

- •Operative Cranial Neurosurgical Anatomy
- •Contents
- •Foreword
- •Preface
- •Contributors
- •1 Training Models in Neurosurgery
- •2 Assessment of Surgical Exposure
- •3 Anatomical Landmarks and Cranial Anthropometry
- •4 Presurgical Planning By Images
- •5 Patient Positioning
- •6 Fundamentals of Cranial Neurosurgery
- •7 Skin Incisions, Head and Neck Soft-Tissue Dissection
- •8 Techniques of Temporal Muscle Dissection
- •9 Intraoperative Imaging
- •10 Precaruncular Approach to the Medial Orbit and Central Skull Base
- •11 Supraorbital Approach
- •12 Trans-Ciliar Approach
- •13 Lateral Orbitotomy
- •14 Frontal and Bifrontal Approach
- •15 Frontotemporal and Pterional Approach
- •16 Mini-Pterional Approach
- •17 Combined Orbito-Zygomatic Approaches
- •18 Midline Interhemispheric Approach
- •19 Temporal Approach and Variants
- •20 Intradural Subtemporal Approach
- •21 Extradural Subtemporal Transzygomatic Approach
- •22 Occipital Approach
- •23 Supracerebellar Infratentorial Approach
- •24 Endoscopic Approach to Pineal Region
- •25 Midline Suboccipital Approach
- •26 Retrosigmoid Approach
- •27 Endoscopic Retrosigmoid Approach
- •29 Trans-Frontal-Sinus Subcranial Approach
- •30 Transbasal and Extended Subfrontal Bilateral Approach
- •32 Surgical Anatomy of the Petrous Bone
- •33 Anterior Petrosectomy
- •34 Presigmoid Retrolabyrinthine Approach
- •36 Nasal Surgical Anatomy
- •37 Microscopic Endonasal and Sublabial Approach
- •38 Endoscopic Endonasal Transphenoidal Approach
- •39 Expanded Endoscopic Endonasal Approach
- •41 Endoscopic Endonasal Odontoidectomy
- •42 Endoscopic Transoral Approach
- •43 Transmaxillary Approaches
- •44 Transmaxillary Transpterygoid Approach
- •45 Endoscopic Endonasal Transclival Approach with Transcondylar Extension
- •46 Endoscopic Endonasal Transmaxillary Approach to the Vidian Canal and Meckel’s Cave
- •48 High Flow Bypass (Common Carotid Artery – Middle Cerebral Artery)
- •50 Anthropometry for Ventricular Puncture
- •51 Ventricular-Peritoneal Shunt
- •52 Endoscopic Septostomy
- •Index
38 Endoscopic Endonasal Transphenoidal Approach
Kevin Swong, Asterios Tsimpas, Chirag R. Patel, and Anand V. Germanwala
38.1 Patient Positioning
•Position: The patient is positioned supine with slight rotation towards operating team.
•Head: The head is slightly extended and above the heart with
Mayfeld pins for intra-arachnoidal lesions.
•The tip of patient’s nose should be the highest point in the surgical feld.
•Abdomen is usually prepped for potential fat graft.
38.2 Preoperative Settings
•Neurophysiological monitoring (electroencephalogram and somatosensory evoked potentials) is often utilized.
•Image guidance navigation with stereotactic CT and MRI is often used.
•Nasal cavity decongestion with topical vasoconstricting agents (1:1000 Epinephrine, oxymetazoline, or
4% cocaine).
38.3 Skin Incision
•Not applicable.
•Close collaboration with an ENT team is favored.
○Option 1: Single nare technique with or without turbinate resection.
○Option 2 (favored): Bilateral nare technique with or without turbinate resection, which provides a wider viewing angle and area of exposure, more room for skull base instruments, and better haptic feedback.
38.4 Soft Tissue Dissection, Nasal
Phase (Figs. 38.1–38.4)
•Depending on the preference of the ENT surgeon, local anesthetic may be injected before or after the patient is draped.
