

11 Supraorbital Approach
Phillip A. Bonney, Andrew K. Conner, and Michael E. Sughrue
11.1 Introduction
The supraorbital approach is a frontal approach, which is suitable for the unilateral exposure of the anterior skull base. The surgical route corresponds to the anatomical corridor seated between the inferior aspect of the frontal lobe and the foor of the anterior cranial fossa.
The approach is mainly indicated in case of vascular lesions of the anterior circulation as well as of lesions involving the anterior skull base as well as the parasellar areas.
11.2 Indications
•Anterior circulation aneurysms.
•Anterior skull base meningiomas.
•Parasellar tumors (e.g., craniopharyngiomas).
•Less common: posterior circulation aneurysms, inferior frontal pathology.
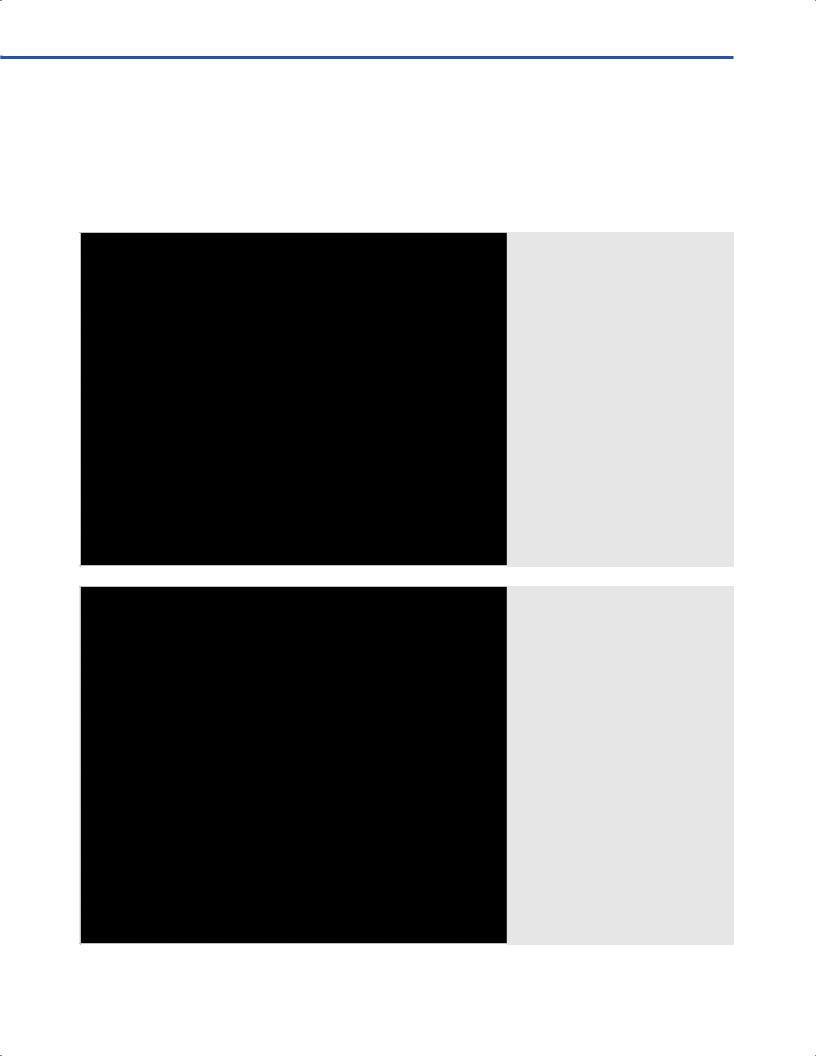
11.3 Patient Positioning (Fig. 11.1)
•Position: Patient is positioned supine in a 20° of reverse Trendelenburg position.
•Head: The head is extended 20°, rotated 5°-15° to the contralateral side for most pathology; for anterior lesions near the midline (e.g., olfactory groove meningiomas) rotation may be up to 60°.
•The malar eminence is the highest point in the surgical feld.
