

- •Operative Cranial Neurosurgical Anatomy
- •Contents
- •Foreword
- •Preface
- •Contributors
- •1 Training Models in Neurosurgery
- •2 Assessment of Surgical Exposure
- •3 Anatomical Landmarks and Cranial Anthropometry
- •4 Presurgical Planning By Images
- •5 Patient Positioning
- •6 Fundamentals of Cranial Neurosurgery
- •7 Skin Incisions, Head and Neck Soft-Tissue Dissection
- •8 Techniques of Temporal Muscle Dissection
- •9 Intraoperative Imaging
- •10 Precaruncular Approach to the Medial Orbit and Central Skull Base
- •11 Supraorbital Approach
- •12 Trans-Ciliar Approach
- •13 Lateral Orbitotomy
- •14 Frontal and Bifrontal Approach
- •15 Frontotemporal and Pterional Approach
- •16 Mini-Pterional Approach
- •17 Combined Orbito-Zygomatic Approaches
- •18 Midline Interhemispheric Approach
- •19 Temporal Approach and Variants
- •20 Intradural Subtemporal Approach
- •21 Extradural Subtemporal Transzygomatic Approach
- •22 Occipital Approach
- •23 Supracerebellar Infratentorial Approach
- •24 Endoscopic Approach to Pineal Region
- •25 Midline Suboccipital Approach
- •26 Retrosigmoid Approach
- •27 Endoscopic Retrosigmoid Approach
- •29 Trans-Frontal-Sinus Subcranial Approach
- •30 Transbasal and Extended Subfrontal Bilateral Approach
- •32 Surgical Anatomy of the Petrous Bone
- •33 Anterior Petrosectomy
- •34 Presigmoid Retrolabyrinthine Approach
- •36 Nasal Surgical Anatomy
- •37 Microscopic Endonasal and Sublabial Approach
- •38 Endoscopic Endonasal Transphenoidal Approach
- •39 Expanded Endoscopic Endonasal Approach
- •41 Endoscopic Endonasal Odontoidectomy
- •42 Endoscopic Transoral Approach
- •43 Transmaxillary Approaches
- •44 Transmaxillary Transpterygoid Approach
- •45 Endoscopic Endonasal Transclival Approach with Transcondylar Extension
- •46 Endoscopic Endonasal Transmaxillary Approach to the Vidian Canal and Meckel’s Cave
- •48 High Flow Bypass (Common Carotid Artery – Middle Cerebral Artery)
- •50 Anthropometry for Ventricular Puncture
- •51 Ventricular-Peritoneal Shunt
- •52 Endoscopic Septostomy
- •Index

44 Transmaxillary Transpterygoid Approach
Nicola Boari, Federico Biglioli, Filippo Gagliardi, and Pietro Mortini
44.1 Introduction
The transmaxillary transpterygoid approach is a variant of the standard Le-Fort I transmaxillary approach, suitable for midline extradural tumors, extending from the sella turcica to the anterior rim of the foramen magnum and laterally to the internal carotid artery (ICA), invading the pterygopalatine fossa, the medial infratemporal fossa and the medial parapharyngeal space.
44.2 Indications
•Clival chordomas and chondrosarcomas.
•Other non-chordomatous lesions of the clivus.
•Esthesioneuroblastoma.
•Malignancy of the anterior skull base-sinonasal tumors.
44.3 Anesthesia And Patient
Intubation
•Downward retraction of the maxilla can be improved by using tracheostomy or submental orotracheal intubation according to Hernandez-Altamir (see Chapter 43).
•Subsequent enhanced exposure of the lower clivus is obtained.
44.5.1 Critical Structures
•Superfcial temporal artery.
•Facial nerve.
44.6 Soft Tissues Dissection
(See Chapter 43)
•Mucosal level
○Gingival mucosa is detached till the maxillary-malar refection on both sides and the foor of the nasal cavity are identifed.
•Bone exposure
○The bony exposure is continued to the level of the last molar.
○Subperiosteal dissection is carried out to expose the anterior maxilla and the piriform aperture, as far as the inferior rim of the infraorbital foramen is exposed.
○The infraorbital nerve is identifed at the exit from its canal. The cartilaginous septum is detached from the nasal spine and vomer.
44.6.1 Critical Structures
• Infraorbital nerves.
44.4 Patient Positioning
•Position: The patient is positioned supine with the head fxed to a horseshoe head holder.
•Body: The body is placed in neutral position with the trunk elevated of 30° to increase venous backfow and the legs elevated at the level of the heart.
•Head: The head is tilted back 20°and toward the left shoulder 25°. The surgeon is placed on the right side of the patient.
•Anti-decubitus device: Rolls are placed under the knees.
•The zygoma must be the highest point in the surgical feld.
44.5 Mucosal Incision
(See Chapter 43)
A mucoperiosteal incision is performed between the frst molars, 1 cm above the gingival refection along the upper alveolar margin, leaving a cuf of mucosa on the gingival side.
