

- •Operative Cranial Neurosurgical Anatomy
- •Contents
- •Foreword
- •Preface
- •Contributors
- •1 Training Models in Neurosurgery
- •2 Assessment of Surgical Exposure
- •3 Anatomical Landmarks and Cranial Anthropometry
- •4 Presurgical Planning By Images
- •5 Patient Positioning
- •6 Fundamentals of Cranial Neurosurgery
- •7 Skin Incisions, Head and Neck Soft-Tissue Dissection
- •8 Techniques of Temporal Muscle Dissection
- •9 Intraoperative Imaging
- •10 Precaruncular Approach to the Medial Orbit and Central Skull Base
- •11 Supraorbital Approach
- •12 Trans-Ciliar Approach
- •13 Lateral Orbitotomy
- •14 Frontal and Bifrontal Approach
- •15 Frontotemporal and Pterional Approach
- •16 Mini-Pterional Approach
- •17 Combined Orbito-Zygomatic Approaches
- •18 Midline Interhemispheric Approach
- •19 Temporal Approach and Variants
- •20 Intradural Subtemporal Approach
- •21 Extradural Subtemporal Transzygomatic Approach
- •22 Occipital Approach
- •23 Supracerebellar Infratentorial Approach
- •24 Endoscopic Approach to Pineal Region
- •25 Midline Suboccipital Approach
- •26 Retrosigmoid Approach
- •27 Endoscopic Retrosigmoid Approach
- •29 Trans-Frontal-Sinus Subcranial Approach
- •30 Transbasal and Extended Subfrontal Bilateral Approach
- •32 Surgical Anatomy of the Petrous Bone
- •33 Anterior Petrosectomy
- •34 Presigmoid Retrolabyrinthine Approach
- •36 Nasal Surgical Anatomy
- •37 Microscopic Endonasal and Sublabial Approach
- •38 Endoscopic Endonasal Transphenoidal Approach
- •39 Expanded Endoscopic Endonasal Approach
- •41 Endoscopic Endonasal Odontoidectomy
- •42 Endoscopic Transoral Approach
- •43 Transmaxillary Approaches
- •44 Transmaxillary Transpterygoid Approach
- •45 Endoscopic Endonasal Transclival Approach with Transcondylar Extension
- •46 Endoscopic Endonasal Transmaxillary Approach to the Vidian Canal and Meckel’s Cave
- •48 High Flow Bypass (Common Carotid Artery – Middle Cerebral Artery)
- •50 Anthropometry for Ventricular Puncture
- •51 Ventricular-Peritoneal Shunt
- •52 Endoscopic Septostomy
- •Index

42 Endoscopic Transoral Approach
Edward E. Kerr, Lamia Buohliqah, Farid M. Elhefnawi, Ricardo L. Carrau, and Daniel M. Prevedello
42.1 Introduction
The endoscopic transoral approach is a midline approach to the craniocervical junction. It is suitable for surgical exposure of the clivus, as well as the anterior aspect of the magnum foramen, the atlas, and the axis (C1 and C2).
Surgical exposure can be further widened laterally through the retrostyloid approach gaining access to the jugular foramen region.
The midline approach is indicated for extradural lesions involving the anterior aspect of the craniovertebral junction. The lateral variants are instead indicated to treat lesions involving the jugular foramen, lower cranial nerves.
42.2 Indications
42.2.1 Midline Approach to the Craniovertebral Junction
•Extradural neoplasms (chordoma, chondrosarcoma) situated in the anterior midline craniovertebral junction region.
•Cord-compressive masses (such as reactive pannus secondary to trauma or rheumatoid diseases) situated anteriorly to the lower cranial nerves, at the craniovertebral junction in the setting of a contraindication to an endonasal approach.
42.2.2 Parapharyngeal Retrostyloid
Approach
•Paragangliomas situated mostly or entirely caudal to the jugular foramen.
•Benign peripheral nerve tumors (schwannomas and neurofbromas) of the lower cranial nerves.
•Carotid body tumors below the foramen lacerum.