•Ipsilateral temporary tarsorrhaphy is performed to protect the cornea.
11.4 Skin Incision (Fig. 11.2)
•Slightly curved incision
○Starting point: Incision starts just medial to supraorbital notch.
Fig. 11.2 Planned incision through the eyebrow, running from just medial to the supraorbital notch to the edge of the brow. If more medial access is necessary, care should be taken to
preserve the supraorbital nerve, which can be found deep to the frontalis muscle.
Abbreviations: FH = forehead; N = nose; RE = right eye; SN = supraorbital notch.
Fig. 11.1 Patient positioning.
72
11 Supraorbital Approach
○Course: Incision line runs within hair-bearing skin of the eyebrow.
○Ending point: It ends at the lateral edge of the brow (may be extended up to 1 cm).
11.4.1 Critical Structures
• Supraorbital nerve
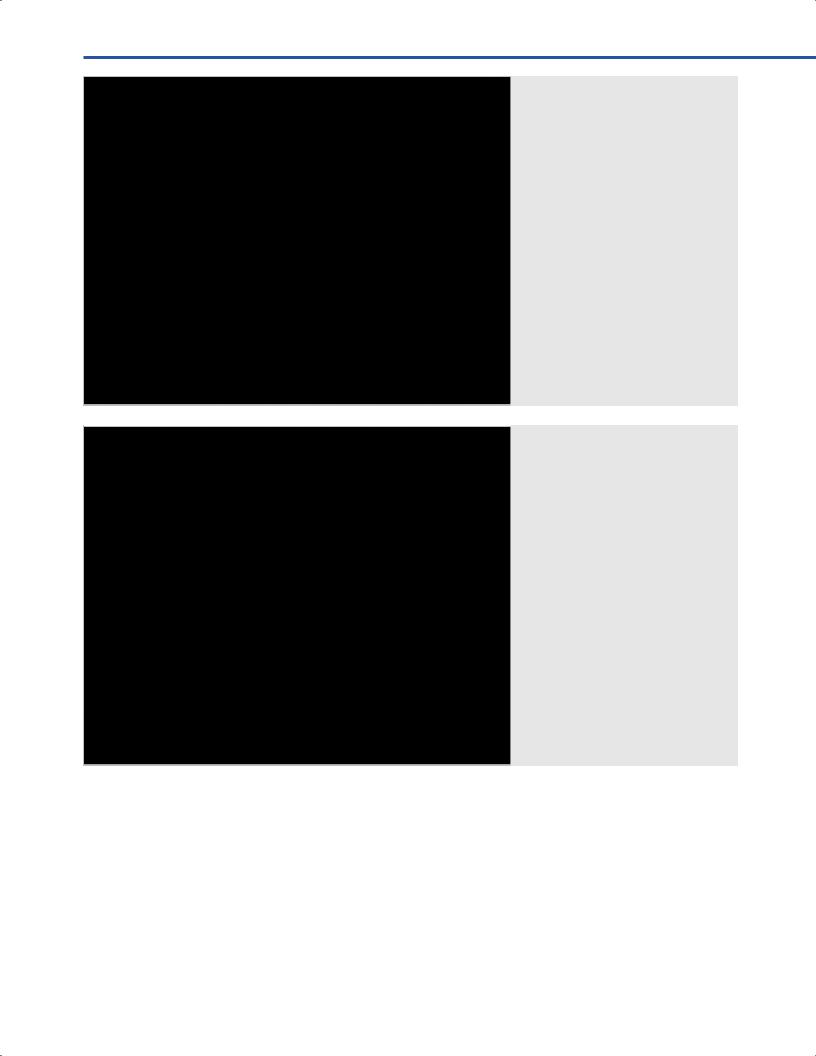
11.5 Soft Tissue Dissection (Figs. 11.3–11.5)
•Myofascial and muscular layers
○The frontal muscle is divided with monopolar electrocautery along the path of the incision.
○Usually this does not need to extend medially to the supraorbital notch.
Fig. 11.3 Muscle dissection: frontal muscle is divided in the plane of the incision. Abbreviations: FH = forehead; FM = frontalis muscle; N = nose; RE = right eye.