•Additionally, cotton pledgets saturated in a topical vasoconstricting agent placed between the middle turbinate and the nasal septum may aid in decongestion.
•A 0° rigid endoscope is introduced into the nasal cavities; the inferior turbinates and the nasal septum are the frst identifable landmarks.
•The middle turbinates are then moved laterally to allow for increased exposure. If necessary, the middle turbinate can be resected for additional space.
•The sphenoid ostium is identifed adjacent to the septum near the inferior edge of the superior turbinate. This is approximately 2 cm above the arch of the choana.
38.4.1 Critical Structures
•Inferior, middle, and superior turbinates.
•Choana, sphenoid ostium.
38.5 Osteotomy, Sphenoid Phase (Fig. 38.4–38.9)
•Care is taken during approach to preserve sphenopalatine arteries in anticipation of possible skull base dural reconstruction with a pedicled vascularized nasoseptal fap.
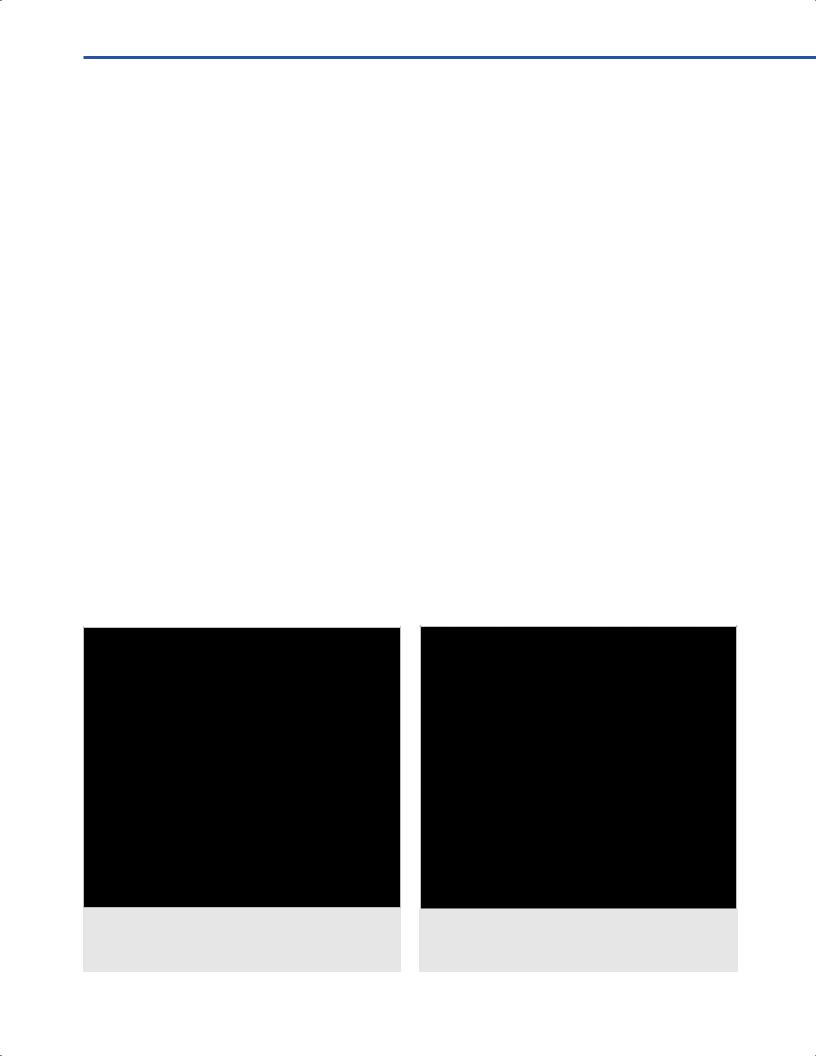
Fig. 38.1 Endoscopic endonasal photo depicting sino-nasal landmarks in the right nasal cavity.
Abbreviations: IT = inferior turbinate; MT = middle turbinate; NS = nasal septum.
