


25 Midline Suboccipital Approach
S. Alexander König, Veronika Messelberger, and Uwe Spetzger
25.1 Introduction
The suboccipital approach is a midline approach to the posterior cranial fossa, which gives direct access to the suboccipital surface of the cerebellar hemispheres.
By opening the inferior medullary velum, the fourth ventricle as well as the brainstem can be accessed. The surgical approach can be tailored to accommodate the relevant pathology. Options include, supratentorial extension as well as the removal of the posterior arch of the atlas (C1).
25.2 Indications
•Parenchymal lesions of the lower cerebellum (e.g., hemorrhages, metastases, von Hippel-Lindau angiomas).
•Parenchymal lesions of the upper cerebellum and lesions in the pineal region (supracerebellar infratentorial approach).
•Lesions of the fourth ventricle (e.g., ependymomas).
•Dorsal brainstem lesions (e.g., cavernomas).
•Meningiomas of the medial posterior fossa.
•Posterior inferior cerebellar artery (PICA) aneurysms.
•Dorsal meningiomas of the foramen magnum.
•Chiari malformation.
25.3 Patient Positioning (Figs. 25.1, 25.2)
•Position: The patient is positioned prone. The head is fexed and fxed to a Mayfeld clamp.
•Body: The body is placed in a slight ’Concorde’ position with 10 to 20° of reverse Trendelenburg.
•Head: The head is maintained straight and fexed, leaving a space of about 2 cm between the chin and the chest.
•Shoulders: Shoulders are slightly pulled down for a safe position of the arms on the armrests.
•The spinous process of the third dorsal vertebra (T3) should be the highest point of patient´s body.
•The inion is the highest point in the surgical feld.
25.4 Skin Incision
•Straight skin incision on the midline
○Starting point: Incision starts 3 cm above the inion on the midline.
○Course: Incision line runs exactly along the midline.
○Ending point: It ends at the spinous process of the axis (C2).
25.4.1 Critical Structures
• None
25.5 Soft Tissues Dissection (Figs. 25.3–25.5)
•Myofascial level
○The myofascial level is incised along the midline, according to the course of the skin incision (Fig. 25.3)
•Muscles
○Origins of both trapezius muscles are detached from the occipital bone and refected laterally (Figs. 25.3, 25.4).
Fig. 25.1 Patient positioning. The head is inclined ventrall ed by a Ma ld clamp, while the patient is in prone position.
150

25 Midline Suboccipital Approach
○Further incision of the nuchal ligament along the midline is carried out.
○Semispinalis capitis is detached and refected laterally
(Fig. 25.4).
○Rectus capitis posterior minor and rectus capitis posterior major are detached and refected laterally
(Fig. 25.5).
•Bone exposure
○Subperiosteal dissection of the occipital squama laterally from the midline to both sides is performed (Fig. 25.5).
○Subperiosteal dissection of the posterior arch of the C1 vertebra is carried out.
Fig. 25.2 Patient positioning. Skin incision.
Abbreviations: C2sp = spinous process of C2;
EOP = external occipital protuberance.
Fig. 25.3 Muscles dissection and bone exposure. B ting the skin inferior to t al muscle layer will merge.
The trapezius muscle is detached from the occipital bone and the nuchal ligament in the midline (red lines).
Abbreviations: EOC = external occipital crest; EOP = external occipital protuberance;
IL = incision line; LA = linea alba; MF = muscle fascia; OA = occipital artery; OB = occipital bone; TR = trapezius muscle.
•Vertebral arteries
○The vertebral arteries are identifed by dissecting the muscle layer laterally from the posterior atlanto-occipital membrane (blunt dissection) at the cranial edge of the C1 lamina.
25.5.1 Critical Structures
•Vertebral arteries.
•Greater occipital nerve (dorsal ramus of the second cervical nerve root) close to the external occipital protuberance.
151
III Cranial Approaches
25.6 Craniotomy/Craniectomy (Figs. 25.6, 25.7)
25.6.1 Suboccipital Craniotomy Landmarks (Fig. 25.6)
•Burr holes
○I and II: The frst two burr holes are placed about
1 cm paramedian and about 1 cm below the superior nuchal line.
○III and IV: Following burr holes are placed about 3 cm below the previous two holes, at the extreme lateral aspect of the surgical feld on both sides.
Fig. 25.4 Exposure of the deep muscle layer. The semispinalis capitis muscle is detached from the occipital bone and the nuchal ligament in the midline (red lines). After detaching the semispinalis capitis muscle both posterior rectus capitis muscles are detached.
