


l!1lEJ1l!DijCirculatory System |
1 85 |
b.Myocardium consists of layers of striated cardiac muscle cells arranged in a spiral fashion about the heart's chambers and inserted into the fibrous skeleton. The myocardium contracts to propel blood into the arteries for distribution to the body.
c.Epicardium, the outermost layer of the heart, constitutes the visceral layer of the pericardium. It is composed of simple squamous epithelium (mesothelium) on the external surface. Beneath the mesothelium lies fibroelastic connective tissue, containing nerves, the coronary vessels, and adipose tissue.
2.The fibrous skeleton of the heart consists of thick bundles of collagen fibers oriented in various directions and especially oriented to support the fourvalve rings of the heart valves. It also contains occasional foci of fibrocartilage.
3.Heartvalves
a.Atrioventricular (AV) valves are composed of a skeleton of fibrous connective tissue, arranged like an aponeurosis, and lined on both sides by endothelium. They are attached to the annuli fibrosi of the fibrous skeleton. The right AV valve is formed of three interlocking cusps (tricuspid valve), whereas the left AV valve is formed of two interlocking cusps (bicuspid or mitral valve). These valves prevent regurgitation of ventricular blood into the atria.
b.Semilunar valves in the pulmonary and aortic trunks are each composed ofthree cusps that approximate each other as they fill with arterial blood. They are lined with endothelium on both sides separated by sparse strands of connective tissue. These valves prevent regurgitation of pulmonary and aortic blood into the respective ventricles.
CLINICAL |
Rheumatic heartvalve disease is a sequel to childhood rheumatic fever (sub |
|
CONSIDERATIONS |
||
sequent to streptococcal infection), which causes scarring of the heartvalves. |
||
|
1.The disease is characterized by reduced elasticity of the heart valves, making them unable to close (incompetence) or unable open (stenosis) properly.
2.It most commonly affects the mitral valve, followed by the aortic valve.
4.The impulse-generating and impulse-conducting system of the heart comprises several specialized structures with coordinated functions that act to initiate and regulate the heartbeat.
a.The sinoatrial (SA) node, the pacemaker of the heart, is composed of specialized cardiac cells located within the wall of the right atrium adjacent to the entry of the superior vena cava into the heart. It generates impulses that initiate contraction of atrial muscle cells; which are then conducted to the AV node.
b.The AV node is located in the wall of the right atrium, adjacent to the tricuspid valve.
c.The AV bundle of His is a band of conducting tissue radiating from the AV node into the interventricular septum, where it divides into two branches and continues as Purkinje fibers.
d.Purkinje fibers are large, modified cardiac muscle cells (see Chapter 8 V B 9) that make contact with cardiac muscle cells at the apex of the heart via gap junctions, desmosomes, and fasciae adherentes.
e.As indicated (in Section I B of the current chapter), the autonomic nervous system modulates the heart rate and stroke volume.
Cardiac arrest occurs when the heart ceases to beat, resulting in cessation of blood flow in the entire circulatory system. Cardiac death
is imminenet unless cardiopulmonary resuscitation and defibrillation are conducted successfully and the electrical system of the heart is revived . Health conditions that may lead to cardiac arrest include, but are not limited to, tachycardia, fibrillation, and bradycardia.

t a b l e |
11.1 |
1 86 |
BRS Cell Biology and Histology |
Comparison of Tunicae in Different Types of Arteries
Tunica Components |
Elastic Arteries |
Muscular Arteries |
Arterioles |
Metarterioles |
Intima |
|
|
|
|
Endothelium |
+ |
+ |
+ |
+ |
Factor VIII in endothelium |
+ |
+ |
+ |
|
Basal lamina |
+ |
+ |
+ |
+ |
Subendothelial layer* |
+ |
+ |
± |
|
Internal elastic lamina |
Incomplete |
Thick, complete |
Some elastic fibers |
|
Media |
|
|
|
|
Fenestrated elastic membranes |
40-70 |
|
|
|
Smooth muscle cells |
Interspersed between |
:s:40 layers |
1 or 2 1ayers |
Discontinuous |
|
elastic membranes |
|
|
layer |
External elastic lamina |
Thin |
Thick |
|
|
Vasa vasorum |
± |
|
|
|
Adventitia |
|
|
|
|
Fibroelastic connective tissue |
Thin layer |
Thin layer |
|
|
Loose connective tissue |
|
|
+ |
|
Vasa vasorum |
+ |
|
|
|
Lymphatic vessels |
+ |
+ |
|
|
Nerve fibers |
+ |
+ |
+ |
|
|
|
|
|
|
+ , present and prominent; ± , present but not prominent; -, absent.