Fig. 11.4 Muscle dissection: the supraorbital nerve may be ident o the frontalis muscle and carefully retracted medially if required.
Abbreviations: FH = forehead; FM = frontalis muscle; N = nose; RE = right eye; SON = supraorbital nerve.
73
III Cranial Approaches
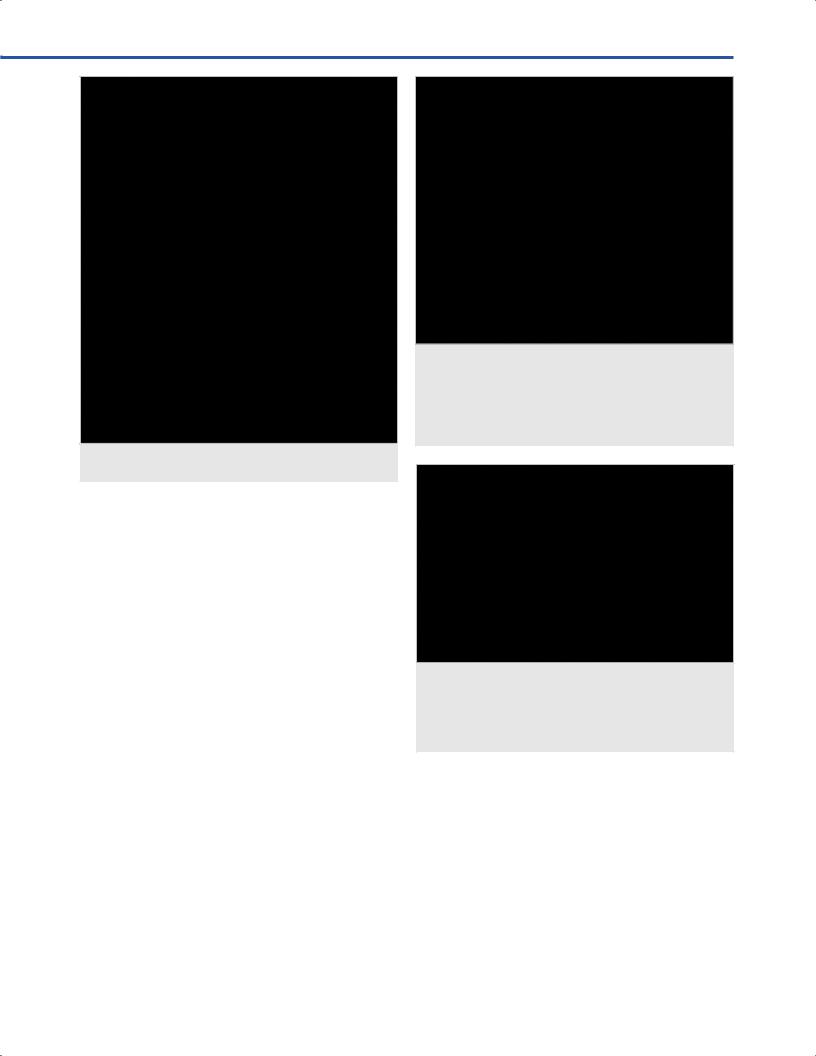
○The muscle is elevated and refected superiorly with scalp hooks.
•Bone exposure
○The pericranium is cut along the superior edge of the skin incision.
○The medial edge of the temporal muscle is dissected with the pericranium to expose the lateral orbital rim.
○Subperiosteal dissection proceeds until the frontozygomatic suture is visible.
○The pericranial fap is elevated of the bone, refected inferolaterally, and sutured down.
Fig. 11.5 Bone exposure: after scalp hooks are placed to retract the skin superiorly, a pericrani tarted along the superior edge.
Abbreviations: FH = forehead; N = nose; P = pericranium; RE = right eye; SOA = supraorbital artery; STA = supratrochlear artery.
