

ECHO 2013 / Echo and the Athlete’s heart
.pdfMore common cardiovascular pathologies and eligibility to participate in athletics

Case:
•18 year old during pre-sports screening with murmur noted, follow up ECG.

BC#36
•Athletes with probable or definitive clinical diagnosis of HCM should be precluded from most competitive sports, with possible exception of those of lowintensity regardless of phenotype or treatment/intervention.
•Athletes genotype (+), phenotype (-) with no cardiac symptoms or FH of SCD are not precluded, but are recommended to have frequent serial echo, EKG, Holter, exercise stress and CMR.
•Athletes with abnormal 12 lead ECG, with normal 2D echo, esp with FH(+) for HCM, should undergo CMR for regional LVH undetected by echo and delayed enhancement.
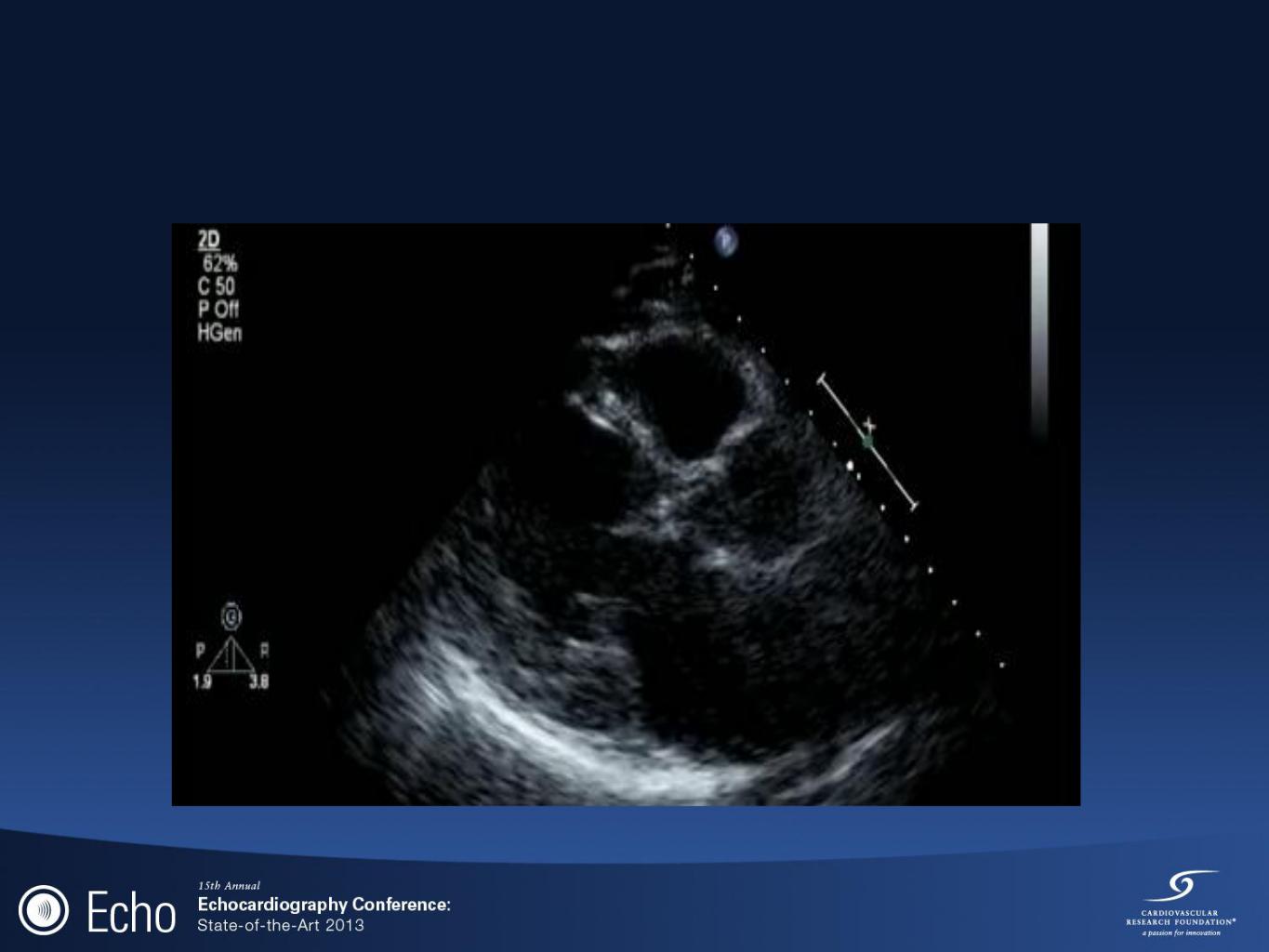
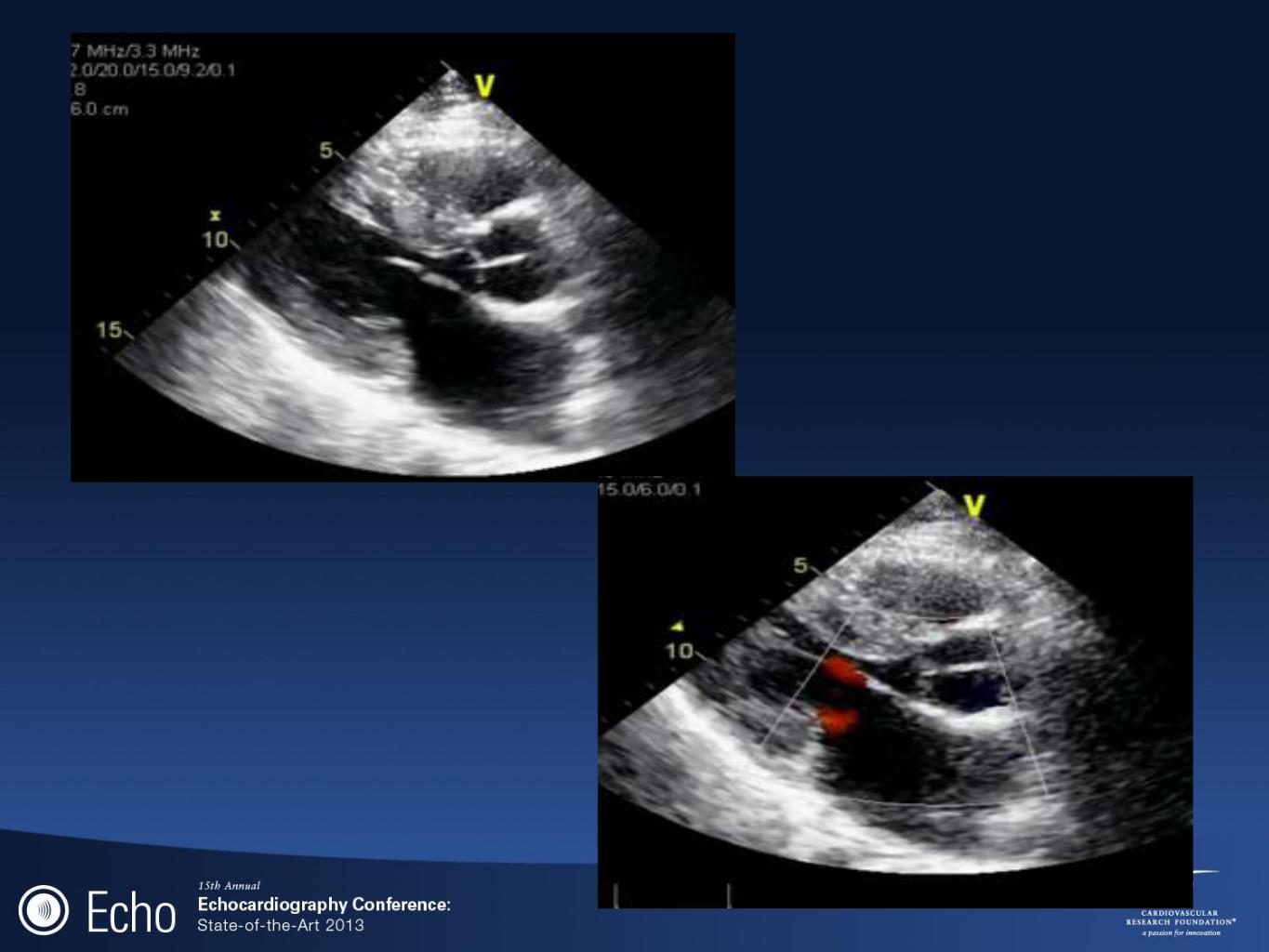
MVP
BC#36 recommendations
•Athletes with MVP and WITHOUT these features can compete in all competitive sports
•prior syncope due to arrhythmia
•sustained or repetitive and Nonsustained supraventricular and/or complex ventricular tachyarrhtyhmias on Holter
•severe MR
•LV EF <50%
•prior embolic event
•family history of MVP-related sudden death
•Athletes with MVP WITH any of above can compete in lowintensity competitive sports only

Summary
•Pre-participation History/physical exam/+/-ECG (12point AHA guideline)
•Echo findings of athlete’s heart-Eccentric/concentric hypertrophy, enlarged atria, RV enlargement, higher PA pressures, possibly LLN EF.
•Use of exercise echo/Doppler indices/CMR/detraining to differentiate between LVH and cardiomyopathy.
•Follow aortic roots >4.0cm. Compare with first, not just prior year.
•Bethesda Conference #36 recommendations
• Thank you
Cardiac physiology during exercise
•Increase cardiac output primarily due to increased SV, not HR
•?mechanism: early and rapid diastolic filling, increased diastolic volume, increased systolic contractility
•Increase in PASP in athletes during intense exercise >non-athletes
Bicuspid aortic valve