


18 Midline Interhemispheric Approach
Marzia Medone, Filippo Gagliardi, Cristian Gragnaniello, Anthony J. Caputy, Pietro Mortini, and Remi Nader
18.1 Introduction
The interhemispheric approach is a midline transcranial approach, which provides access through this anatomical corridor to the corpus callosum and the ventricular system. The craniotomy can be easily tailored according to the pathology and to the venous anatomy, which is one of the main limiting factor of surgical maneuverability.
Callosotomy provides access to the lateral ventricle and to the third ventricle, either through the foramen of Monro or through the choroidal fssure.
The approach is indicated for extra-axial tumors involving the interhemispheric fssure, as well as intra-axial lesions located in the anterior aspect of the third ventricle and lateral ventricles.
18.2 Indications
•Vascular and neoplastic lesions located in the anterior aspect of the third ventricle, including lesions extending out of the third ventricle into the lateral ventricles.
○Tumors of the third ventricle including gliomas, ependymomas, choroid plexus papillomas, meningiomas, craniopharyngiomas.
○Colloid cysts.
○Vascular malformations.
•Extra-axial tumors of the interhemispheric fssure (i.e., falx or parasagittal meningiomas).
Fig. 18.1 Skin incision (red dotted line).
Abbreviations: CS = coronal suture; LE = left ear; M = midline; N = nose; RE = right ear.
18.3 Patient Positioning
•Position: The patient is positioned supine or lateral decubitus with the head fxed with a Mayfeld head holder.
•Body: The body is lined horizontally.
•Head: The head is fexed 15 to 30°, depending on the location of the lesion.
○Ending point: Incision ends at the superior attachment of the temporal muscle controlaterally.
18.4.1 Critical Structures
•Superfcial temporal artery.
•Auriculo-temporal nerve.
18.4 Skin Incision (Fig. 18.1)
•U-shaped unilateral incision
○An area of approximately 5x5 cm centered on the bregma is shaved, prepped and draped.
○A U-shaped horseshoe scalp incision is made with the open end of the “U” pointing laterally.
○Starting point: The incision starts just behind the hairline,
5 cm lateral from the midline.
○Course: It runs 1/3 anterior and 2/3 posterior to the coronal suture.
○Ending point: Incision ends the same as the starting but more posterior.
•Linear ¾ Suttar or bicoronal incision
○Starting point: The incision starts just above the pinna.
○Course: It runs along the coronal suture.
18.5 Soft Tissues Dissection
•Myofascial level
○The myofascial level is incised according to skin incision.
○It is important to preserve the pericranial layer, for further reconstruction.
•Muscles
○Although the temporal muscle is exposed by the skin incision, there is no need to incise it, thus it is preserved.
•Bone exposure
○The bone exposure is completed when the frontal and parietal bony surface are exposed for about 5x5 cm.
○Antero-posterior extension of the bone exposure has to run 1/3 anterior and 2/3 posterior to the coronal suture.
○Lateral exposure extends up to the temporal muscle attachment on the ipsilateral side.
○The sagittal suture has to be exposed on the midline.
113
III Cranial Approaches
18.6 Craniotomy/
Craniectomy (Figs. 18.2,18.3)
Midline coronal craniotomy
•Burr holes
○I: The frst burr hole has to be placed along the midline about 2 to 3 cm anterior to the coronal suture.
○II: The second burr hole is made along the midline about
3 to 4 cm posterior to the coronal suture.
•Cuts
○The frst cut is made between the two burr holes, laterally in a U-shaped fashion with a lateral extension reaching the superior temporal line.
○The second cut is made along the sagittal sinus.
