

Essentials of Orthopedic Surgery, third edition / 10-The Hand
.pdf10. The Hand |
407 |
Gout is a common metabolic illness in which uric acid forms crystals and accumulates in joints or soft tissues. Although it is most common in the first metatarsophalangeal (MTP) joint of the foot, it can occur in the joints and soft tissues of the hand. Often, it presents as a warm, tender, swollen, erythematous region and can mimic infection. Aspiration of a joint and visualization of negatively birefringent crystals under polarized light microscopy evaluation of the fluid confirms the diagnosis. The condition of severe tophaceous gout in the hands, which can cause extensive destruction of tendons or joints, is fairly uncommon because of improvements in medical management of this disease, but it still can be seen. Treatment options include rest, immobilization, antiinflammatory medications, corticosteroids, and other antigout medications. Surgery can sometimes be indicated for erosive tophi.
Calcium pyrophosphate dihydrate deposition disease is another metabolic problem in which crystals accumulate in joints and around tendons. This accumulation, too, can cause redness, swelling, and warmth over a joint, and again, aspiration and visualization of crystals in the fluid can be diagnostic for the problem. Treatment includes corticosteroid injections, nonsteroidal antiinflammatories, prednisone or colchicine for acute flareups, and surgery in severe cases.
Vascular
Arterial occlusions and small vessel disease in the hand can cause severe problems with pain and, occasionally, necrosis of the fingers. Although uncommon, ulnar artery occlusions, which usually occur at the level of the hamate hook, can cause significant ulnar nerve symptoms as well as diminished flow to the digits. When this occurs after a repetitive trauma situation, it is called hypothenar hammer syndrome, and it is seen in manual laborers who use their hypothenar eminence as a hammer on the objects with which they are working. A diagnosis for this can be made at times with ultrasound but an angiogram is usually required. The treatment involves decompression of the nerve and artery and reconstruction or ligation of the thrombosed segment of the artery. Thrombosis of digital arteries is sometimes seen in patients with atherosclerotic disease proximally, but it is quite uncommon.
Vascular deficiencies secondary to other underlying diseases can be a significant problem in the hand, particularly in diabetes and scleroderma. Many of these patients go on to require amputations of digits, but in earlier stages of scleroderma, a digital sympathetectomy or removal of the vascular adventitia can decrease the amount of spasm that occurs and limit the damage to the digits.
Patients who have severe loss of flow to the hands can also develop gangrene of the digits. This condition is particularly common in patients who go into systemic vascular shock and require vasopressors, which restrict flow to the extremities. Once again, many of these patients develop gangrene of the digits and require formal amputations later.

408 M.A. Haque
True aneurysms of the wrist and hand are relatively uncommon. Usually occurring in the ulnar artery, they cause symptoms very similar to hypothenar hammer syndrome and can be treated the same way. Pseudoaneurysms are more common and can occur anywhere in the hand as the result of trauma to an artery. They are usually treated by ligating or reconstructing the artery involved.
Neoplasms
Skin Cancer
Skin cancers (squamous cell and basal cell carcinomas, and melanoma) are relatively common, especially in the elderly or those with predisposing factors. These factors include prolonged exposure to the sun in farmers and other outdoor workers, and excessive exposure to X-rays, arsenicals, or other chemicals (Fig. 10-6A). Squamous and basal cell carcinomas can usually be cured by wide excision if they have not already metastasized. Melanomas are much more unpredictable in their behavior and need to be addressed quickly (Fig. 10-6B).
Other Soft Tissue Masses
Benign soft tissue masses are very common in the hand and wrist. They can arise in any of the tissues making up the hand including nerves, vessels, fat, and fascia. The most common “tumors” of the hand arise from the synovium and include ganglions, mucous cysts, and giant cell tumors of the tendon sheath. Ganglia occur in four locations: on the dorsum of the wrist, on the volar aspect of the wrist adjacent to the radial artery, in the flexor tendon sheath at the base of the finger, and over the dorsum of the DIP joint (mucous cyst), usually associated with osteoarthritis and osteophyte formation of the joint. A ganglion on the dorsum of the wrist or over the flexor tendon sheath can be aspirated, although rates of recurrence are fairly high.
Aspiration of a volar wrist ganglion should be approached cautiously, if at all, because of the proximity of the radial artery. Surgical resection is a more definitive option, with only 5% to 10% recurrence rates when done correctly. Arthroscopic resection is now available for dorsal wrist ganglia. Giant cell tumors of the tendon sheath are solid lesions arising from the synovium of the tendon sheath or from the finger joints. Simple excision is usually curative, although occasional recurrences are seen.
Other common benign soft tissue masses include foreign-body granulomas, epidermal inclusion cysts, arteriovenous malformations and hemangiomas, neurilemmoma, and glomus tumors.
Malignant soft tissue tumors in the hand are very rare aside from skin cancers. The most common ones are epithelioid sarcomas, synovial cell sarcomas, and malignant fibrous histiocytoma. Delay in diagnosis is a common problem to these tumors. Limb salvage surgery is the treatment of choice whenever possible.

