

ECHO 2013 / Echocardiography in Acute Coronary Syndromes Management and Risk Assessment
.pdfMultifocal pneumonia due to aspiration superimposed ACS ????
•Echo
–Trivial anterior pericardial effusion
–Subtle inferior WMA
•No progression of ECG
•Trop remains elevated > four days later
–No typical ACS curve
•Myo-pericarditis ?
–Confirmed on cMR

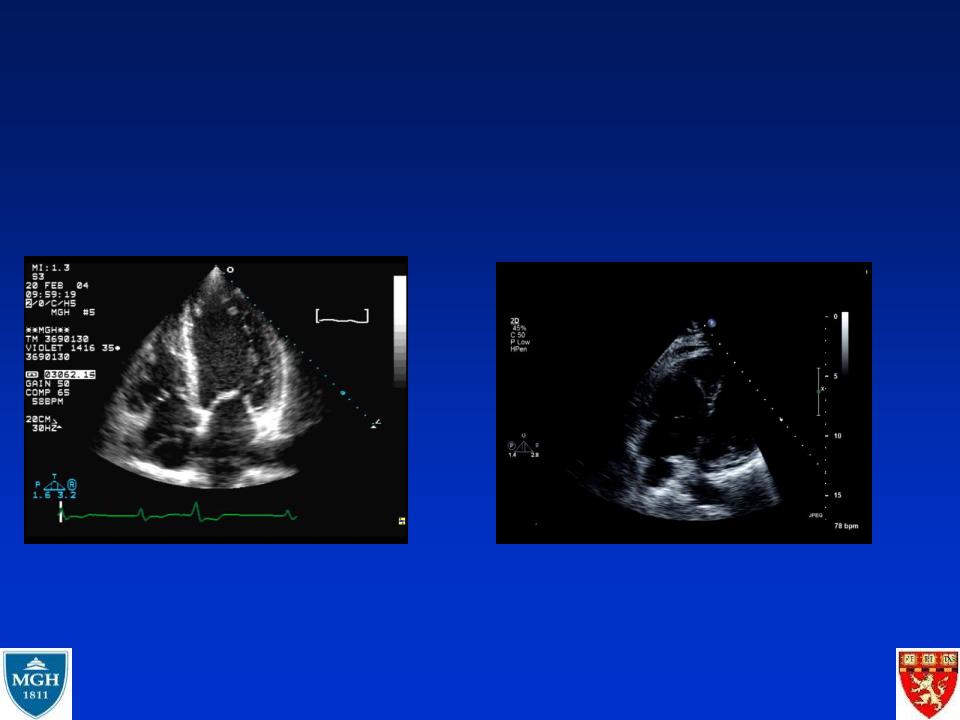
ACS and hypotension
•Differential diagnosis
–Poor LV function vs. Mechanical complications
•Prognostic echo markers
–LVEF, MR
•important across all age groups
SHOCK Trial: Kaplan-Meier survival based on independent effects of MR and LVEF and regardless of treatment strategy
PROPORTION ALIVE
1.0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0.9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0.8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0/1 MR, LVEF 28% |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
0.7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0.6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2/3/4 MR, LVEF 28% |
|
|
|
|
|
|
||||||
0.5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0/1 MR, LVEF<28% |
|
|
|
|
|
|
|
|
|
|
|||||
0.4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0.3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
0.2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2/3/4 MR, LVEF<28% |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
0.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0.0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
2 |
4 |
|
|
6 |
8 |
10 |
12 |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TIME FROM RANDOMIZATION (MONTHS) |
|
|
|
|
|
|
||||||||||
Picard MH et al, Circulation 2003;107:279-284
Echo to discriminate the differential
diagnosis: Hypotension, chest pain
Ant MI, LBBB |
Pulmonary embolism |

Chest pain, murmur, nonspecific STT wave
changes but echo shows it is not an MI
Aortic dissection

Not all WMA = ACS
•Stress cardiomyopathy (reversible)
–Takotsubo
•Myopericarditis (reversible)
•Old MI (not reversible)
•Chagas cardiomyopathy

What do the appropriate use criteria say ?
Douglas et al, JASE 2011;24:229-64 and JACC 2011;57:1126-66
•Myocardial Ischemia / Infarction with TTE
–Acute CP with suspected MI and non-diagnostic ECG when a resting echo can be performed during pain = APPROPRIATE
–Evaluation of a patient without chest pain but with other features of an ischemic equivalent or laboratory markers indicative of ongoing MI = APPROPRIATE
–Suspected complication of myocardial ischemia /infarction = APPROPRIATE
•Evaluation of Ventricular Function after ACS with TTE
–Initial evaluation of ventricular function following ACS = APPROPRIATE
–Re-evaluation of ventricular function following ACS during recovery phase when results will guide therapy = APPROPRIATE

Echocardiography in Acute
Coronary Syndromes:
should we image ? SOMETIMES
•To make the correct diagnosis
–Uninterpretable or non diagnostic ECG
–Confusing presentation
•Sorting out the differential diagnosis
–Immediate – no need to wait for the markers
•Assessing prognosis
–Early or later
•When things turn sour
–Assessing complications of CAD