

- •Operative Cranial Neurosurgical Anatomy
- •Contents
- •Foreword
- •Preface
- •Contributors
- •1 Training Models in Neurosurgery
- •2 Assessment of Surgical Exposure
- •3 Anatomical Landmarks and Cranial Anthropometry
- •4 Presurgical Planning By Images
- •5 Patient Positioning
- •6 Fundamentals of Cranial Neurosurgery
- •7 Skin Incisions, Head and Neck Soft-Tissue Dissection
- •8 Techniques of Temporal Muscle Dissection
- •9 Intraoperative Imaging
- •10 Precaruncular Approach to the Medial Orbit and Central Skull Base
- •11 Supraorbital Approach
- •12 Trans-Ciliar Approach
- •13 Lateral Orbitotomy
- •14 Frontal and Bifrontal Approach
- •15 Frontotemporal and Pterional Approach
- •16 Mini-Pterional Approach
- •17 Combined Orbito-Zygomatic Approaches
- •18 Midline Interhemispheric Approach
- •19 Temporal Approach and Variants
- •20 Intradural Subtemporal Approach
- •21 Extradural Subtemporal Transzygomatic Approach
- •22 Occipital Approach
- •23 Supracerebellar Infratentorial Approach
- •24 Endoscopic Approach to Pineal Region
- •25 Midline Suboccipital Approach
- •26 Retrosigmoid Approach
- •27 Endoscopic Retrosigmoid Approach
- •29 Trans-Frontal-Sinus Subcranial Approach
- •30 Transbasal and Extended Subfrontal Bilateral Approach
- •32 Surgical Anatomy of the Petrous Bone
- •33 Anterior Petrosectomy
- •34 Presigmoid Retrolabyrinthine Approach
- •36 Nasal Surgical Anatomy
- •37 Microscopic Endonasal and Sublabial Approach
- •38 Endoscopic Endonasal Transphenoidal Approach
- •39 Expanded Endoscopic Endonasal Approach
- •41 Endoscopic Endonasal Odontoidectomy
- •42 Endoscopic Transoral Approach
- •43 Transmaxillary Approaches
- •44 Transmaxillary Transpterygoid Approach
- •45 Endoscopic Endonasal Transclival Approach with Transcondylar Extension
- •46 Endoscopic Endonasal Transmaxillary Approach to the Vidian Canal and Meckel’s Cave
- •48 High Flow Bypass (Common Carotid Artery – Middle Cerebral Artery)
- •50 Anthropometry for Ventricular Puncture
- •51 Ventricular-Peritoneal Shunt
- •52 Endoscopic Septostomy
- •Index

37 Microscopic Endonasal and Sublabial Approach
Michael Buchfelder and Sven-Martin Schlafer
37.1 Introduction
The microscopic endonasal and sublabial approach is a midline skull-base approach, which provides direct access to the sellar and parasellar region with a surgical corridor free from major neurovascular structures.
37.2 Indications
•Intraand suprasellar pituitary adenomas.
•Intraand suprasellar craniopharyngiomas.
•Any other intrasellar lesions.
•Suprasellar lesions depending on magnitude of sella enlargement.
37.3 Patient Positioning (Fig. 37.1)
•Position: Patient is positioned supine with the head on a fat headrest.
•Body: The body is positioned straight and fat.
•Head: The head is positioned straight, extended 15°.
•Cushion is placed under patient’s shoulders.
•The upper lip has to be the highest point in the surgical feld.
Fig. 37.1 Patient positioning.
37.4 Mucosal Incision for Endonasal Approach (Fig. 37.2)
•The right nostril is exposed (if surgeon is right-handed).
•The base of right nostril is retracted with Langenbeck retractor.
•A straight unilateral incision is performed.
○Starting point: Incision starts 4 mm below the surface of right cartilage.
○Course: It runs straight above nasal cartilage, parallel to nostril.
○Ending point: It ends at the superior medial margin of the right nostril.
37.5 Mucosal Incision for Sublabial Approach (Figs. 37.3–37.5)
•The upper lip is retracted with 2 Langenbeck retractors.
•A straight unilateral incision is performed (Fig. 37.3).
○Starting point: Incision starts at the level of medial canines.
○Course: It runs parallel to the plica between gingiva and upper lip (4 mm from plica), crossing the phrenulum.