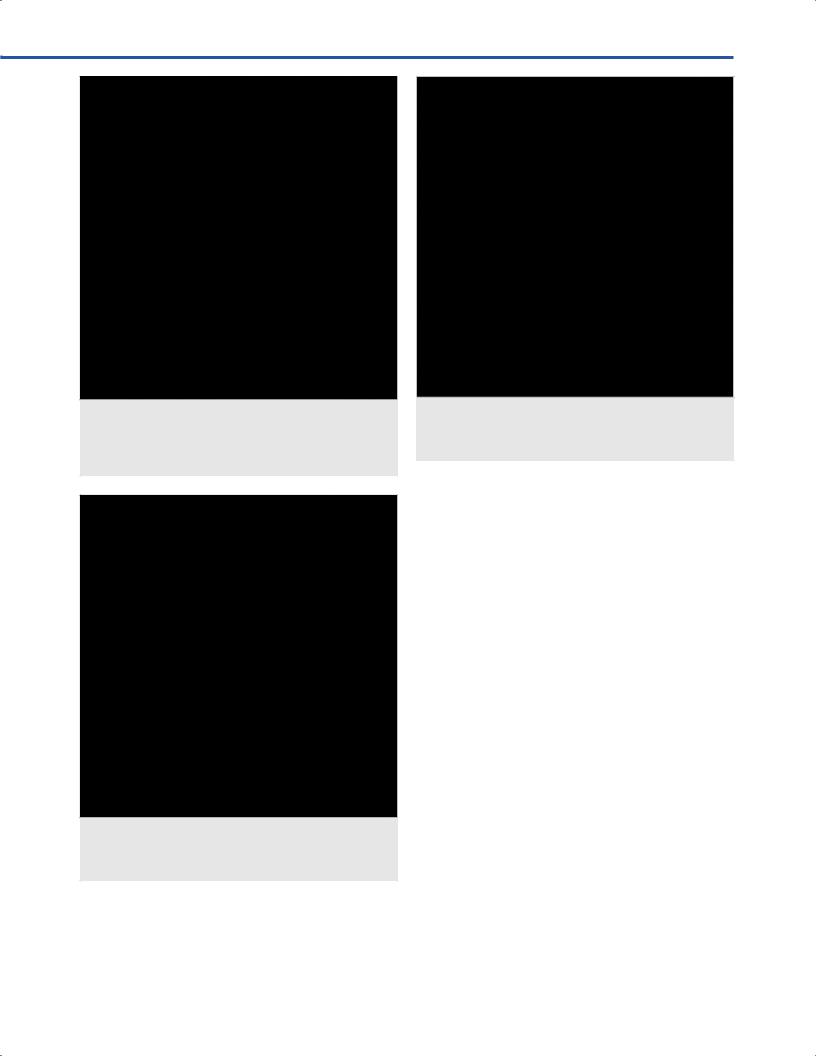
42.3 Patient Positioning (Fig. 42.1)
•General position: The body is positioned supine with the head on a horseshoe or cranial fxation pins.
•Head position: For maximum surgeon comfort, the neck should be neutral or slightly fexed. Assuming a two-surgeon team
Fig. 42.1 Head positioning. (A) The head is translated vertically to prevent the instruments from hitting the chest, especially when the head must be plac xed position. (B) The head is rotated approximately 30° to the right along the coronal plane of the body if both surgeons are right-handed. This may be left neutral if one member of the team is left-handed. (C) The head is tilted approximately 30° along the sagittal axis of the body if both surgeons are right-handed to prevent them from having to reach across the torso to operate. This may be left neutral if one member of the team is left-handed.
260

42 Endoscopic Transoral Approach
(typically an otolaryngologist and a neurosurgeon), a three-step process further maximizes ergonomics for the surgeons:
○1. The head is elevated slightly from the body (Fig. 42.1A).
○2. It is tilted slightly toward the left relative to the axis of the body for right-handed teams (Fig. 42.1B).
○3. It is further turned slightly toward the right or left for surgical teams that are completely rightor left-handed, respectively or left neutral for teams of mixed handedness (Fig. 42.1C).
•Anti-decubitus device: Standard pressure point padding for dependent pressure points in the supine position, including the elbow joints, ulnar nerves if wrapping the patient and foregoing the use of arm boards, the sacral prominence, and the heels might be used.
