

29 Trans-Frontal-Sinus Subcranial Approach
Nicola Boari, Filippo Gagliardi, Alfo Spina, and Pietro Mortini
29.1 Introduction
The trans-frontal-sinus subcranial approach is well suited for the treatment of tumors of the median anterior skull base. This technique provides early devascularization of the tumor by division of the ethmoidal arteries, direct tumor access from the base, atraumatic frontal lobes decompression, broad exposure of sphenoid and ethmoidal sinuses. It also provides good visual exposure for the dissection of the optic nerves and anterior cerebral arteries, and afords access to a pedicled pericranial fap for dural reconstruction.
29.2 Indications
•Olfactory grove and planum sphenoidale meningiomas.
•Tuberculum sellae and diaphragma sellae meningiomas.
•Giant pituitary adenomas.
•Clival chordomas.
•Esthesioneuroblastomas.
•Malignancy of the anterior skull base - sinonasal tumors.
29.3 Patient Positioning
•Position: The patient is positioned supine with the head fxed to a horseshoe head holder.
•Body: The body is placed in neutral position with the trunk elevated 30° to increase venous backfow and the legs elevated at the level of the heart.
•Head: The head is in neutral position, elevated 15° and extended 20° with the vertex kept downward.
•Anti-decubitus devices: Rolls are placed under the knees.
•The zygoma has to be the highest point in the surgical feld.
29.4 Skin Incision
•Coronal incision (See Chapters 6 and 7)
○Starting point: Incision starts 1 cm anterior and above the tragus.
○Run: Incision line should stay behind the hairline.
○Ending point: It ends 1 cm anterior and above the tragus of the contralateral side.
29.4.1 Critical Structures
•Superfcial temporal artery.
•Facial nerve.
29.5 Soft Tissues Dissection (Fig. 29.1)
•Myofascial level
○A subgaleal dissection posterior to the coronal plane of the incision may be performed to maximize the length of the pericranial fap.
○The pericranial fap is then gently elevated from the cranial vault from posterior to anterior.
Fig. 29.1 Frontonasal osteotomy. The osteotomy of the anterior wall of the frontal sinus is performed using an oscillating
saw (dotted lines).
Abbreviations: FB = frontal bone; FSAW = frontal sinus anterior wall; PC = pericranium; PO = periorbit;
SON = supraorbital nerve; TM = temporal muscle; ZP = zygomatic process.
172
29 Trans-Frontal-Sinus Subcranial Approach
•Muscles
○Temporal fascia and muscle are not detached from the temporal fossa.
•Bone exposure
○The scalp is raised forward to expose the supraorbital ridge bilaterally and the nasal process of the frontal bone up to the fronto-naso-maxillary suture in the midline.
○The periorbit is detached from the superior and medial wall of the orbit on both sides.
•Supraorbital nerve and artery
○They can be freed from the supraorbital notch bilaterally to avoid traction on the orbital contents.
29.5.1 Critical Structures
•Supraorbital nerve and artery.
•Periorbit.
•Lacrimal gland.
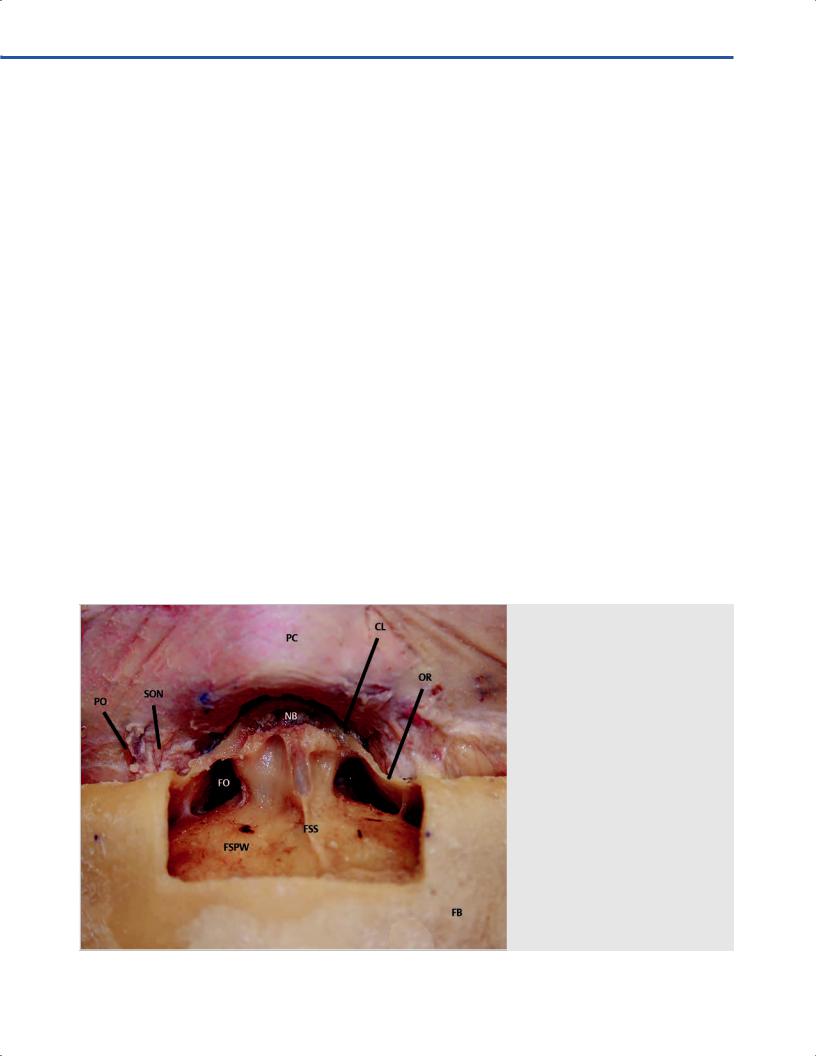
29.6 Osteotomy (Fig. 29.2)