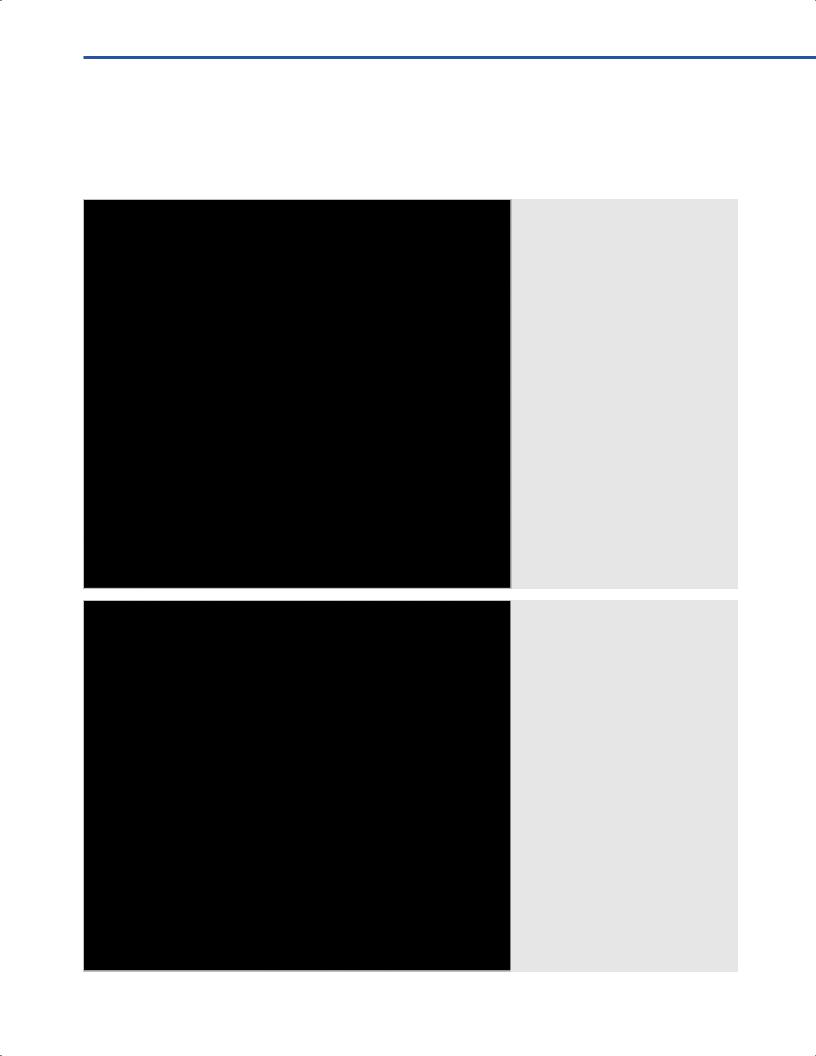
Fig. 18.2 Craniotomy landmarks (black dotted line).
Abbreviations: CS = coronal suture; FB = frontal bone st burr hole; II = second burr hole; P = pericranium; PB = parietal bone; S = skin.
Fig. 18.3 Craniotomy.
Abbreviations: CS = coronal suture; FB = frontal bone st burr hole; II = second burr hole; P = pericranium; PB = parietal bone; S = skin.
114

18 Midline Interhemispheric Approach
•Craniotomy landmarks
○Medially: The sagittal suture on the midline.
○Laterally: The superior temporal line.
○Rostrally: An ideal line parallel to the coronal plane, which runs 2 cm anterior to coronal suture.
○Caudally: An ideal line parallel to the coronal plane, which runs 3 to 4 cm posterior to coronal suture.
18.6.1 Variants
•Burr holes
○Four burr holes, straddling the superior sagittal sinus may alternatively be made.
○Two of them are made anteriorly and the remaining two posteriorly.
○This technical variant aims to increase safety in and avoid injuring the sinus, and it is mostly advised in elderly patients.
○An extra burr hole might be made laterally, in cases where the dura is tightly adherent to the bone in order to achieve a better dural dissection.
18.6.2 Critical Structures
•Superior sagittal sinus.
•Dural venous lakes.