*In elastic arteries. the subendothelial layer is composed of loose connective tissue containing fibroblasts. collagen. and elastic fibers. In arterioles. this layer is less prominent; the connective tissue is sparse and contains a few reticular fibers.
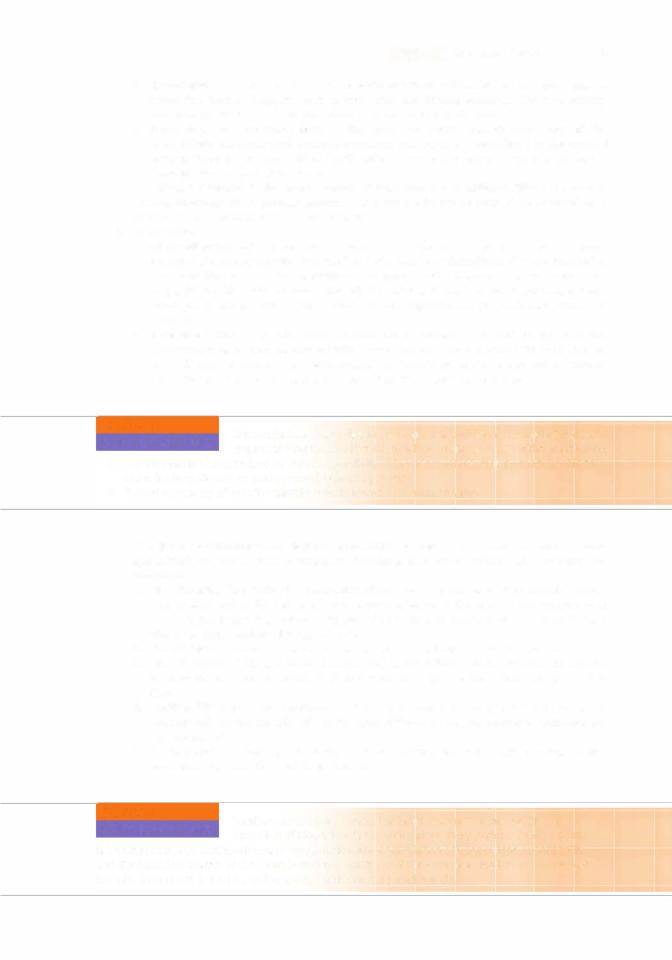
C.Arteries conduct blood away from the heart to the organs and tissues. Arterial walls are composed of three layers (tunicae): the tunica intima (inner), tunica media (middle), and tunica adventitia (outer). Components of these layers and variations among types of arteries are summarized in
Table 11 . 1 .
1 . TypesI of arteries
a.Elastic arteries (conducting arteries)are large and include the aorta andits major branches
(Figures 1 1 . 1 and 1 1 .2).
(1 Elastic arteries help reduce changes in blood pressure associated with the heartbeat.
(2)Small vessels (vasa vasorum) and nerves are located in their tunicae adventitia and
media. The vasa vasorum vascularizes the walls of the elastic arteries.
IThick, concentric sheaths of elastic membranes, known as fenestrated membranes, are located in the tunica media.
b.Muscular arteries (distributing arteries) distribute blood to various organs. (1 They include most of the named arteries of the human body.
(2) These medium-sized arteries are smaller than elastic arteries but larger than arterioles.
(3) The tunica adventitia contains vasa vasorum.
(4) The tunica media is thick, composed oflayers of smooth muscle cells. Larger muscular
arteries possess an external elastic lamina separating their boundary with the tunica adventitia (Figure 1 1 .3).
(51 The tunica intima is characterized by its endothelium and a prominent subendothelial internal elastic lamina.



l!1lEJ1l!DijCirculatory System |
1 91 |
a.Continuous (somatic) capillaries contain numerous pinocytotic vesicles except in the central nervous system (CNS), where they contain only a limited number of pinocytotic vesicles (a property that is partly responsible for the blood-brain barrier).
(1 ) Continuous capillaries lack fenestrae and have a continuous basal lamina.
(2)They are located in nervous tissue, muscle, connective tissue, exocrine glands, and the lungs.
b.Fenestrated (visceral) capillaries are formed from endothelial cells that are perforated withfenestrae. These openings are 60 to 80 nm in diameter and are bridged by a diaphragm thinner than a cell membrane; in the renal glomerulus, the fenestrae are larger and lack a diaphragm.
(1 ) Fenestrated capillaries have a continuous basal lamina and few pinocytotic vesicles.
(2)They are located in endocrine glands, the intestine, the pancreas, and the glomeruli of kidneys.
c.Sinusoidal capillaries (sinusoids) possess many large fenestrae that lack diaphragms.
(1 ) Sinusoidal capillaries are 30 to 40 IJ,m in diameter, much larger than continuous and fenestrated capillaries.