Fig. 11.6 Bone exposure: the pericranial ted anteriorly and inferiorly and
sutured down along the inferior margin of t eyhole is exposed utilizing sub-periosteal dissection with the temporal
musc |
ted laterally. Care should be |
|
taken to avoid dissect |
al to the |
|
al temporalis fascia to avoid damage to the frontalis branch of the facial nerve. Abbreviations: FB = frontal bone; FH = forehead; FZS = frontozygomatic suture; KH = keyhole; N = nose; P = pericranium; TM = temporal muscle.
11.6 Craniotomy (Figs. 11.6, 11.7)
•Burr hole
○I: The single burr hole is made at the keyhole.
•Craniotomy landmarks
Anatomical landmarks that must be taken into consideration when designing the craniotomy are
○Medially: Lateral wall of the frontal sinus or supraorbital nerve.
○Laterally: Keyhole.
74
11 Supraorbital Approach
Fig. 11.7 Outline of the craniotomy on skull model. Abbreviations: BH = burr hole; SN = supraorbital notch.
○Superiorly: Approximately 1.5-2 cm above the frontal foor.
○Inferiorly: Orbital roof.
•The craniotomy is made near the frontal foor approximately
2-3 cm wide and 1.5-2 cm high.
•The medial border of the craniotomy should not extend to the frontal sinus.
•Image guidance is helpful to identify the lateral wall of the frontal sinus, which is usually, but not always, medial to the supraorbital notch.
11.6.1 Critical Structures
•Frontal sinus.
•Supraorbital nerve.
•Orbital roof.
11.7 Dural Opening (Fig. 11.8)
•The dura is frst separated from the orbital roof and bony prominences are drilled down so that the orbital roof is fush with the sphenoid wing.
•The dural opening is a C-shaped incision based inferiorly.
11.7.1 Critical Structures
• None.
Fig. 11.8 Dural opening. The bony prominences of the orbital
roof are dr |
t to the sphenoid wing. If the orbital roof is |
|
transgressed, periorbital fat will be evident. A C-shaped dural |
||
opening is made. |
|
|
Abbreviations: D = dura; FF = front |
; FH = forehead; FL = frontal |
|
lobe; N = nose; OR = orbital rim; P = pericranium; TM = temporal muscle.
Fig. 11.9 The frontal lobe has fallen back allowing visualization of the suprasellar region.
Abbreviations: AC = anterior clinoid process; ACF = anterior cranial fossa; BA = basilar artery; FL = frontal lobe; ICA = internal carotid artery; III = third cranial nerve; M2 = M2 segment of middle cerebral artery; ON = optic nerve; OR = orbital ridge.
11.8 Intradural Exposure (Fig. 11.9)
•Parenchymal structures: Orbital gyrus, pituitary, mammillary bodies, lamina terminalis, brainstem.
•Arachnoid layer: Sylvian cistern, opticocarotid cistern, suprasellar cistern, interpeduncular cistern.
•Cranial nerves: I, II, III, IV cranial nerves.
•Arteries: Internal carotid artery (ICA), middle cerebral artery (MCA), anterior cerebral artery (ACA), anterior
75

III Cranial Approaches
choroidal artery (AChA), posterior communicating artery (PcoA).
• Veins: Cavernous sinus, Sylvian fssure veins.
11.9 Pearls
•Having enough room to work requires accessing and draining CSF spaces early. Understanding this concept is the most important aspect of the procedure.
•The 30° endoscope aids in visualizing beyond the feld of the microscope. This can be used, for example, when inspecting the sella for residual tumor or assessing the clipping of an aneurysm.
•Optimal cosmetic outcomes can be achieved with a careful attention paid to closure techniques.
References
1.Little AS, Gore PA, Darbar A, et al. Supraorbital eyebrow approach: a less invasive corridor to lesions of the anterior cranial fossa, parasellar region, and ventral brainstem. In: Cappabianca P, Califano L, Iaconetta G, eds. Cranial, craniofacial, and skull base surgery. Milan: Springer; 2010
2.Teo C, Sughrue ME. Principles and practice of keyhole brain surgery. New York, NY: Thieme Medical Publisher; 2014
76