An osteotomy of the anterior wall of the frontal sinus, including the upper medial aspect of the superior orbital rims is performed with a reciprocating saw.
•Cuts
○I: The frst cut is made at the nasofrontal suture on the axial plane down the medial orbital wall and along the nasomaxillary grooves just anterior to the lacrimal crest.
○II and III: Two symmetric cuts are made medial to the supraorbital notch vertically on the sagittal plane.
○IV: A horizontal cut is made on the axial plane across the frontal bones, connecting the previous two, at a level corresponding to the superior limit of the frontal sinus.
29.7 Anterior Skull Base Exposure
•The anterior wall of the sinus is lifted after fracturing the frontal intersinus septa with a chisel.
•Intersinus septa are removed with a rongeur. The mucosa lining the anterior and posterior walls of the sinus is resected
(Fig. 29.3).
•Posterior sinus wall is thinned using a diamond drill and piecemeal removed using a Kerrison punch.
•Frontal dura is dissected from the apex and lateral surfaces of the crista galli, which is detached from the ethmoidal cribriform plate, and removed.
•Dissection in a subperiorbital plane along the medial wall of the orbit is performed to identify the anterior and posterior ethmoidal arteries, which are coagulated and divided bilaterally (Fig. 29.4).
•The falx with the origin of the superior sagittal sinus are coagulated and cut.
•Bone from the medial orbital walls is removed and the ethmoid can be drilled to obtain access to the nasal and sphenoethmoidal cavities and to the upper clivus.
•Drilling of the planum sphenoidalis up to the tuberculum sellae can be accomplished (Fig. 29.5).
•The medial optic canals can be unroofed bilaterally to perform an extradural optic nerves and chiasm decompression.
29.7.1 Critical Structures
•Anterior and posterior ethmoidal arteries.
•Internal carotid arteries (ICAs) (C4 and C5 segments).
•Optic nerves and chiasm.
Fig. 29.2 By removing the bony wall and the sinus mucosa the posterior wall of the sinus comes into view.
Abbreviations: CL = canthal ligament; FB = frontal bone; FO = frontal ostium; FSPW = frontal sinus posterior wall; FSS = frontal sinus septum; NB = nasal
bone; OR = orbital roof; PC = pericranium; PO = periorbit; SON = supraorbital nerve.
173

III Cranial Approaches
Fig. 29.3 After drilling the posterior sinus wall the frontal dura is exposed. Abbreviations: FB = frontal bone; FD = frontal dura; FSP = frontal sinus pneumatization;
NB = nasal bone; PC = pericranium; PO = periorbit; SON = supraorbital nerve; dotted line depicts the following dural opening.
Fig. 29.4 Crista galli is detached from the frontal dura and from nasal mucosa and the anterior and posterior ethmoidal arteries are skeletonized and divided. Olfactory grooves dura is cut with the olfactor s. Abbreviations: FD = frontal dura; NM = nasal mucosa; OGD = olfactory groove dura; PC
= pericranium; PEA = posterior ethmoidal artery; PO = periorbit; rCG = resected crista galli; SON = supraorbital nerve.