Abbreviations: EOP = external occipital protuberance; IL = incision line;
LN = ligamentum nuchae; MF = muscle fascia; RCPMA = rectus capitis posterior major muscle; RCPMI = rectus capitis posterior minor muscle; SEMC = semispinalis capitis muscle; SPC = splenius capitis muscle.
Fig. 25.5 Exposure of the occipital bone over the posterior fossa.
Abbreviations: AOM = atlanto-occipital membrane; EOC = external occipital crest; EOP = external occipital protuberance; FM = foramen magnum; M = retracted
muscles; OB = occipital bone; TR = trapezius muscle.
•Craniotomy landmarks
○Laterally: Craniotomy extends about 3.5 cm paramedian at the level of the inferior nuchal line.
○Superiorly: Bone cut runs 1 cm below the superior nuchal line.
○Inferiorly: Inferior margin of sub-occipital craniotomy is the magnum foramen.
25.6.2 Variants (Figs. 25.7, 25.8)
•Optional C1 laminectomy (Fig. 25.7)
○C1 laminectomy is indicated for surgical decompression in Chiari malformation.
○By resecting the posterior arch of C1 a special emphasis should be put on the course of the vertebral arteries.
152
25 Midline Suboccipital Approach
•Supracerebellar infratentorial approach (Krause’s approach) (Fig. 25.8)
○Krause’s approach is indicated for lesions of the upper cerebellum and of the pineal region (see Chapter 23).
○Patient is placed in a sitting position.
○Two burr holes are placed directly over the transverse sinuses as lateral as possible; one optional burr hole is made directly over the superior sagittal sinus, and two paramedian burr
Fig. 25.6 Median suboccipital craniectomy and laminectomy of C1. Placement of four burr holes over the posterior fossa. Craniotomy (red lines) from 1 cm below the superior nuchal line and down to the posterior edge of the foramen magnum.
Abbreviations: BH = burr holes; EOC = external occipital crest; EOP = external occipital protuberance; FM = foramen magnum;
M = retracted muscles; OB = occipital bone.
Fig. 25.7 Median suboccipital craniotomy/craniectomy. Abbreviations: C1 = atlas; EOP = external occipital protuberance; OS = occipital sinus; SSS = superior sagittal sinus; TS = transverse sinus.
Fig. 25.8 Supracerebellar infratentorial approach. Burr holes placed directly over the venous sinuses for optimum dura dissection and bleeding control if necessary.
Abbreviations: C1 = atlas; EOP = external occipital protuberance;
OS = occipital sinus; SSS = superior sagittal sinus; TS = transverse sinus.
153
III Cranial Approaches
holes over the posterior fossa (Fig. 25.8). Perforator drivers of modern drilling systems leave an “eggshell” of bone on the dura, especially by drilling directly over the venous sinuses.
○Blunt dissection of the dura from the internal table with a curved dissector before completing the craniotomy must be performed.
25.6.3 Critical Structures
•Vertebral arteries (laminectomy of C1)
•Transverse and superior sagittal sinuses (supracerebellar infratentorial approach)
25.7 Dural Opening (Fig. 25.9)
•Dura is opened in a Y-shaped fashion.
•Lower margin corresponds to the upper edge of the C2 lamina.
•Triangular faps are based on the superior and lateral edges of the craniotomy.
•Connection of the three cuts are not exactly in the midline to avoid heavy bleeding from the occipital sinus.
•Flaps are refected laterally and superiorly.
25.7.1 Critical Structures
•Occipital sinus.
•Transverses sinuses in case of a supracerebellar infratentorial approach.
25.8 Intradural Exposure (Fig. 25.10)
•Parenchymal structures: Cerebellar hemispheres, vermis, cerebellar tonsils, medulla oblongata.
Fig. 25.9 Median suboccipital craniectomy and laminectomy of C1. Completed craniectomy with resection of the posterior C1 arch. Y-shaped dural opening. Paramedian incision (red line) for better control of the occipital sinus.
Abbreviations: C1 = C1 remnants after laminectomy; CCJ = craniocervical junction; EOC = external occipital crest; EOP = external occipital protuberance; M = retracted muscles; OB = occipital bone; OS = occipital sinus; PFD = dura of the posterior fossa;
VP = vertebral plexus.
Fig. 25.10 Intradural exposure.