•The anterior margin of nasal cartilage is exposed (Fig. 37.4).
•The mucosa is dissected on a sub-perichondrial plane.
•The self-retaining speculum is inserted (Fig. 37.5).
37.6 Soft Tissue Dissection for Endonasal Approach
(Figs. 37.6–37.9)
•Mucosa is detached unilaterally from the cartilaginous septum and the submucosal tunnel is created (Fig. 37.6).
•Medial nasal mucosa has to be kept intact by careful stepwise dissection.
•A self-retaining speculum is inserted.
•The junction of cartilaginous and bony nasal septum is exposed and dissected (Fig. 37.7).
•The mucosa is detached bilaterally from the bony nasal septum (Figs. 37.7, 37.8).
•The junction of cartilaginous and bony nasal septum is separated.
•The paraseptal mucosa is detached bilaterally from the bony nasal septum.
•Portions of bony nasal septum are resected (Fig. 37.8).
•The self-retaining speculum is inserted (Fig. 37.9).
228

37 Microscopic Endonasal and Sublabial Approach
Fig. 37.2 Mucosal incision for endonasal approach.
Fig. 37.3 Mucosal incision for sublabial approach.
Abbreviations: G = gingiva; UL = upper lip.
229

VEndonasal, Transoral, and Transmaxillary Procedures
37.6.1 Critical Structures
•Alveolar branches to the frontal teeth.
•Anterior nasal spine.
•Any irregularities in the osseous nasal spine.
•Beware of subluxation of cartilaginous and bony nasal septum.
37.7 Sphenoid Sinus Dissection for Endonasal Approach
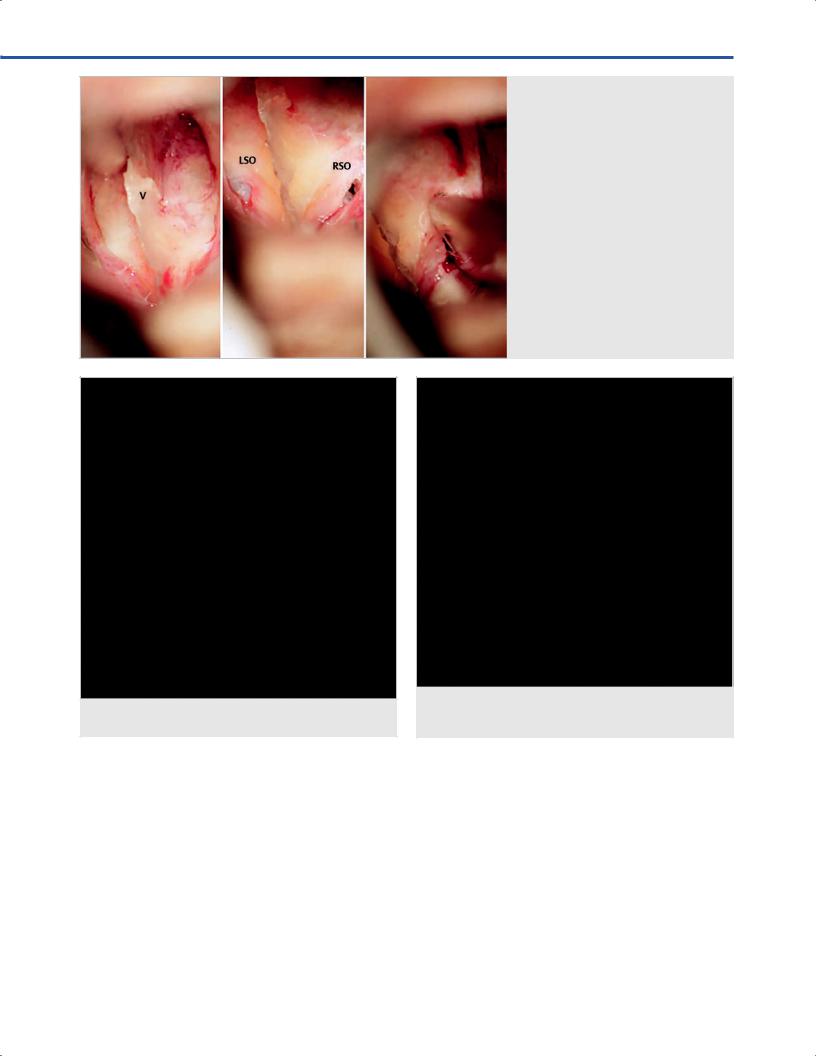
37.7.1 Bone Exposure (Figs. 37.10, 37.11)
•Subperiosteal dissection of the anterior surface of the vomer is performed.