•Motor cortex below the dura and posterior to the coronal suture.
18.7 Dural Opening (Fig. 18.4)
•The dura is opened in a C-shaped fashion.
•The edges of dural incision are based on the superior sagittal sinus.
•The fap is refected along the midline.
•The ends of the dural incision have to be kept close to, but not violating the sagittal sinus.
18.7.1Critical Structures
•Superior sagittal sinus.
•Venous lakes.
•Parasagittal draining veins.
•Motor cortex.
18.8 Intradural Exposure (Figs. 18.5, 18.6)
•Parenchymal structures: Fronto-parietal cortex, cingulate gyrus, corpus callosum.
•Arachnoidal layer: Interhemispheric fssure and cistern.
•Arteries: Callosomarginal and pericallosal arteries, distal anterior cerebral artery (ACA).
•Veins: Bridging cortical veins, superior sagittal sinus.
18.8.1 Details of Intradural Exposure
•Brain retractors are placed on the ipsilateral cerebral hemisphere in the interhemispheric fssure and gentle retraction is applied.
•A gentle dissection with gradual advancement of the retractors is used to visualize the corpus callosum.
•Care must be taken to accurately defne the corpus callosum and to avoid injury to the pericallosal arteries.
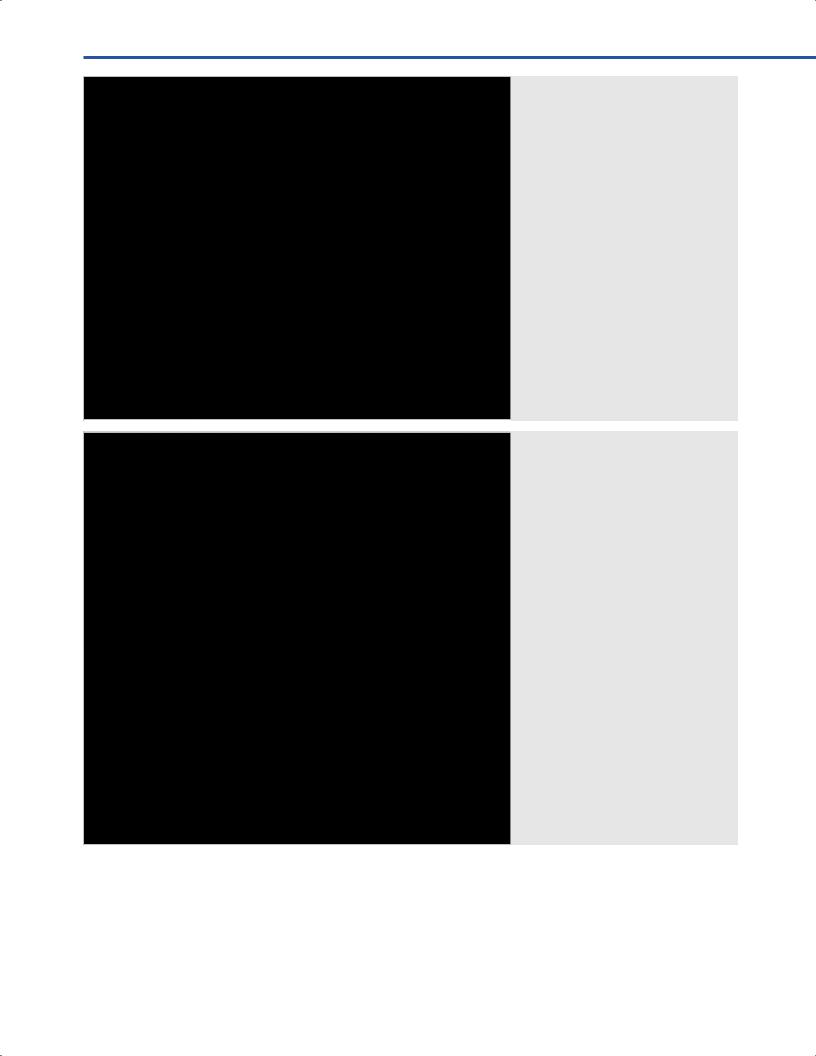
Fig. 18.4 Dural opening.