•Unique preparation consideration: The periumbilical and/ or anterolateral thigh should be prepared using the surgeon’s choice of antimicrobial agent and draped so that they are available for fat and/or muscle graft if needed for dural defect repair or carotid artery injury.
42.4 Oropharyngeal Access and
Retraction
•No skin incision is required to access the posterior oropharyngeal mucosa.
•An oral retractor (such as a Dingman or Spetzler Sonntag retractor) is used to keep the mouth open and tongue retracted caudally throughout the case, carefully avoiding injury to the teeth and protecting the endotracheal tube behind the retractor.
•The two anatomic regions relevant to the skull base neurosurgeon via this approach are the craniovertebral junction (may require a midline transpalatal approach) and the
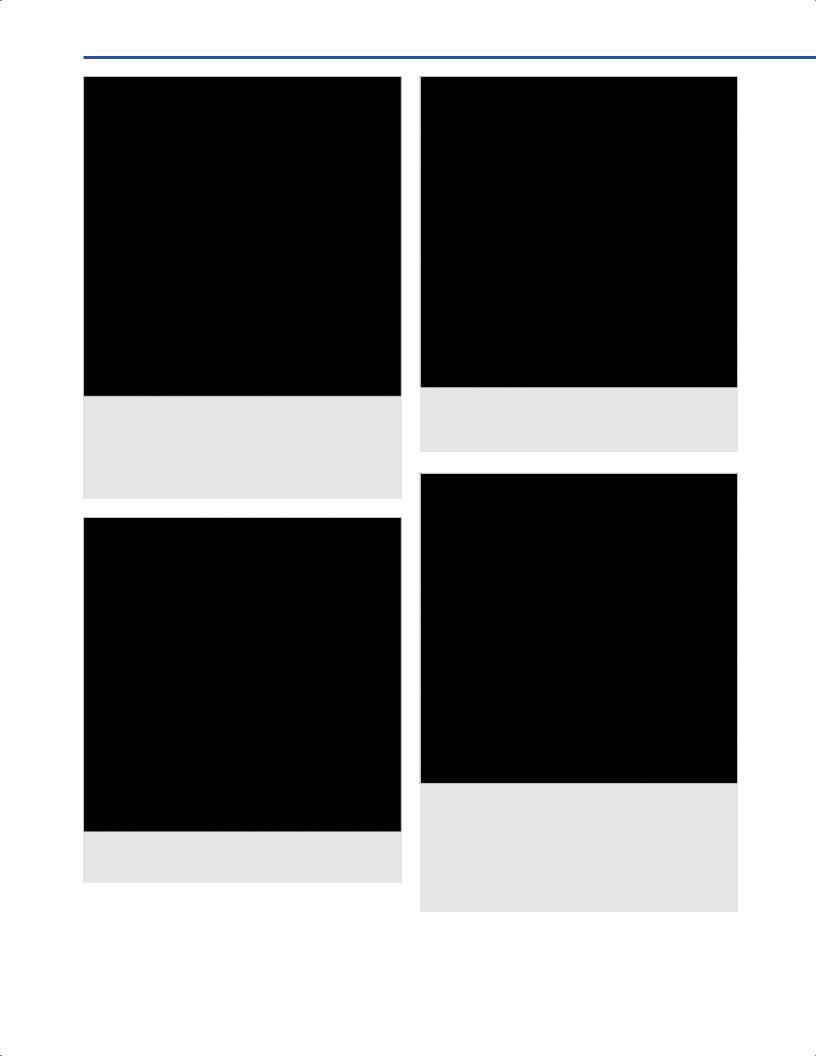
Fig. 42.2 Oral cavity with retractor in place. Red line depicts soft palate incision from the hard palate superiorly and to either side of the uvula inferiorly (left side arbitrarily selected in t Abbreviations: PGA = palatoglossal arch (anterior pillar);
T = tongue; U = uvula.
region of the parapharyngeal internal carotid artery (ICA), foramen lacerum, and jugular foramen (requiring a parapharyngeal retrostyloid approach).
42.4.1 Critical Structures
•Tongue.
•Teeth.
•Soft palate.
•Uvula.
•Palatoglossal arch (anterior pillar).