44.7 Maxillar Osteotomy
(See Chapter 43)
•A Le Fort I osteotomy is performed 8-10 mm above the roots of the teeth with an oscillating saw.
•The nasal septum is then divided from the maxilla on the midline, and a curved chisel is used to divide the ptery- goid-maxillary junctions.
•The hard palate is down-fractured and mobilized into the oral cavity.
•A self-retaining retractor is positioned between the maxilla and the hard palate.
44.7.1 Critical Structures
• Palatine nerves and arteries.
270
44 Transmaxillary Transpterygoid Approach
44.8 Clival Exposure
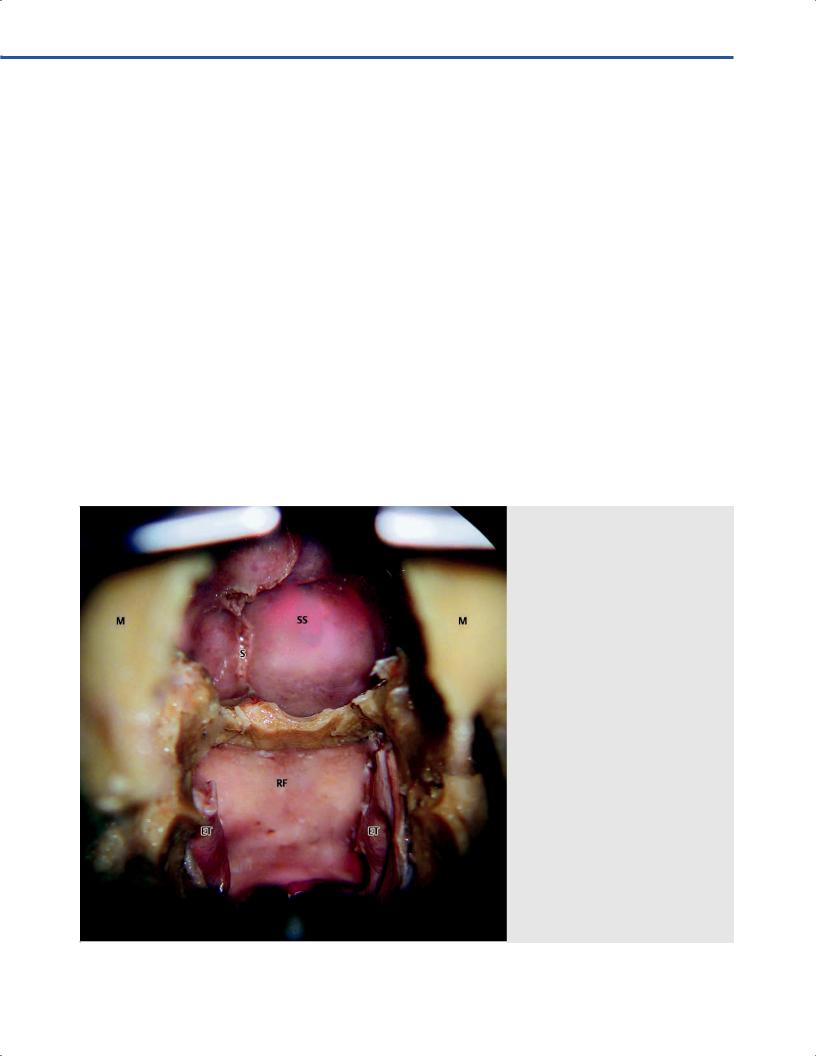
•The sphenoid sinus is opened and the posterior sinus wall is drilled out, exposing the sellar foor, the carotid and optic prominences (Fig. 44.1).
•A longitudinal incision is performed on the midline along the rhinopharynx mucosa and the parapharyngeal muscles, together with the mucosa, are dissected in a subperiosteal fashion from the underlying clival bony surface.
•Clival resection is completed by drilling the middle and lower clival bone until the foramen magnum.
44.8.1 Critical Structures
•Internal carotid arteries (ICA): C3, C4 and C5 segments.
•Optic nerves and chiasm.
44.9 Paraclival Exposure (Figs. 44.2–44.5)
•Lateral exposure is completed by removing the inferior and middle turbinates and by resecting the posterior wall of the maxillary sinus.
•Pterygopalatine fossa is opened, gaining access to the third segment of the maxillary artery, which is mobilized laterally by dividing the sphenopalatine artery.
•The greater palatine artery is preserved. The vidian nerve is completely skeletonized to the lacerous segment of the internal carotid artery.
•The pterygoid plates on both sides are removed, widening the paraclival dura exposure to the infratemporal segment of the mandibular branch of the trigeminal nerve (V3).
•The Eustachian tube can be divided opening the surgical access to the parapharyngeal space.
44.9.1 Critical Structures
•ICAs: C2, C3 and C4 segments.
•Maxillary arteries.
•Greater palatine nerves and arteries.
•Pterygopalatine ganglions.
•Maxillary (V2), and mandibular branch (V3) of the trigeminal nerve.
•Eustachian tubes.
•Twelfth cranial nerves (hypoglossal nerve).