•Bilateral exposure of ostium is carried out.
•Sphenoidotomy must be performed with forceps, rongeur, diamond drill.
37.7.2 Resection of Sphenoid Sinus
Mucosa (Fig. 37.12)
•The mucosa and mucosal polyps are extracted from the sphenoid sinus.
•Hydrogen peroxide cottonoids are inserted for hemostasis and disinfection.
37.7.3 Resection of Sphenoid Sinus
Septa (Fig. 37.13)
•Septa has to be resected, so that a complete view onto the sella foor is provided.
Fig. 37.4 Exposure of anterior margin of nasal cartilage and sub-perichondrial dissection. Abbreviations: G = gingiva; NC = nasal cartilage; SM = septal mucosa; UL = upper lip.
Fig. 37.5 Insertion of the self-retaining speculum.
•Incomplete pneumatization of the sphenoid sinus requires aggressive drilling of clivus so that a sufcient portion of the sellar foor is directly exposed.
•Bleeding from clival bone can be controlled with bone wax.
37.8 Sphenoidotomy Landmarks
Usually, the sphenoidotomy extends from both the anterior ostia until the entire sellar foor can be visualized.
230

37 Microscopic Endonasal and Sublabial Approach
•The entire sellar foor from the planum sphenoidale to the clivus has to be exposed.
•Clival and retro-sellar lesions require more posterior opening.
•Osseous canal of carotid artery is frequently encountered.
•Bone has to be maintained intact around carotid artery.
Fig. 37.6 Sub-perichondrial dissection.
Abbreviations: NC = nasal cartilage;
SM = septal mucosa.
Fig. 37.7 Junction of cartilagenous and bony nasal septum is separated. Abbreviations: BCSJ = bony-cartilage nasal septum junction; BNS = bony nasal septum.
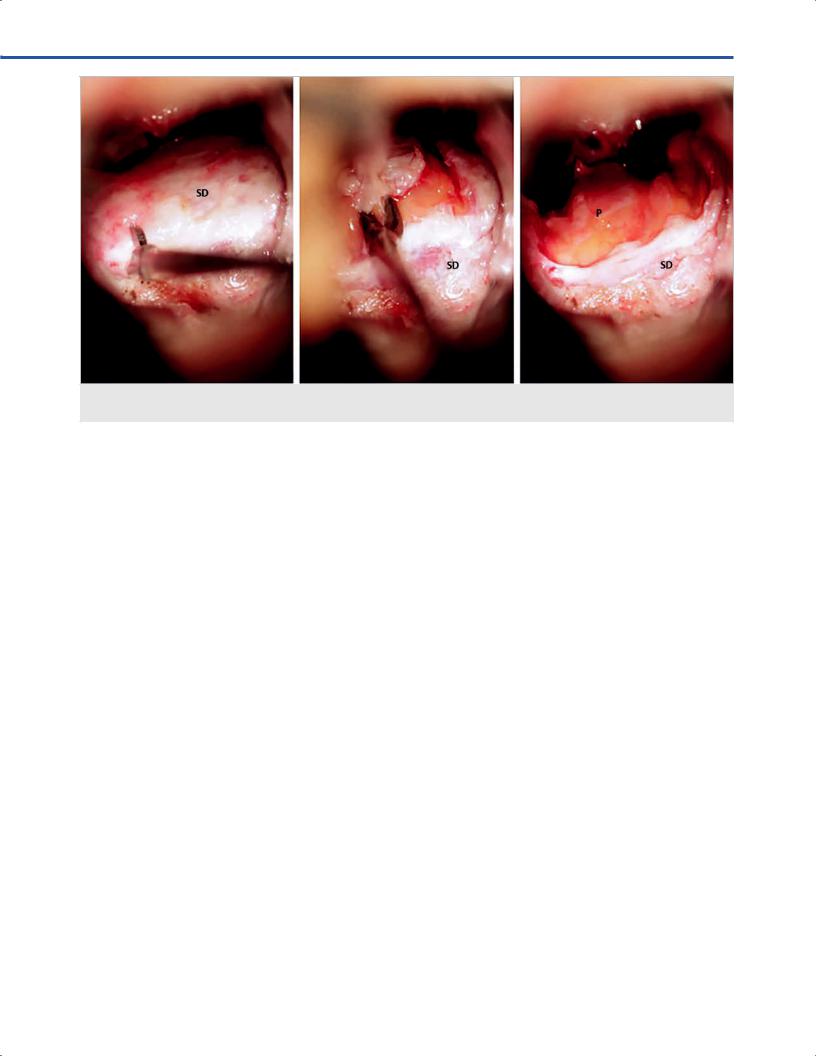
37.8.1 Exposure of the Sellar Floor
•The sellar foor is resected between both cavernous sinus with rongeur or diamond drill (Fig. 37.14).