Fig. 38.2 Endoscopic endonasal photo depicting sino-nasal landmarks deeper in the right nasal cavity. Ident tion of the superior turbinate. Abbreviations: IT = inferior turbinate; MT = middle turbinate;
NS = nasal septum; ST = superior turbinate.
236
38 Endoscopic Endonasal Transphenoidal Approach
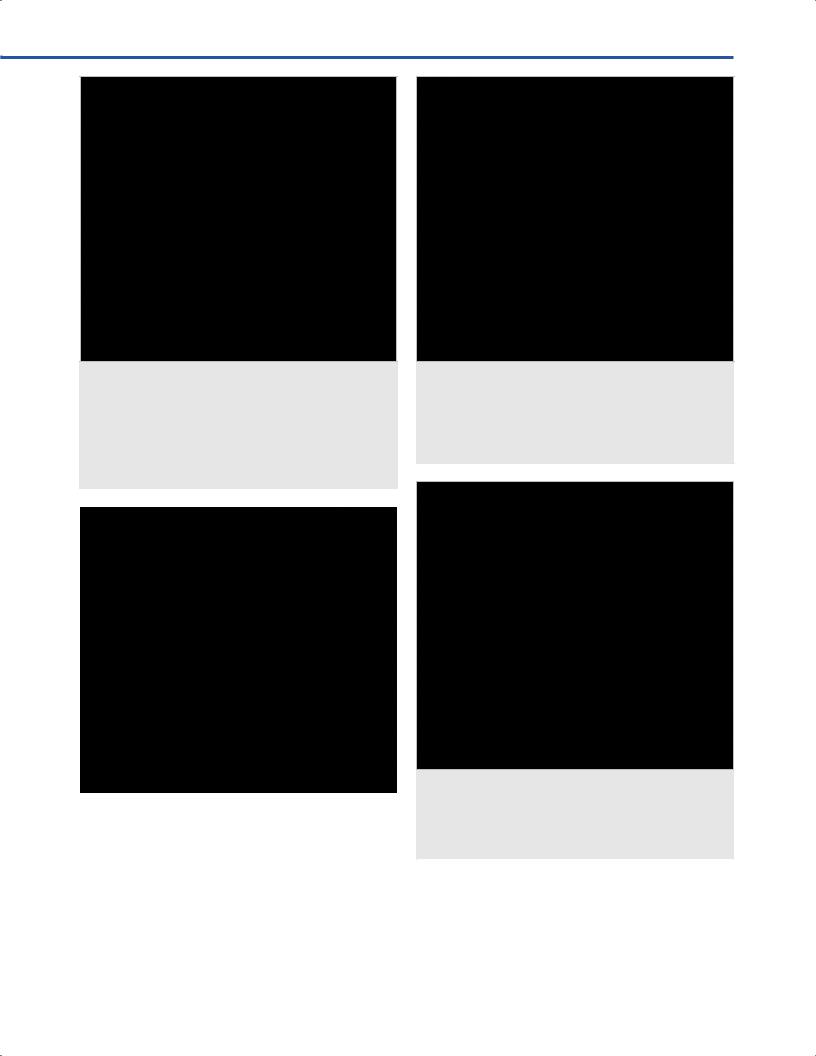
Fig. 38.3 Endoscopic endonasal intraoperative photo depicting location of the right sphenoid ostium. Note that the sphenoid ostium in this specimen is higher than we would typically expect (i.e. closer to the inferior edge of the superior turbinate). Extra caution should be taken during widening of the sphenoid ostium in this situation as it is located much closer to the skull base
(i.e. planum sphenoidale).
Abbreviations: MT = middle turbinate; NS = nasal septum; SO = sphenoid ostium; ST = superior turbinate.
|
|
|
Fig. 38.4 |
View of right nasal cavity after removal of middle |
|
turbinate. Note the location of the vascular pedicle for the |
|
|
nasosept |
amage to this mucosa should be avoided to |
|
preserve the viability of t |
|
|
Abbreviations: CA = choanal arch; MTr = middle turbinate |
|
|
resected; NS = nasal septum; NSFP = nasosept |
le; |
|
SO = sphenoid ostium; ST = superior turbinate. |
|
|
|
|
|
•This neurovascular pedicle runs horizontally across the sphenoid face and extends from the arch of the choana to the level of the natural sphenoid ostium.
