


21 Extradural Subtemporal Transzygomatic Approach
Filippo Gagliardi, Cristian Gragnaniello, Nicola Boari, Anthony J. Caputy, and Pietro Mortini
21.1 Introduction
The subtemporal transzygomatic approach combines some of the nuances of a classic subtemporal exposure with the possibilities of a pure skull base approach, suitable for the treatment of extradural tumors of the middle-upper clivus extending into the ipsilateral paraclival area and middle fossa.
Sectioning of the mandibular branch (V3) of the trigeminal nerve and petrous apicectomy can further enlarge the surgical exposure as well as the maneuverability area and improve vascular control on the internal carotid artery.
21.2 Indications
•Extradural lesions of middle-upper clivus with lateral extension.
21.3 Patient Positioning
•Position: The patient is positioned supine with the head fxed by a Mayfeld head holder.
•Body: The body is rotated 30°.
•Head: The head is extended 20°, rotated 60° to the contralateral side and tilted 10° toward the foor.
•Shoulder: A roll is placed under the ipsilateral shoulder.
•Please note that the zygoma has to be the highest point in the surgical feld.
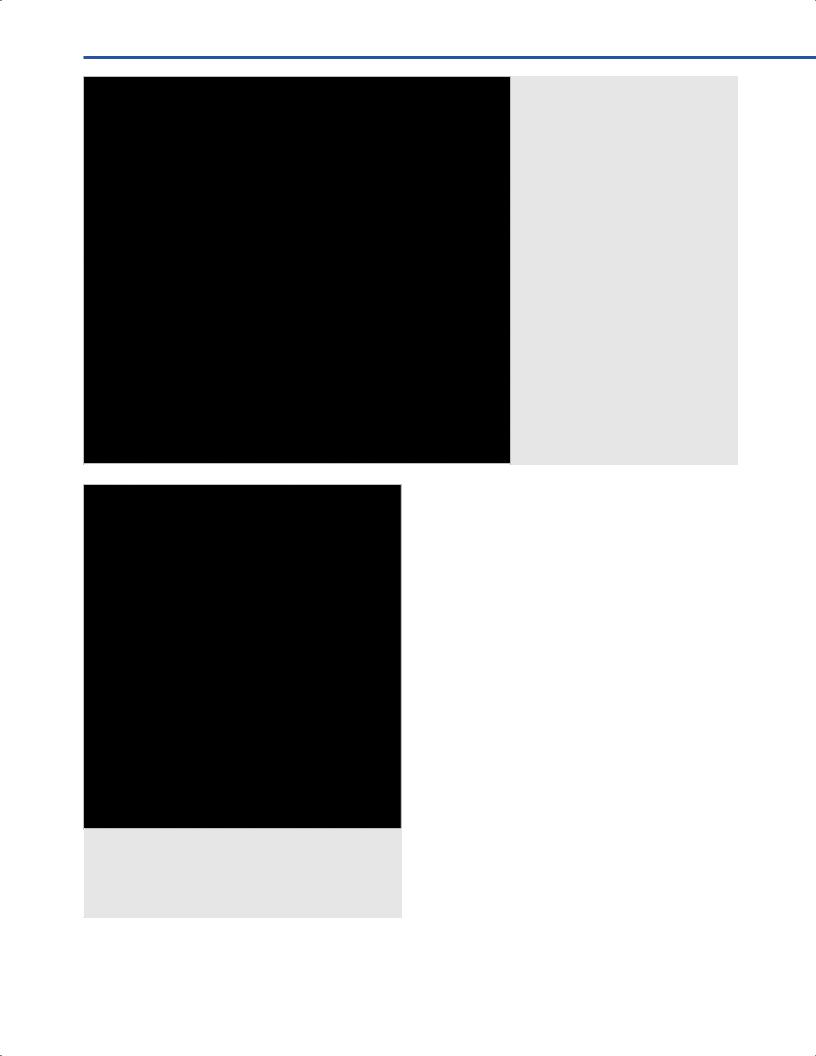
21.4 Skin Incision (Fig. 21.1)
Two main options are available for the skin fap.