•Dura has to be kept initially intact (Fig. 37.15).
231
VEndonasal, Transoral, and Transmaxillary Procedures
•Dural opening may be performed in X-shaped fashion or through a straight incision extended to a dural window (Fig. 37.16).
•Edges remain within the course of cavernous sinuses.
37.8.2 Critical Structures
•Cavernous sinuses.
•Internal carotid arteries, particularly in the posterior portion of sphenoid sinus.
•The arachnoid close to the junction with the anterior cranial fossa.
37.9 Intradural Exposure (See
Anatomy in Chapters 36 And 39)
•Parenchymal structures: Anterior and posterior pituitary gland.
•Arachnoidal layer: Optic-chiasmatic cistern.
•Cranial nerves: Second, third, fourth, ffth and sixth cranial nerves (only visible with invasive tumors).
•Arteries: Internal carotid arteries.
•Veins: Cavernous sinuses.
Fig. 37.8 Partial resection of bony nasal septum.
Abbreviations: BNS = bony nasal septum; reBNS = resected bony nasal septum.
Fig. 37.9 Insertion of the self-retaining speculum.
232
37 Microscopic Endonasal and Sublabial Approach
Fig. 37.11 Sphenoidotomy.
Abbreviations: SS = sphenoid sinus; SSep = sphenoid septum.
Fig. 37.10 Exposure of the vomer.
Abbreviations: LSO = left sphenoid ostium;
RSO = right sphenoid ostium; V = vomer.
Fig. 37.12 Dissection and resection of mucosa. Abbreviations: SM = sphenoid mucosa; SS = sphenoid sinus; SSep = sphenoid septum.
233

VEndonasal, Transoral, and Transmaxillary Procedures
|
|
Fig. 37.14 Exposure of the se |
. |
Abbreviations: SF = se |
. |
|
|
Fig. 37.13 Resection of bony septa. Abbreviations: SF = se ; SSep = sphenoid septum.
Fig. 37.15 Se sected and the dura is exposed. Abbreviations: SD = sellar dura.
234
37 Microscopic Endonasal and Sublabial Approach
Fig. 37.16 Dural opening and exposure of intrasellar tissue.
Abbreviations: P = pituitary gland; SD = sellar dura.
References
1.Buchfelder M, Fahlbusch R. The “classic” transsphenoidal approach for resection of pituitary tumors. Oper Techn Neurosurg. 2002;5:210–217.
2.Destrieux C, Kakou MK, Velut S, Lefrancq T, Jan M. Microanatomy of the hypophyseal fossa boundaries. J Neurosurg 1998;88(4):743–752.
3.Fatemi N, Dusick JR, de Paiva Neto MA, Kelly DF. The endonasal microscopic approach for pituitary adenomas and other parasellar tumors: a 10-year experience.
Neurosurgery 2008;63(4, Suppl 2):244–256, discussion 256.
4.Fukushima T, Sano K. Sublabial rhinoseptoplastic technique for transsphenoidal pituitary surgery by a hinged-septum method. Technical note. J Neurosurg 1980;52(6):867–870.
5.Grisoli F, Vincentelli F, Henry JF, et al. Anatomical bases for the transsphenoidal approach to the pituitary gland. Anat Clin 1982;3:207–220.
6.Romano A, Zuccarello M, van Loveren HR, Keller JT. Expanding the boundaries of the transsphenoidal approach: a microanatomic study. Clin Anat 2001;14(1):1–9.
235