Fig. 38.5 The right sphenoid ostium has been partially widened. A more limited opening has been employed initially in this specimen due to the high position of the natural ostium (thus its proximity to the skull base superiorly) and the need to protect the nasosept pedicle inferiorly. The posterior septectomy has also been outlined. Abbreviations: NS = nasal septum; PS = posterior septectomy;
SOw = widened sphenoid ostium; STt = trimmed superior turbinate.
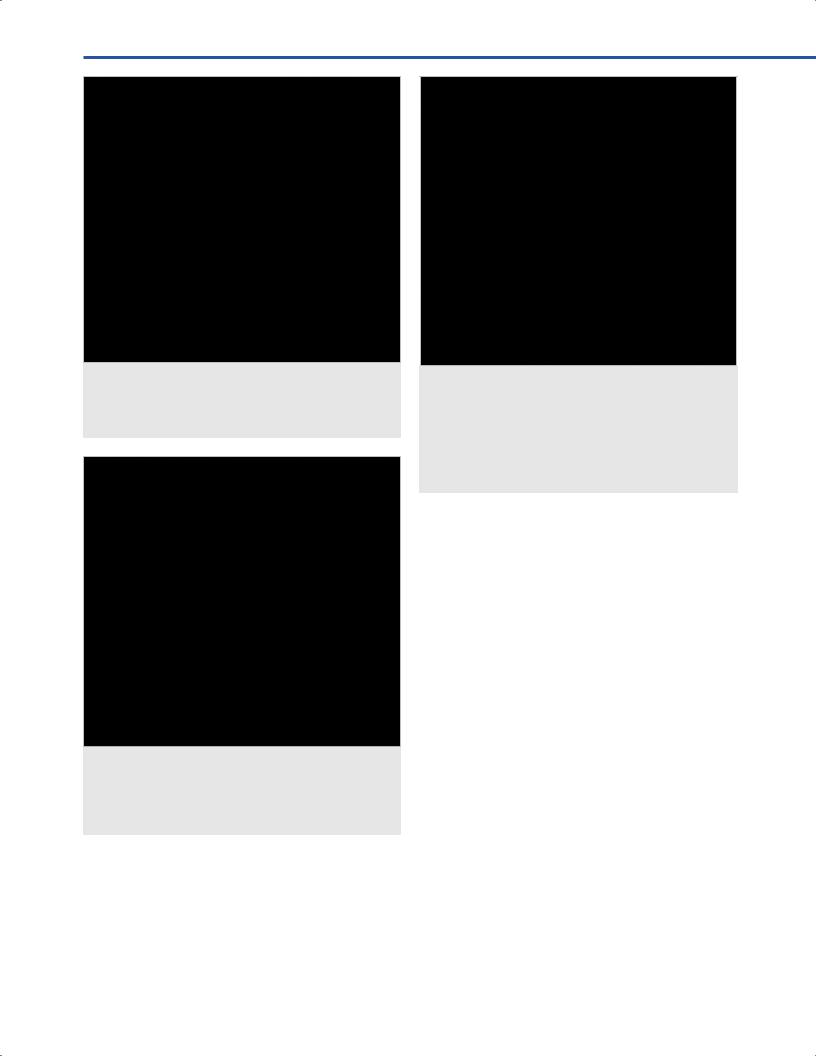
Fig. 38.6 The posterior septectomy has been completed. Instruments passed through the left nasal cavity can now be seen from the right. Also note the sphenoidotomy has been further widened as better visualization has been obtained. Abbreviations: PS = posterior septectomy; RSO =right sphenoid ostium; S = suction tube in the contralateral nasal fossa.