Abbreviations: DM = dura mater; IL = incision line; P = pericranium; S = skin; SSS = superior sagittal sinus.
115
III Cranial Approaches
18.9 Intraventricular
Exposure (Fig. 18.7)
18.9.1 Approach to the Lateral Ventricle
•A 1 cm midline incision is made along corpus callosum fbers.
•The incision is kept less than 2 cm to decrease the risk of disconnection syndrome.
Fig. 18.5 Brain retraction and opening of
the interhemispher |
sure. |
Abbreviations: DM = dura mater; |
|
IF = interhemispher |
sure; P = pericrani- |
um; R = retractor; S = skin; SFG = superior frontal gyrus; SSS = superior sagittal sinus.
Fig. 18.6 Exposure of the corpus callosum. Callosotomy (black dotted line). Abbreviations: AMFA = anterior medial frontal artery; C = callosotomy; CC = corpus callosum; CG = cingulate gyrus; CMA = callosomarginal artery; F = falx; PCA = pericallosal artery; R = retractor.
•The retractors should now be advanced in order to visualize the choroidal fssure.
•The choroidal fssure is opened between the thalamus and the fornix and might be split by opening the tela choroidea.
•The fornix is displaced allowing visualization of the third ventricle.
116

18 Midline Interhemispheric Approach
18.9.2 Approaches to the Third Ventricle
•Transforaminal approach
○The choroid plexus is followed anteriorly to the foramen of Monro.
○Monro foramen is usually enlarged in case of hydrocephalus, improving surgical maneuverability.
○When it is unclear which ventricle is entered, the laterally placed thalamostriate vein will assist the surgeon with the orientation.
○The choroid plexus is cauterized, to minimize the chance of bleeding.
○At the end of the procedure the septum pellucidum should be opened to prevent univentricular hydrocephalus.
•Subchoroidal approach
○The choroidal fssure, which is in continuity with the superior part of the tela choroidea is exposed.
○The terminal branch of the thalamostriate (preferentially) or septal vein may be sacrifced in order to enter the third ventricle after division of the choroidal fssure.
○When the septal vein is divided, additional separation of the internal cerebral veins is necessary, whereas when the thalamostriate vein is sacrifced separation of the internal cerebral veins is not needed.
•Interforniceal approach
○A wide dissection of the septum pellucidum is performed.
○The frst lateral ventricle is entered.
Fig. 18.7 Callosotomy and opening of the third ventricle.
Abbreviations: AMFA = anterior medial frontal artery; CC = corpus callosum; CG = cingulate gyrus; CMA = callosomarginal artery; CP = choroid plexus; FH = frontal horn; MF = Monro foramen; PCA = pericallosal artery; R = retractor.
○Interforniceal dissection is carried out under direct vision of both fornices.
○The internal cerebral veins are widely separated and the tela choroidea is dissected.
18.9.3 Critical Structures
•Thalamus as well as the surrounding large veins including the thalamostriate vein during the deep portion of the approach.
•Corpus callosum (disconnection syndrome or mutism)
•Fornix (memory loss).
References
1.Connolly ES, McKhann GM II, Huang J. Fundamentals of operative techniques in neurosurgery. New York, NY: Thieme
Medical Publishers; 2011
2.Fossett D, Caputy AJ. Operative neurosurgical anatomy. New York, NY: Thieme Medical Publisher; 2002
3.Greenberg MS. Handbook of neurosurgery. New York, NY: Thieme Medical Publishers; 2010
4.Sekhar LN, Fessler RG. Atlas of neurosurgical techniques. Brain. Volume 1. New York, NY: Thieme Medical Publishers; 2016
117