•Question-mark shaped unilateral temporal incision
○Starting point: Incision starts 1 cm in front of the tragus at the level of the zygoma.
○Course: Incision line runs posteriorly around the superior margin of the ear; turns anteriorly after reaching the posterior aspect of the pinna.
○Ending point: It ends on the midline, just behind the hairline.
•Coronal bilateral incision
○Starting point: Incision starts 1 cm in front of the tragus at the level of the zygoma.
○Course: Incision line runs medially, parallel and behind the hairline.
○Ending point: It ends at the contralateral superior temporal line.
21.4.1 Critical Structures
•Superfcial temporal artery.
•Frontal and temporal branches of the facial nerve.
Fig. 21.1 Question-mark shaped unilateral temporal incision.
Abbreviations: Incision (red dotted line); midline (black continuous line); zygomatic
black dotted line). E = ear; N = nasion; Z = zygoma.
128

21 Extradural Subtemporal Transzygomatic Approach
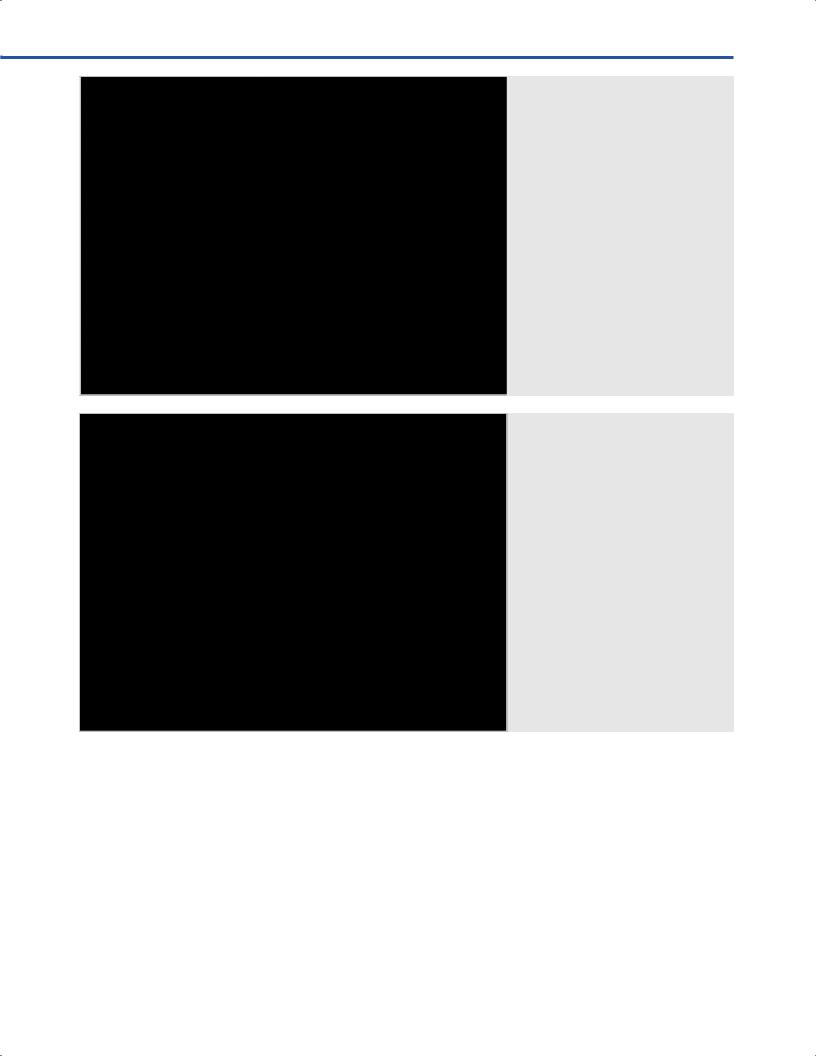
21.5 Soft Tissue Dissection and Zygomatic Osteotomy
(Figs. 21.2, 21.3)
•Myofascial level
○The myofascial level is incised parallel to the course of the skin incision.