•The sphenoid ostium is widened frst laterally then superiorly on both sides. The superior turbinate can be trimmed as needed to improve visualization and access.
•A small posterior septectomy is then performed to allow binarial access.
237
VEndonasal, Transoral, and Transmaxillary Procedures
Fig. 38.7 The vascular pedicle is being carefully elevat he face of the sphenoid to allow widening of the sphenoidotomy inferiorly while protecting t le.
Abbreviations: LS = left sphenoid; NSFP = nasosept peduncle; R = rostrum; RS = right sphenoid.
Fig. 38.9 The remainder of the face of the sphenoid and the sphenoid rostrum have been removed. Note the left sphenoid in this specimen is small and under-pneumatized. The clival recess, sella, and right carotid are clearly visible. The optic-carotid recess is not well formed.
Abbreviations: CR = clival recess; LS = left sphenoid; PS = planum sphenoidalis; RICA = right internal carotid artery; ROCR = right optic-carotid recess; RS = right sphenoid; S = sella; T = tuberculum sellae.
The pedicle is elevated inferiorly of the face of the sphenoid to expose the underlying bone. The sphenoidotomy can then be safely widened inferiorly without sacrifcing the pedicle.
•The bony nasal septum is detached from sphenoid rostrum, and the rostrum is removed with rongeurs or a drill.
The anterior wall of the sphenoid sinus is further widened as needed.
•Sphenoid septations are removed, allowing visualization of the bony prominences of the internal carotid artery (ICA), planum, and optic-carotid recess (OCR).
Fig. 38.8 In this view, a right nasosept s been elevated and tucked into the nasopharynx. The bony nasal septum has been disarticulated from the rostrum, giving us a clear view of the “keel.”
Abbreviations: LS = left sphenoid; NS = nasal septum; NSF = nasosept ostrum; RS = right sphenoid.
•If use of a nasoseptal fap is anticipated for reconstruction, it should be elevated at this point to protect the neurovascular pedicle and the fap mucosa. The fap can be stored in the nasopharynx for safekeeping until needed. Should the fap not be needed, it can be sutured back to the septum at the end of the procedure.
•If use of a nasoseptal fap is not anticipated, the pedicle should still be protected to preserve reconstructive options.
38.5.1 Critical Structures
•OCR: Endonasally visualized pneumatization of optic strut.
•ICA: Cavernous segment.
38.5.2 Pitfalls
•Spheno-ethmoidal air cell (Onodi Cell): posterior ethmoid air cell that lies superior to the sphenoid sinus that may house the ICA or the optic nerve (ON).