29.8 Dural Opening (Fig. 29.6)
•The dura is divided circumferentially around the olfactory groove.
29.8.1 Critical Structures
• Optic nerves and chiasm.
29.9 Intradural Exposure (Fig. 29.7)
•Parenchymal structures: Basal frontal lobes.
•Arachnoidal layer: Chiasmatic cistern.
•Cranial nerves: Optic and olphactory nerves.
•Arteries: Anterior communicating artery (ACoA), anterior cerebral artery (A1 and A2 segments), Heubner’s arteries.
•Veins: Anterior aspect of the superior sagittal sinus.
174
29 Trans-Frontal-Sinus Subcranial Approach
29.10 Reconstruction
•Dural defect is repaired by using a free pericranium patch sutured to the dural edges with a 6/0 prolene under microscopic magnifcation.
•The suture is sealed with fbrin glue.
•A wide pedicled frontal pericranial fap is harvested and then refected along the anterior skull base. The fap is fxed with fbrin glue.
•Abdominal fat can be positioned to fll the dead space inside the pedicle pericranial fap.
Fig. 29.5 After performing the ethmoidectomy and opening of the sphenoid sinus, the se , carotid, and optic protuberances come into view.
Abbreviations: CB = clival bone; FD = frontal dura; LICAP = left internal carotid artery prominence; LONP = left optic nerve prominence; P = planum; RICAP = right internal carotid artery prominence; RONP = right optic nerve prominence; S = sella; SS = sphenoid sinus; SSS = sphenoid sinus septum.
Fig. 29.6 Frontal dura is divided circumferentially exposing the olfactory bulbs and tracts and the frontal lobes. Abbreviations: F = falx; FD = frontal dura; LFL = left frontal lobe; LICA = left internal carotid artery; LON = left optic nerve;
ONs = olfactory nerves; PC = pericranium; RFL = right frontal lobe; RICA = right internal carotid artery; RON = right optic nerve; SD = sellar dura; SS = sphenoid sinus.
•The anterior wall of the frontal sinus is repositioned and fxed with micro titanium screws and plates.
•A lumbar drain can be positioned if a watertight closure could not be obtained.
29.11Pearls
•For small frontal sinuses, bone fap has to be extended beyond the limits of the sinus, including the external layer of the frontal vault, which is cut tangentially.
175

III Cranial Approaches
•Identifcation, coagulation and section of anterior and posterior ethmoidal arteries is crucial in obtaining an early devascularization of the tumor.
•Extensive drilling of the ethmoidal bone allows for an early tumor debulking from below, without any retraction on the frontal lobes; the tumor tends to collapse downward, pushed down by the re-expansion of the edematous frontal lobes.
•Dissection and removal of the posterior pole of the tumor has to be done very carefully in order to identify and preserve the anterior cerebral arteries (ACAs) with the anterior communicating artery (ACoA), that are usually covered by tumor.
•Meticulous multilayer dural reconstruction is crucial in order to avoid cerebrospinal fuid (CSF) leak through the nose.
Fig. 29.7 By slight retraction of the frontal lobes, optic nerves, chiasm, and pituitary stalk come into view.
Abbreviations: LFL = left frontal lobe; LICA = left internal carotid artery; LON = left optic nerve; OC = optic chiasm; PS = pituitary stalk; RFL = right frontal lobe; RICA = right internal carotid artery; RON = right optic nerve; SD = sellar dura.
References
1.Boari N, Gagliardi F, Roberti F, Barzaghi LR, Caputy AJ, Mortini P. The trans-frontal-sinus subcranial approach for removal of large olfactory groove meningiomas: surgical technique and comparison to other approaches. J Neurol Surg A Cent Eur Neurosurg 2013;74(3):152–161
2.Gagliardi F, Boari N, Mortini P. Reconstruction techniques in skull base surgery. J Craniofac Surg 2011;22(3):1015–1020
3.Hallacq P, Moreau JJ, Fischer G, Béziat JL. Trans-sinusal frontal approach for olfactory groove meningiomas. Skull Base 2001;11(1):35–46
4.Raveh J, Turk JB, Lädrach K, et al. Extended anterior subcranial approach for skull base tumors: long-term results. J Neurosurg 1995;82 (6):1002–1010
176