○The fap is refected anteriorly with the skin.
•Muscles: Step 1
○Temporal muscle: inter-fascial dissection is carried out as it is already described (see Chapters 6 and 8).
○Deep temporal muscle fascia is detached from the inner surface of the zygoma.
○Masseter muscle is detached from the inferior margin of the zygoma.
21.5.1 Zygomatic Osteotomy
•Cuts
○I: Posterior cut is made in front of the mandibular fossa.
○II: Anterior cut is made at the basis of the zygomatic temporal process.
•Muscles: Step 2
○Temporal muscle is incised posteriorly along the posterior margin of the skin incision.
○Temporal muscle insertion is cut along the superior temporal line.
Fig. 21.2 Soft tissue dissection. Abbreviations: Temporal muscle insertion incision (black dotted line); Limits of zygomatic osteotomy (red dotted lines); E = ear;
FB = frontal bone; FZS = fronto-zygomatic suture; MM = masseter muscle; PO = periorbit; SON = supraorbital nerve; TMF = temporal muscle fascia; TMFP = temporal muscle fat pad; Z = zygoma.
•Bone exposure
The bone exposure is completed, when the following structures come into view:
○Temporal squama, outer surface of sphenoid greater wing, pterion, inferior aspects of frontal and parietal bone located below the superior temporal line.
21.5.2 Critical Structures
• Frontal branch of the facial nerve.
21.6 Craniotomy/Craniectomy (Fig. 21.4)
A temporal, low-positioned craniotomy, including the greater sphenoid wing and the squamosal part of the temporal bone is performed.
21.6.1 Temporal Craniotomy
•Burr holes
○I: At the McCarty keyhole.
○II: At the posterior aspect of temporal squama just below the superior temporal line.
○III: At the greater wing of the sphenoid bone at the zygomatic level.
129
III Cranial Approaches
Fig. 21.4 Schematic picture resembling osteotomy and craniotomy landmarks. I, II, III: sequential order of the craniotomy cuts. Arrows indicate direction of the craniotomy cuts. Black dotted line = superior temporal line. Red dotted line = connection of the burr holes by drilling the greater wing of the sphenoid bone with a high-speed drill.
Fig. 21.3 Bone exposure after zygomatic osteotomy and temporal musc tion. Abbreviations: Craniotomy margins (black dotted line); E = ear; PO = periorbit; TM = temporal muscle; TMFP = temporal muscle fat pad; TSq = temporal squama; Z = zygoma.
•Craniotomy landmarks
○Anteriorly: Anterior margin of spheno-temporal fossa.
○Posteriorly: External auditory canal.
○Superiorly: Superior temporal line.
○Inferiorly: Middle fossa foor.
21.6.2 Further Osteotomies
•Lateral orbitotomy.
•Extradural clinoidectomy.
21.6.3 Middle Fossa Floor Drilling
The temporal dura is gently separated from middle fossa foor, which is drilled using a diamond burr.
•Sequential exposure of anatomical landmarks (Fig. 21.5)
○I: Arcuate eminence.
○II: Greater superfcial petrosal nerve (GSPN).
○III: Middle meningeal artery (MMA) and foramen spinosum.
○IV: Mandibular nerve (V3) and foramen ovale.
○V: Maxillary nerve (V2) and foramen rotundum.
○VI: Superior orbital fssure.
•Surgical steps of middle fossa dissection (Figs 21.6, 21.7)
○GSPN division (to protect the geniculate ganglion from mechanical and thermal injury).
○MMA division, on the dural side, distal and away from the foramen, to avoid retraction of the artery inside the foramen, which may lead to difcult to control bleeding.
○Skeletonization of the foramen rotundum and ovale.
130
21 Extradural Subtemporal Transzygomatic Approach
○Sphenoid sinus opening (medially and rostrally to the vidian nerve).
○Vidian canal skeletonization (between V2 and V3).