38.6 Osteotomy, Sellar
Phase (Figs. 38.10–38.13)
•The endoscope may be attached to a holder if desired; however, most surgeons use an assistant to hold the endoscope to allow for continued dynamic manipulation of the feld of view.
238
38 Endoscopic Endonasal Transphenoidal Approach
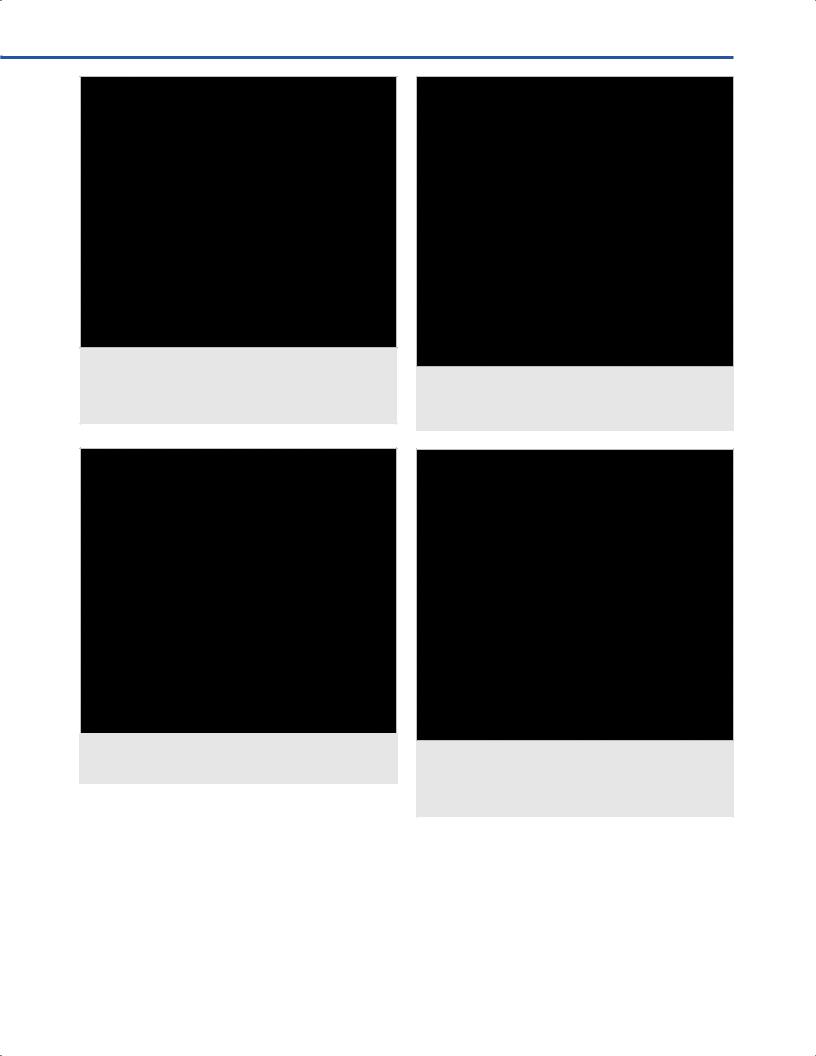
Fig. 38.10 A two-handed binarial technique can now be employed. Here a suction is placed through the right nostril and a drill is passed through the left.
Abbreviations: LS = left sphenoid; RICA = right internal carotid artery; S = sella.
Fig. 38.11 Endoscopic endonasal photo depicting thinned sellar ter drilling.
Abbreviations: RICA = right internal carotid artery; S = sella.
•The sellar foor is opened using a combination of a highspeed drill and Kerrison rongeurs.
○Bony work may be less if there is erosion of the bony foor.
○Footplate of the rongeur should be parallel with the carotid artery.
•Ultrasonic doppler probe and image guidance may be utilized to identify the carotid arteries.
Fig. 38.12 The bone of the sella is thinned and a small bony defect is created to allow further bone removal with Kerrison rongeurs. Abbreviations: RICA = right internal carotid artery; S = sella;
SD = sellar dura.
Fig. 38.13 The bone has been removed from the sella, tuberculum, and both carotids.
Abbreviations: CR = clival recess; CS = chiasmatic sulcus; LICA = left internal carotid artery; PS = planum sphenoidalis; RICA = right internal carotid artery; SD = sellar dura.
38.7 Dural Opening (Figs. 38.14–38.16)
•Once the bone has been cleared, the dura is opened in a cruciate fashion.
239
VEndonasal, Transoral, and Transmaxillary Procedures
Fig. 38.14 Endoscopic endonasal photo depicting dural opening with a sickle knife blade.
Abbreviations: CR = clival recess; CS = chiasmatic sulcus; LICA = left internal carotid artery; RICA = right internal carotid artery; SD = sellar dura.
Fig. 38.15 The dura can be dissected away from the pituitary capsule.
Abbreviations: CR = clival recess; CS = chiasmatic sulcus; LICA = left internal carotid artery; RICA = right internal carotid artery.
•Venous bleeding is controlled with gentle pressure, warm irrigation, and hemostatic agents such as Floseal or Gelfoam soaked in thrombin.
38.8 Intradural Exposure (See
Anatomy in Chapters 36 And 39)
•Identify tumor capsule if present (and frm) to allow for enbloc resection.
Fig. 38.16 Completed dural opening with underlying gland exposed.