(2)Sinusoidal capillaries have a discontinuous basal lamina and lack pinocytotic vesicles.
(3)Gaps maybe present at the cell junctions, permitting leakage between endothelial cells.
(4)They are located in the liver, spleen, bone marrow, lymph nodes, and adrenal cortex.
3.Permeability of capillaries is dependent on the morphology of their endothelial cells and on the size, charge, and shape of the traversing molecules. Permeability is altered during the inflammatory response by histamine and bradykinin.
a.Some substances diffuse, whereas others are actively transported across the plasma membrane of capillary endothelial cells.
b.Other substances move across capillary walls via small pores (intercellular junctions) or large pores (fenestrae and pinocytotic vesicles).
c.Leukocytes leave the bloodstream to enter the tissue spaces by penetrating intercellular junctions. This process is called diapedesis.
4.Metabolic functions of capillaries are carried out by the endothelial cells, and include the following (see Table 1 1 .2):
a.Conversion of inactive angiotensin I to active angiotensin II (especially in the lung). This powerful vasoconstrictor also stimulates secretion of aldosterone, a hormone that promotes water retention.
b.Deactivation of various pharmacologically active substances (e.g., bradykinin, serotonin, thrombin, norepinephrine, prostaglandins).
c.Breakdown of lipoproteins to yield triglycerides and cholesterol.
d.Release of prostacyclin, a potent vasodilator and inhibitor of intravascular platelet
|
aggregation. |
e. |
Release of the relaxing factor NO (nitric oxide) and contraction factor (endothelin 1). |
f. |
Regulation oftransendothelial migration ofinflammatory cells (neutrophils). |
g.Release of tissue factors responsible for blood coagulation.
5.Blood flow to capillary beds occurs either from metarterioles (with precapillary sphincters) or from terminal arterioles (Figure 1 1 .5).
a.Central channels are vessels that traverse a capillary bed and connect arterioles to small venules. Their proximal portion is the metarteriole (possessing precapillary sphincters), and their distal portion is the thoroughfare channel (with no precapillary sphincter) (see Figure 1 1 .5).
b.Metarterioles supply blood to the capillary bed, whereas thoroughfare channels receive blood from capillary beds.
6.Arteriovenous shunt (bypassing a capillary bed)
a. Contraction of precapillary sphincters forces the blood flow from the metarteriole directly
into the thoroughfare channel, thus bypassing the capillary bed and draining into a postcapillary venule.
b.AV anastomoses are small vessels that directly connect arterioles to venules, bypassing the capillary bed. They function in thermoregulation, especially in the skin where they are abundant. These anastomoses also control blood pressure and flow.



1 94 |
BRS Cell Biology and Histology |
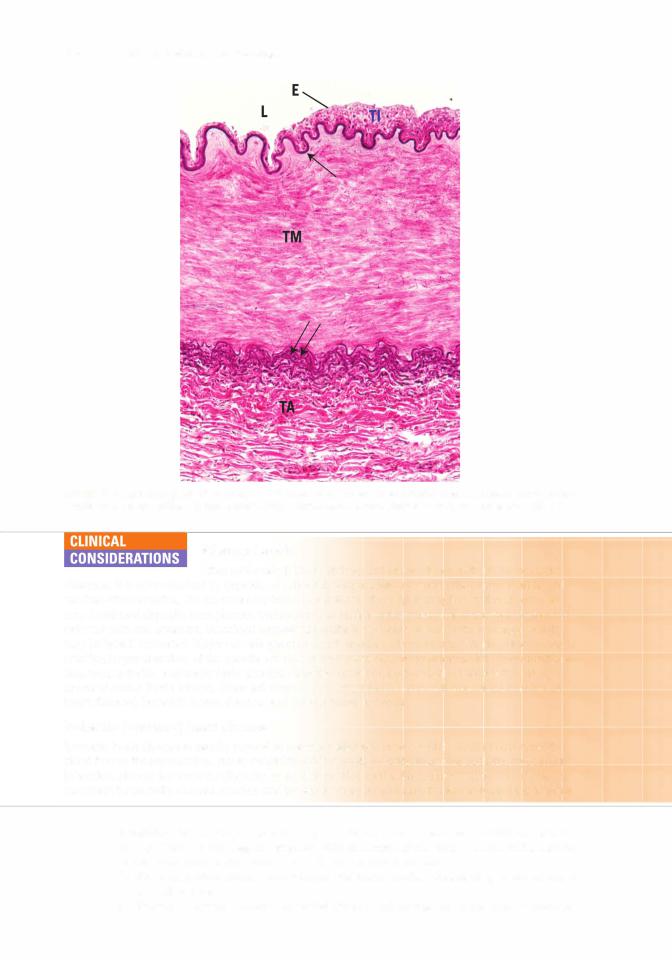
FIGURE 11 .6. Light micrograph of an artery and vein ( X 270l. Vein-lumen (LVI, tunica media (TMVI, and tunica adventitia (TAVI. Artery-tunica adventitia (TAAI, tunica media (TMAI. and lumen (LAI.
b. Small and mediuml -sized veins includel the external jugular vein. These veins have a diameter of to 9 mm.
c. Venules have a diameter of 0.2 to mm and are involved in exchange of metabolites with tissues and in diapedesis (exiting of blood cells through vessel walls).
