, Gekas N. Endoscopic third ventriculostomy in obstructive hydrocephalus: surgical technique and pitfalls. Acta Neurochir Suppl (Wien) 2012;113:135–139.
2.Chibbaro S, Di Rocco F, Makiese O, et al. Neuroendoscopic management of posterior third ventricle and pineal region tumors: technique, limitation, and possible complication avoidance. Neurosurg Rev 2012;35(3):331–338, discussion 338–340.
3.Constantini S, Mohanty A, Zymberg S, et al. Safety and diagnostic accuracy of neuroendoscopic biopsies: an international multicenter study. J Neurosurg Pediatr 2013; 11(6):704–709.
333

VII Ventricular Shunts Procedures
4.Hermann EJ, Esmaeilzadeh M, Ertl P, Polemikos M, Raab P, Krauss JK. Endoscopic intracranial surgery enhanced by electromagnetic-guided neuronavigation in children. Childs Nerv Syst 2015;31(8):1327–1333.
5.Jallo GI, Kothbauer KF, Abbott IR. Endoscopic third ventriculostomy. Neurosurg Focus 2005;19(6):e11.
6.Limbrick DD Jr, Baird LC, Klimo P Jr, Riva-Cambrin J, Flannery AM; Pediatric Hydrocephalus Systematic Review and Evidence-Based Guidelines Task Force. Pediatric
hydrocephalus: systematic literature review and evidence-based guidelines. Part 4: Cerebrospinal fuid shunt or endoscopic third ventriculostomy for the treatment of hydrocephalus in children. J Neurosurg Pediatr 2014;14(suppl 1):30–34.
7.Navarro R, Gil-Parra R, Reitman AJ, Olavarria G, Grant JA, Tomita T. Endoscopic third ventriculostomy in children: early and late complications and their avoidance. Childs
Nerv Syst 2006;22(5):506–513.
334