42.5 Midline Approach to the Craniovertebral Junction
•Once patient is under general anesthesia and the endotracheal tube is secured very laterally in the mouth, a rubber band is passed from the nostrils and it is encountered in the oropharynx. The rubber band is retracted anteriorly bringing the soft palate away from the oropharynx allowing for palate sparing transoral approach.
•In cases of high position of C2, the authors prefer a transnasal approach. However, if there is a need for transoral approach, the soft palate can be transected entirely to permit lateral retraction for oropharyngeal exposure. To accomplish this, an incision is made just lateral to the uvula on either side and curved toward midline above the uvular base. This is extended cranially to the junction with the hard palate (Fig. 42.2). Hooks or sutures are then used to maintain lateral retraction of the split soft palate.
•The oropharyngeal mucosa is incised at the midline (Fig. 42.3) and refected laterally, exposing the horizontally-oriented
Fig. 42.3 Oral cavity with soft palate incised and retracted laterally. Red line depicts midline oropharyngeal mucosal incision, which should be limited caudally to only that which is necessary for access to pathology to minimize risk of dysphagia.
Abbreviations: OM = oropharyngeal mucosa; SP = soft palate; T = tongue; U = uvula.
261
VEndonasal, Transoral, and Transmaxillary Procedures
Fig. 42.4 Oral cavity with the oropharyngeal mucosa incised ted laterally. Red line depicts midline incision on the
superior constrictor muscle, which should be limited caudally to only that which is necessary for access to pathology to minimize risk of dysphagia.
Abbreviations: SCM = superior constrictor muscle; SP = soft palate; T = tongue; U = uvula.
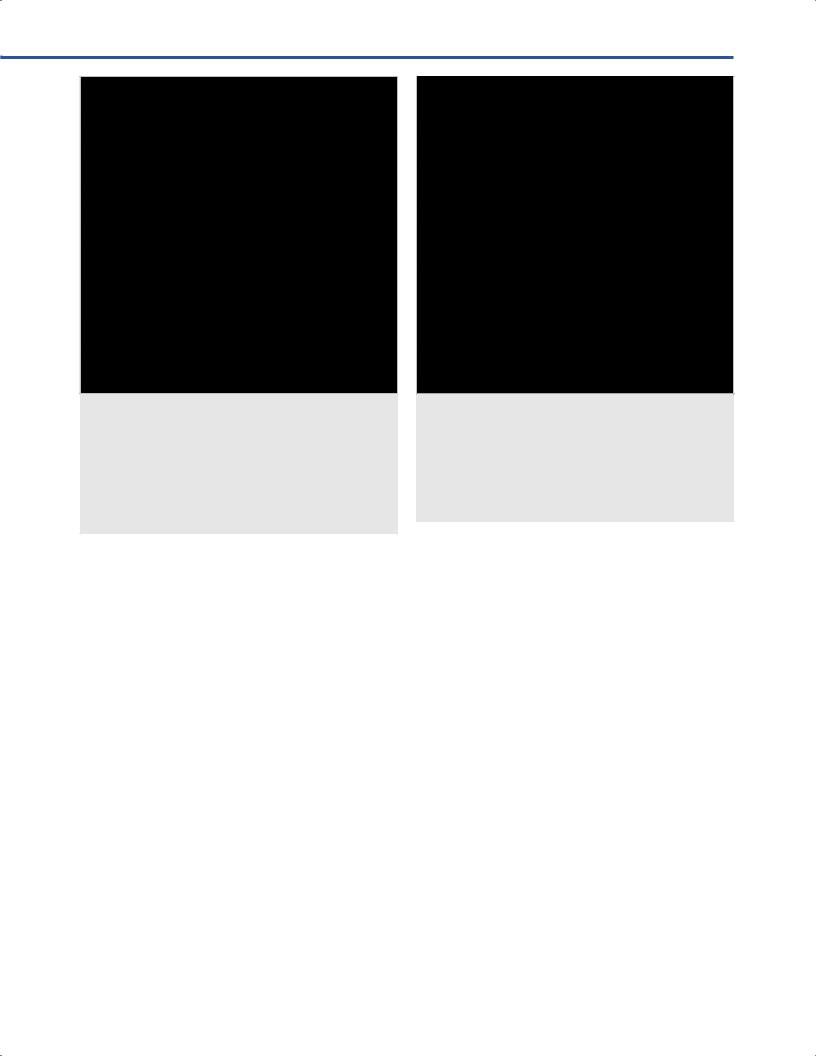
Fig. 42.5 Oral cavity with the superior constrictor muscle incised ted laterally. The prevertebral fascia is seen overlying the
C1 anterior arch and the longus capitis muscles.