Varicose veins are abnormally tortuous dilated veins, usually of the leg. 1. They are caused by a decline in muscle tone, degenerative alteration
of the vessel wall, and valvular incompetence. They generally occur in older people, being most prevalent in women. Pregnant women are also susceptible to varicose veins.
2.When they occur in the region of the anorectal junction, they are known as hemorrhoids.
F.Specialized sensory mechanisms within arteries include three types of sensors: the carotid sinus, the carotid body, and the aortic bodies.
1.Carotid sinus is a baroreceptor in the wall ofthe internal carotid arteryjust as it begins at the common carotid artery. Sensory endings of the glossopharyngeal nerve embedded with the wall of the artery are sensitive to changes in pressure that distend the vessel, thus initiating a signal to the vasomotor center of the brain. The resultant response triggers adjustments to the tension on the arterial wall via the smooth muscles of the tunica media, effecting changes in
2.Carotid body is a chemoreceptor at the bifurcation of the commonl)carotid artery. Specialized nerve endings of the vagus and glossopharyngeal cranial nerves are sensitive to oxygen and carbon dioxide levels as well as H+ concentration. Glomus (type cells and sheath (type 2)

l!1lEJ1l!DijCirculatory System |
1 95 |
cells, which envelop the glomus cells, constitute the parenchyma. Nerve endings lose their Schwann cells upon entering the parenchyma, becoming covered instead by sheath cells. Impulses are shuttled to the brain by these two cranial nerves for processing.
3.Aortic bodies are located in the wall of the arch of the aorta at the junction of the common carotid and subclavian arteries. Their structure and function are similar to those of the carotid body.
4.Hormonal control of low blood pressure starts with the kidney:
a.Kidney produces renin
b.Renin cleaves angiotensinogen circulating in the blood, forming angiotensin I, a mild vasoconstrictor.
c.Angiotensin I is converted into angiotensin II by angiotensin-converting enzyme (ACE), located on the luminal plasmalemmas of capillary endothelia (especially capillaries of the lungs).
d.Angiotensin II, a potent vasoconstrictor, causes the walls of arterioles to contract, which raises blood pressure.
e.Antidiuretic hormone, or vasopressin, secreted by the pituitary gland, is another potent vasoconstrictor employed after severe hemorrhage.
This system consists of peripheral lymphatic capillaries, lymphatic vessels of gradually increasing size, and lymphatic ducts. The lymphatic vascular system collects excess tissue fluid (lymph) and returns it to the venous portion ofthe cardiovascular system. It drains most tissues with the exception of the nervous system and bone marrow.
A.Lymphatic capillaries are thin-walled vessels that begin as blind-ended channels (e.g., lacteals) adjacent to capillary beds where they collect lymph.
1.They are composed of a single layer of attenuated endothelial cells that lack fenestrae and fasciae occludentes. They possess a sparse basal lamina.
2.Lymph enters these leaky capillaries via spaces between overlapping endothelial cells.
3.Small lymphatic anchoring filaments between the surrounding connective tissue and the abluminal plasma membrane assist in maintaining luminal patency in these delicate vessels.
B.Large lymphatic vessels possess valves and are similar in structure to small veins, except that they have larger lumina and thinner walls.
1.Lymph nodes that filter the lymph are interposed along their routes.
2.These vessels converge to form the thoracic duct and right lymphatic duct. The thoracic duct empties into the venous system at the junction of the left internal jugular vein with the subclavian vein, whereas the right lymphatic duct empties into the venous system at a similar location on the right side of the neck.
CLINICAL
Edema is a pathologic process resulting in an increased volume of tissue
CONSIDERATIONS fluid.
Edema may be caused by venous obstruction or decreased venous blood flow (as in conges tive heart failure), increased capillary permeability (due to injury), starvation, excessive release of histamine, and obstruction of lymphatic vessels. It is common during pregnancy and in older persons. Edema that is responsive to localized pressure (i.e., depressions persist after release of pressure)
is called pitting edema. Edema can be a symptom of a serious underlying disorder, including heart disease; liver disease; or diseases of the thyroid, lymphatic system, or the kidneys, with serious consequences.