○Eustachian tube isolation (laterally and caudally to the vidian nerve).
○V2 division at the foramen rotundum.
○V3 division at the foramen ovale.
○Pituitary and ipsilateral carotid prominences skeletonization.
○Middle clival dura exposure.
○Skeletonization of the contralateral carotid, V2 and V3.
Fig. 21.5 Middle fos illing. Skeletonization of V2, V3 and middle meningeal artery, further opening of the sphenoid sinus.
Abbreviations: ACP = anterior clinoid process; FO = foramen ovale; FR = foramen rotundum; FS = foramen spinosum;
MMA = middle meningeal artery;
PPF = pterygopalatine fossa; PO = periorbit; SOF = superior orbit sure; SSM = sphenoid sinus mucosa; SSop = sphenoid sinus opening; TM = temporal muscle;
V2 = second branch of trigeminal nerve;
V3 = third branch of trigeminal nerve; Z = zygoma.
Fig. 21.6 Middle fos illing. Skeletonization of the Vidian nerve. Abbreviations: ACP = anterior clinoid process; FO = foramen ovale; FR = foramen rotundum; FS = foramen spinosum;
MMA = middle meningeal artery;
PPF = pterygopalatine fossa; PO = periorbit; R = retractor; SOF = superior orbit sure; SS = sphenoid sinus; SSop = sphenoid sinus opening; TM = temporal muscle;
V2 = second branch of trigeminal nerve;
V3 = third branch of trigeminal nerve; VN = Vidian nerve; Z = zygoma.
21.6.4 Petrous apicectomy (Fig. 21.8)
This maneuverer allows for exposure of posterior fossa dura and for internal carotid artery (ICA) mobilization
•ICA is freed from the carotid sulcus trough the resection of the petrolingual ligament.
•Petrous bone apex is drilled.
•ICA is mobilized posteriorly and laterally.
•Gives access to a blind corner located at the lateral edge of the middle clivus, medial to the horizontal segment of the ICA.
131
III Cranial Approaches
21.6.5 Critical Structures
•Ipsilateral superior orbital fssure.
•Ipsilateral and contralateral V2.
•Ipsilateral and contralateral V3.
•Ipsilateral and contralateral ICA.
•Ipsilateral Eustachian tube.
References
1.al-Mefty O, Anand VK. Zygomatic approach to skull-base lesions. J Neurosurg 1990;73(5):668–673
Fig. 21.7 Middle fos illing. Skel - etonization of the carotid canal and the Eustachian tube.
Abbreviations: ACP = anterior clinoid process; ET = Eustachian tube; MMA = middle meningeal artery; PPF = pterygopalatine fossa; PO = periorbit; R = retractor; RICA = right internal carotid artery; SOF = superior orbital sure; SS = sphenoid sinus; SSop = sphenoid sinus opening; TM = temporal muscle;
V2 = second branch of trigeminal nerve;
V3 = third branch of trigeminal nerve; VN = Vidian nerve; Z = zygoma.
Fig. 21.8 Final dural exposure (Eustachian tube and pterygopalatine fossa are not in view).
Abbreviations: LCS = left cavernous sinus; LGG = left Gasserian Ganglion; LICA = left internal carotid artery; LV1 = lef st branch of the trigeminal nerve; LV2 left second branch of trigeminal nerve; LV3 = left third branch of trigeminal nerve; P = pituitary; PAP = petrous apex; R = retractor;
RICA = right internal carotid artery; RV2 = right second branch of trigeminal
nerve; RV3 = right third branch of trigeminal nerve; TM = temporal muscle; Z = zygoma.
2.Sekhar LN, Janecka IP, Jones NF. Subtemporal-infratemporal and basal subfrontal approach to extensive cranial base tumours. Acta Neurochir (Wien) 1988;92(1–4):83–92
3.Sekhar LN, Schramm VL Jr, Jones NF. Subtempo- ral-preauricular infratemporal fossa approach to large lateral and posterior cranial base neoplasms. J Neurosurg 1987;67(4):488–499
132