Abbreviations: C1 = C1 anterior arch; LCAM = longus capitis muscle; T = tongue.
Fig. 42.6 Resection of prevertebral fascia at the craniovertebral junction, revealing the anterior longitudinal ligament, clivus, C1 anterior arch, C2 body, longus capitis muscles, and longus colli muscles. Abbreviations: ALL = anterior longitudinal ligament; C1 = C1 anterior arch; C2 = C2 body; CV = clivus; LCAM = longus capitis muscle.
fbers of the superior constrictor muscle, which terminates at approximately the level of the superior aspect of the C1 anterior arch and the C2 body (Fig. 42.4). Greater tongue retraction facilitates exposure of the C3 body caudally.
•The superior constrictor muscle is divided in the midline and refected laterally, exposing the fascia overlying the craniovertebral junction and paravertebral musculature, and C1 anterior arch (Fig. 42.5). This prevertebral fascia is resected, exposing the clivus, C1 anterior arch, and C2 body, as well as the anterior longitudinal ligament overlying these structures (Fig. 42.6).
•The anterior longitudinal ligament is removed, and the longus colli are detached from the caudal aspect of the C1 anterior arch (Fig. 42.7); C1 anterior arch is drilled out laterally to the point of the longus capitis bilaterally, facilitating access to the dens and exposing the apical and alar ligaments (Fig. 42.8).
•The dens is drilled in its entirety, exposing the transverse ligament posteriorly (Fig. 42. 9), which must be removed in most of the pathologic situations forming pannus in order to achieve appropriate decompression.
42.5.1 Critical Structures
•Soft palate/uvula.
•Superior constrictor muscle.
•Longus colli.
•Longus capitis.
•C1 anterior arch.
•Body of C2, dens, and apical ligament/alar ligaments.
•Transverse ligament.
•Clivus.
262
42 Endoscopic Transoral Approach
Fig. 42.7 Resection of the anterior longitudinal ligament and detachment of longus colli from C1 bilaterally, fully exposing the C1 anterior arch.
Abbreviations: C1 = C1 anterior arch; C2 = C2 body; CV = clivus; LCAM = longus capitis muscle; LCOM = longus colli muscle.
Fig. 42.8 Dens and alar ligament exposure after removal of the median portion of the C1 anterior arch with a drill. Abbreviations: APL = apical ligament; ARL = alar ligament;
C2 = C2 body; CV = clivus; D = dens; LCAM = longus capitis muscle.
Fig. 42.9 Exposure of transverse ligament and craniocervical junction dura mater after removal of the dens with a drill.
Abbreviations: C1 = C1 anterior arch; C2 = C2 body; CV = clivus; DM = dura mater; LCAM = longus capitis muscle; TL = transverse ligament.
42.6 Parapharyngeal Retrostyloid Approach to the Jugular Foramen Region
•A vertical incision is made just lateral to the palatoglossal arch (anterior pillar) from the hard palate rostrally to the posterolateral foor of the mouth caudally through the
mucosal and submucosal layers until the prestyloid space is opened (Fig. 42.10).
•This is bordered by the oropharynx medially and the medial pterygoid muscle laterally (Fig. 42.11).
•The lingual nerve is seen coursing inferiorly from just lateral to the medial pterygoid toward the tongue (Fig. 42.12).
•After removal of fat from the prestyloid space, the styloglossus muscle is the anterior-most muscle seen attached to the styloid process, and it courses inferomedially toward the base of the tongue.
•Lateral retraction of this reveals the stylopharyngeus muscle, which attaches more posteriorly to the styloid process and courses nearly horizontally toward the superior constrictor muscle (Fig. 42.13).