Abbreviations: CR = clival recess; LICA = left internal carotid artery; OC = optic chiasm; P = pituitary gland; RICA = right internal carotid artery.
○If unable to identify plane or tumor is soft, intra-tumoral debulking will be necessary.
○Prefer two suction technique or ultrasonic aspiration for resection under visualization.
○However, at times, curettes can be used to assist in resection more superfcially.
•Inferior and lateral aspects of tumor should be approached before the superior aspect to prevent premature downward descent of the diaphragma which may obstruct visualization.
•If there is extension into the medial cavernous sinus, it is helpful to insert the endoscope into the contralateral nostril to improve visualization or consider use of angled endoscopes.
○A Doppler and image guidance is helpful to identify the carotid arteries.
○Venous bleeding can be controlled with a combination of hemostatic agents and cotton pledgets.
○Neurophysiological monitoring of cranial nerves (EMG) may be helpful in this particular case.
•If there is extension into the lateral cavernous sinus, the exposure can be extended by removal of the ethmoidal bullae and medial pterygoid process.
○The carotid artery is identifed with a Doppler probe before the dura is opened.
○Neurophysiological monitoring of cranial nerves (EMG) may be helpful in this particular case.
•The area of the resection is directly inspected for any residual tumor.
•An angled scope is helpful for seeing around neurovascular structures.
38.8.1 Critical Structures
•Carotid artery.
•Cavernous sinus.
•Diaphragma sellae.
240
38 Endoscopic Endonasal Transphenoidal Approach
Fig. 38.17 A free mucosal graft was harvested from the previously resected middle turbinate and has been placed over the sellar defect. Note that a rather sizeable graft can be harvested from the middle turbinate. It is important to ensure the periosteal side faces the bone and the mucosal side faces the sinus cavity.
Abbreviations: CR = clival recess; FMG = free mucosal graft.
Fig. 38.18 Use of a nasosept or reconstruct
can be oriented in any position that is favorable as long as the entire perichondrial/periosteal surface is touching denuded bone and the mucosal surface is facing the nasal cavity.
Abbreviations: NSF = nasosept |
sosept |
peduncle. |
|
38.9 Reconstruction (Figs. 38.17, 38.18)
•Depends on type of cerebrospinal fuid (CSF) leak.
○High fow (ventricular) CSF leak.
○Low fow (cisternal) CSF leak.
○Pinhole CSF leak.
○No CSF leak.
•For situations with a pinhole CSF leak or no leak, it is our practice to line the dural defect with an avascular collagen graft and/or a free mucosal graft, and then line the edges with Surgicel.
•A free mucosal graft can be harvested from a previously resected middle turbinate or from the nasal foor.
•For low and high fow leak situations, a vascularized pedicled mucosal fap is favored after repair with an avascular graft.
•It is very rare to utilize a lumbar drain; would consider this, in addition to vascularized reconstruction, in patients with elevated CSF pressure and a high fow leak.
38.10 Postoperative Care
•It is important the close collaboration with ENT for continued follow up.
•Postoperative imaging should be obtained.
•Patients should be monitored for symptoms and signs of CSF leak, infection, and endocrinopathies.
References
1.Cavallo LM, Cappabianca P, Galzio R, Iaconetta G, de Divitiis E, Tschabitscher M. Endoscopic transnasal approach to the cavernous sinus versus transcranial route: anatomic study.Neurosurgery2005;56(2,Suppl):379–389,discussion 379–389.
2.Dallapiazza RF, Jane JA Jr. Outcomes of endoscopic transsphenoidal pituitary surgery. Endocrinol Metab Clin North Am 2015; 44(1):105–115.
3.Elhadi AM, Hardesty DA, Zaidi HA, et al. Evaluation of surgical freedom for microscopic and endoscopic transsphenoidal approaches to the sella. Neurosurgery 2015;11(Suppl 2):69–78, discussion 78–79.
4.Patel MR, Stadler ME, Snyderman CH, et al. How to choose? Endoscopic skull base reconstructive options and limitations. Skull Base 2010;20(6):397–404.
241