ECHO 2013 / Echocardiography in Acute Coronary Syndromes Management and Risk Assessment
.pdfHas troponin replaced the echo ?
NOT ALWAYS !!
•Reperfusion therapy should not wait for the results of biomarkers
–Troponins rise 4 – 6 hrs after MI
•Sensitivity low in first 4 – 6 hrs
•Takes 3.5 hours after necrosis to be detectable
–Takes 6 – 9 hours to detect elevations in all MI pts
–Echo WMA is immediate
|
Onset |
Peak |
Duration |
|
|
|
|
|
|
CK |
3 – 12 hrs |
18 |
- 24 hrs |
36 - 48 hrs |
|
|
|
|
|
Troponin |
3 – 12 hrs |
18 |
– 24 hrs |
Up to 10 days |
|
|
|
|
|

High sensitivity Troponins will change the game
•Earlier detection
–Smaller quantities detected earlier
•However will need echo to assess functional significance of many of these positive tests
(low values)
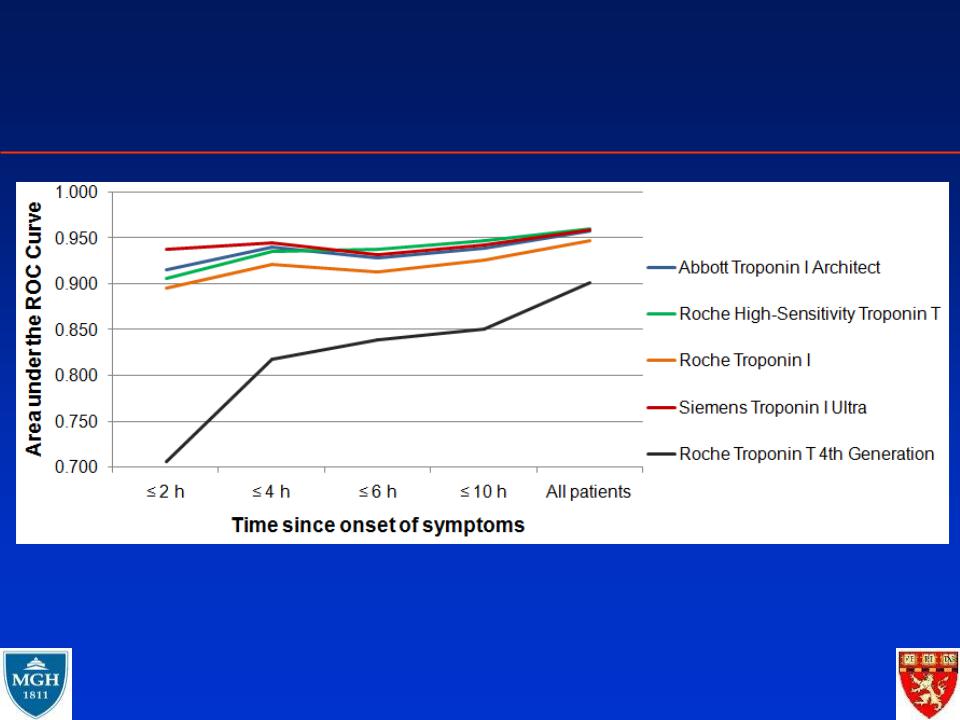
Sensitive Troponins improve the early
diagnosis of AMI (at presentation!)
Reichlin et al, NEJM 2009;361;858-867

Has troponin replaced the echo ?
•The spectrum of CAD
–Troponins don’t increase in myocardial ischemia
–echo can demonstrate ischemia
•Biomarkers poorly correlate with EF and RWMA
•Other things can increase Troponins
–Pulmonary embolism (RV)
–Myocarditis
–Renal insufficiency
•Troponin elevations commonly observed in patients with renal insufficiency who do not have clinical evidence of myocardial damage
–Echo has unique features in these scenarios

Non-ACS Situations of Troponin Elevation
• |
A real false positive |
• |
Myocarditis |
• |
Normal variants? |
• |
Pulmonary embolism |
• |
Pericarditis |
• |
Myocardial abscess |
• |
Severe illness |
• |
CHF and LVH |
|
– Sepsis |
• |
Arrhythmias and LVH |
• |
Blunt chest trauma |
• |
Idiopathic CMP |
• |
Radiofrequency |
• |
Chemotherapy or other |
|
ablation |
|
toxic/metabolic insults |
• |
DC Cardioversion |
• |
Cirrhosis |
• |
Transplant rejection |
• |
Renal failure |
• |
Aortic dissection |
|
|

Biomarkers and cardiac imaging are synergistic
•Biomarkers for typical MI diagnosis
–Echo when presentation confusing
–Echo when need to know LVEF, location or extent of LV dysfunction
•Echo for mechanical complications of MI or identifying etiology of hemodynamic compromise after MI

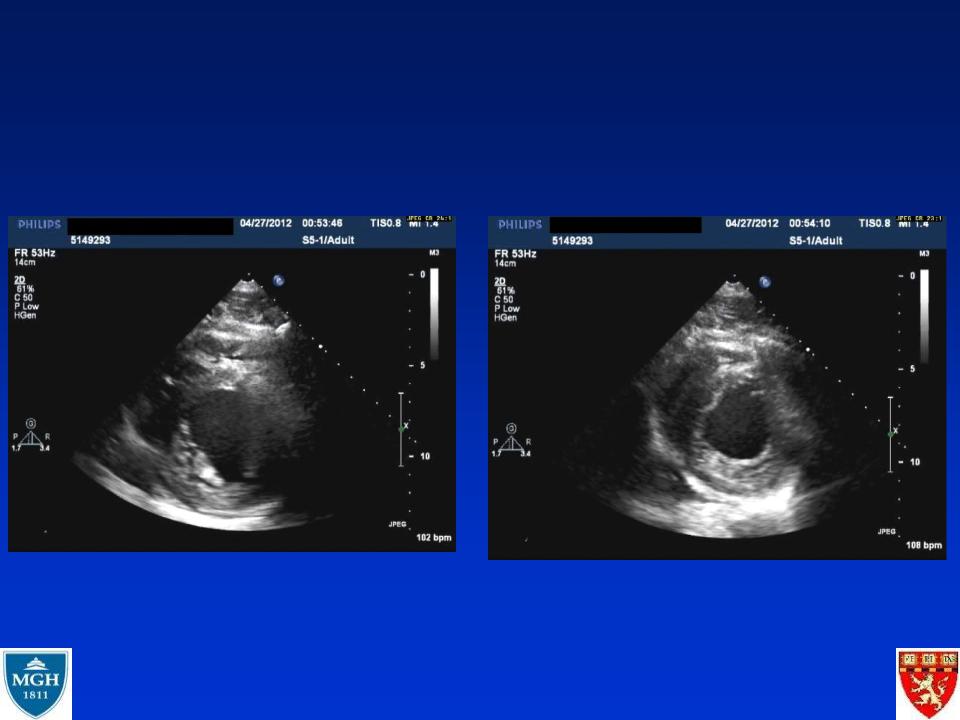
31 yo M with Troponin elevation is it an STEMI ?
•Previously healthy 31 yo M
•Transferred from prison with aspiration pneumonia
–RML cavitary lesion + abscess
–Drained with chest tubes
•Increasing dyspnea
–ECG (next page) “STE”
–Troponin 4.86
–No CP
•IS THIS AN MI ?