Abbreviations: A = arachnoid of the cerebello-medullary cistern; CH = cerebellar hemisphere; CF = cuneate fasciculus; GF = gracile fasciculus; MED = medulla oblongata; PFD = dura of the posterior fossa; PICA = posterior inferior cerebellar artery; sXI = spinal roots of accessory nerve (XI); TO = cerebellar tonsils; VER = vermis.
•Arachnoidal layer: Cerebello-medullary cistern.
•Cranial nerves: Spinal roots of the accessory nerve (XI).
•Arteries: Posterior inferior cerebellar arteries (PICAs), posterior spinal artery.
•Veins: Posterior spinal vein, tonsillar veins, major veins of the cerebellar hemispheres.
154
25 Midline Suboccipital Approach
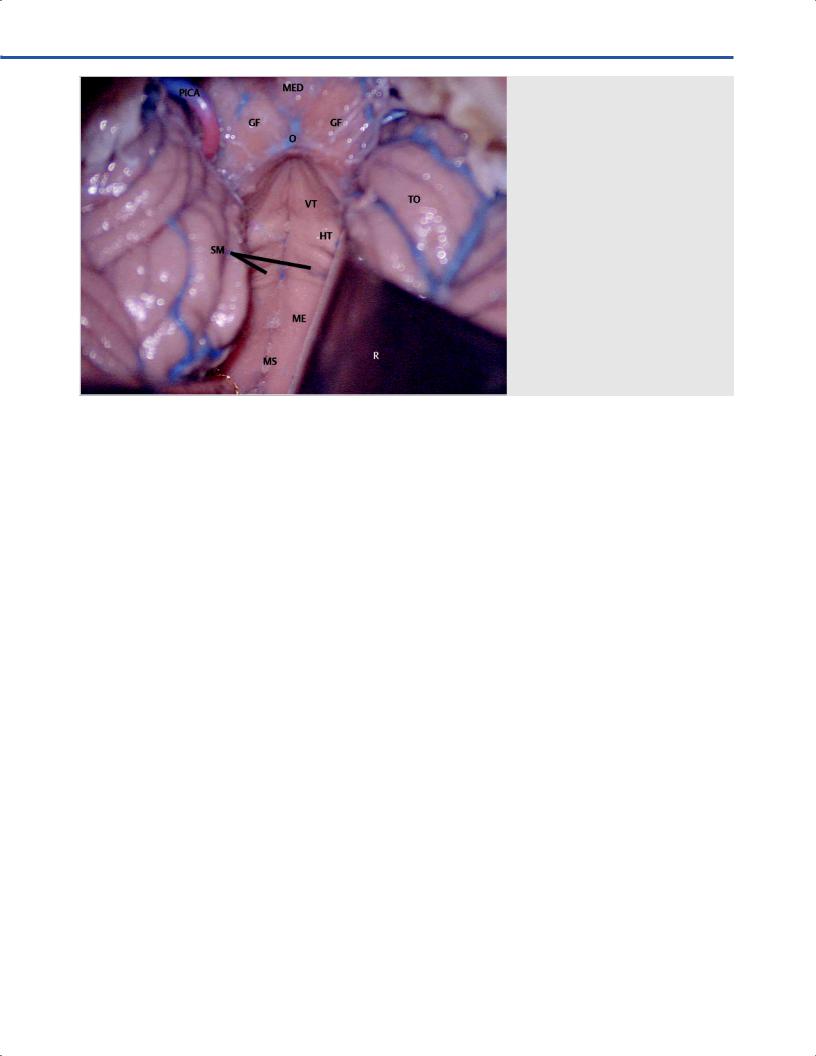
Fig. 25.11 View of t he fourth ventricle after performing a telo-velo-tonsillar approach.
Abbreviations: GF = gracile fasciculus; HT = hypoglossal triangle; ME = medial eminence; MED = medulla oblongata;
MS = median sulcus; O = obex; PICA = posterior inferior cerebellar artery; R = retractor;
SM = stria medullaris; TO = cerebellar tonsils; VT = vagal triangle.
References
1.Bertalanfy H, Sure U, Petermeyer M, Becker R, Gilsbach
JM. Management of aneurysms of the vertebral arteryposterior inferior cerebellar artery complex. Neurol Med Chir (Tokyo) 1998;38(Suppl):93–103
2.König SA, Spetzger U. Surgical strategies for supraand infratentorially grown occipital meningeomas. J Neurol Surg A Cent Eur Neurosurg 2012;73(2):79–83
155