•Lateral retraction of the stylopharyngeus muscle reveals the glossopharyngeal nerve situated on the anterior aspect of the parapharyngeal segment of the internal carotid artery (Fig. 42.14).
263
VEndonasal, Transoral, and Transmaxillary Procedures
Fig. 42.10 Oral cavity with retractor in place in preparation for a left parapharyngeal retrostyloid approach. Red line depicts mucosal incision made just lateral to the palatoglossal arch
(anterior pillar) from the hard palate rostrally to the posterolaterhe mouth caudally.
Abbreviations: PGA = palatoglossal arch; SP = soft palate; T = tongue; U = uvula.
Fig. 42.11 Prestyolid space bordered by the oropharynx medially and the medial pterygoid muscle laterally.
Abbreviations: MPM = medial pterygoid muscle; OP = oropharynx.
Fig. 42.12 The lingual nerve is seen coursing inferiorly from just lateral to the medial pterygoid toward the tongue. Abbreviations: LN = lingual nerve; MPM = medial pterygoid muscle; PGA = palatoglossal arch; SP = soft palate; T = tongue.
Fig. 42.13 The styloglossus muscle is the anterior-most muscle seen attached to the styloid process, and it courses inferomedially toward the base of the tongue. Lateral retraction of this reveals the stylopharyngeus muscle, which attaches more posteriorly to the styloid process and courses nearly horizontally toward the superior constrictor muscle medially.
Abbreviations: ICA = internal carotid artery; MPM = medial pterygoid muscle; SCM = superior constrictor muscle;
SGM = styloglossus muscle; SPM = stylopharyngeus muscle.
264
42 Endoscopic Transoral Approach
Fig. 42.14 The glossopharyngeal nerve situated on the anterior aspect of the parapharyngeal segment of the internal carotid artery, as seen with lateral retraction of the stylopharyngeus muscle. The vagus nerve is found in between the parapharyngeal segment of the internal carotid artery and the internal jugular vein, with the spinal accessory nerve located just lateral to this. Abbreviations: ICA = internal carotid artery; IJV = internal jugular vein; IX = ninth cranial nerve (glossopharyngeal);
SPM = stylopharyngeus muscle; X = tenth cranial nerve (vagus); XI = eleventh cranial nerve (spinal accessory).
•Reduction or resection of the styloid process and inferior retraction of the styloglossus and stylopharyngeus muscles exposes the parapharyngeal segment of the internal carotid artery to the foramen lacerum and the jugular foramen contents from anteriorly, including the internal jugular vein, glossopharyngeal nerve, vagus nerve, spinal accessory nerve, and hypoglossal nerve (Fig. 42.15).
42.6.1 Critical Structures
•Palatoglossal arch (anterior pillar).
•Lingual nerve.
•Styloid process.
•Internal carotid artery.
•Jugular vein.
•Cranial nerves: ninth, tenth, eleventh, twelfth.
42.7 Pearls
•It is usually possible to address midline anterior pathology in the craniovertebral junction region via an endonasal
Fig. 42.15 Lateral retraction of both the styloglossus and stylopharyngeus muscles and reduction of the styloid process reveals all cranial nerves and major blood vessels in the posterior aspect of the parapharyngeal space.
Abbreviations: ICA = internal carotid artery; IX = ninth cranial nerve (glossopharyngeal); IJV = internal jugular vein;
JF = jugular foramen; LF = lacerum foramen; SP = styloid process; X = tenth cranial nerve (vagus); XI = eleventh cranial nerve (spinal accessory); XII = twelfth cranial nerve (hypoglossal nerve).
approach, lowering the risk of dysphagia, dysphonia, and infection.
•We therefore advocate reserving the use of the transoral approach for cases in which craniovertebral junction pathology extends too caudal to be fully addressed via an endonasal approach.
References
1.Dallan I, Seccia V, Muscatello L, et al. Transoral endoscopic anatomy of the parapharyngeal space: a step-by-step logical approach with surgical considerations. Head Neck 2011;33(4):557–561.
2.Seker A, Inoue K, Osawa S, Akakin A, Kilic T, Rhoton AL Jr. Comparison of endoscopic transnasal and transoral approaches to the craniovertebral junction. World Neurosurg 2010; 74(6):583–602.
265