44.10 Dural Opening (Fig. 44.6)
•The dura is divided longitudinally on the midline.
•Bleeding from the basilar plexus must be managed by compression and by using hemostatic agents.
Fig. 44.1 The clivus is exposed from the sella turcica to the anterior border of the foramen magnum.
Abbreviations: ET = Eustachian tube;
M = maxilla; RF = rhinopharynx; S = septum; SS = sphenoid sinus.
271
VEndonasal, Transoral, and Transmaxillary Procedures
Fig. 44.2 The paraclival area is exposed by removing the posterior wall of the maxillary sinus.
Abbreviations: GPA = greater palatine artery; M = maxilla; MPP = middle pterygoid process; SPA = sphenopalatine artery.
Fig. 44.3 Vascular structures of the pterygopalatine fossa. Abbreviations: GPA = greater palatine artery; IOA = infraorbital artery; LPM = lateral pterygoid muscle; LPP = lateral pterygoid process; M = maxilla; MA = maxillary artery; PSAR = posterior superior alveolar artery; SPA = sphenopalatine artery.
Fig. 44.4 Exposure of the lateral pterygoid process. Abbreviations: ET = Eustachian tube; GPN = greater palatine nerve; ION = infraorbital nerve; OF = orbit ; LPM = lateral pterygoid muscle; LPP = lateral pterygoid process; M = maxilla; VN = Vidian nerve.
Fig. 44.5 The operativ ld after removal of medial and lateral pterygoid plates.
Abbreviations: CD = clival dura; CS = cavernous sinus; GPN = greater palatine nerve; ICA = internal carotid artery; ION = infraorbital nerve; OF = orbit ; LPM = lateral pterygoid muscle;
M = maxilla; PPG = pterygopalatine ganglion; SD = sellar dura; V2 = maxillary nerve; VN = Vidian nerve; ZN = zygomatic nerve.
272
44 Transmaxillary Transpterygoid Approach
Fig. 44.6 Exposure of clival dura.
Abbreviations: CD = clival dura; ET = Eustachian tube; ICA = internal carotid artery; M = maxilla; HP = hard palate; SD = sellar dura.
44.10.1 Critical Structures
•Basilar artery.
•Brainstem.
•Sixth cranial nerves (abducens nerve).
44.11 Intradural Exposure (Fig. 44.7)
•Parenchymal structures: Pituitary gland, ventral aspect of the brainstem.
•Arachnoidal layer: Chiasmatic cistern, inter-peduncular cistern, pre-pontine cistern.
•Cranial nerves: Optic nerves, sixth and lower cranial nerves.
•Arteries: Vertebral arteries, basilar artery, posterior-inferior cerebellar artery, anterior inferior cerebellar artery, superior cerebellar artery, posterior cerebral artery.
44.12 Dural Reconstruction
•Free mucosal graft and fascia lata fap are indicated for small dural defects.
•Pedicled fascial, pericranial, galeopericranial, or mucosal faps are necessary for the repair of larger defects.
•Nasal packing is performed.
•A lumbar drainage is positioned and left in place for 5 days is recommended.
44.13 Pearls
•Maxillary pre-plating before Le Fort I osteotomy minimizes the risk of dental malocclusion.
Fig. 44.7 Intradural exposure.
Abbreviations: BA = basilar artery; HP = hard palate; ICA = internal carotid artery; M = maxilla; P = pons; PICA = posterior inferior cerebellar artery; PY = pyramid; SD = sellar dura; VA = vertebral artery.
•Bilateral closure of the greater palatine arteries can increase the risk of aseptic necrosis of the maxilla.
•Identifcation of the optic and carotid prominences in the parasellar area is crucial to avoid neurovascular injuries.
•Onodi cell (spheno-ethmoidal air cell) must be identifed when present.
•An endoscopic-assisted procedure is suggested in order to improve the visualization of paraclival anatomical structures.
•Sacrifce of the cartilaginous part of the Eustachian tube can lead to unilateral deafness; in this case, a tympanic drain should be placed to preserve adequate ventilation of the middle ear.
•Meticulous multilayer dural reconstruction is crucial in order to avoid cerebrospinal fuid (CSF) leak through the nose.
•The same clival and paraclival exposure can be obtained through an extended endoscopic endonasal approach.
References
1.Biglioli F, Mortini P, Goisis M, Bardazzi A, Boari N. Submental orotracheal intubation: an alternative to tracheostomy in transfacial cranial base surgery. Skull Base 2003;13(4):189–195.
2.Boari N, Roberti F, Biglioli F, Caputy AJ, Mortini P. Quantifcation of clival and paraclival exposure in the Le Fort I transmaxillary transpterygoid approach: a microanatomical study. J Neurosurg 2010;113(5):1011–1018.
3.Gagliardi F, Boari N, Mortini P. Reconstruction techniques in skull base surgery. Review J Craniofac Surg 2011;22(3):1015–1020.
4.Roberti F, Boari N, Mortini P, Caputy AJ. The pterygopalatine fossa: an anatomic report. J Craniofac Surg 2007; 18(3):586–590.
273