10. The Hand |
409 |
A
B C
FIGURE 10-6. Neoplasms of the hand. (A) Squamous cell carcinoma of finger in patient with 30-year history of holding children being radiographed. Note atrophic skin changes (arrow) from the radiation exposure. (B) Subungual melanoma with splitting of the nail from involvement of nail bed. (C) Enchondroma of proximal phalanx with expansion of the diaphysis. Note the enchondroma of the metacarpal with callus from a healed pathologic fracture.
Tumors of Bone
Benign tumors of the hand bones are often diagnosed incidentally on radiographic examination for trauma. The most common is the enchondroma (see Fig. 10-6C). Treatment is not required unless pathologic

410 M.A. Haque
fracture through the lesion has occurred or is impending. Simple curettage, with or without bone grafting, often suffices. Osteochondromas, fibrous dysplasia, and giant cell tumor of bone can also present in the small hand bones and may require surgery for diagnosis or treatment. Malignant tumors of the hand skeleton are very rare. Partial or total hand amputation may be required along with adjuvant radiation therapy or chemotherapy. Metastatic tumors of the hand seldom occur as isolated metastases but are not uncommon during widespread metastatic disease, especially from lung or breast lesions.
Management Protocols
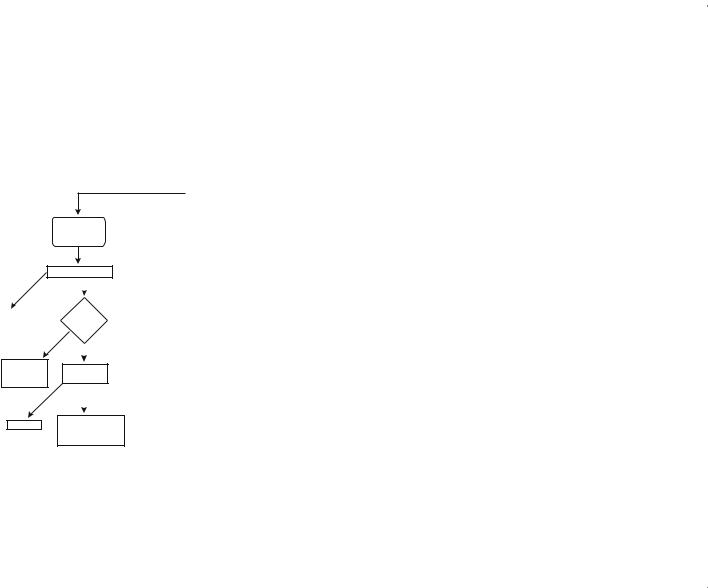
As one can see, a broad variety of complex problems can affect the hand and wrist. It is, therefore, important to have in mind a standardized approach to patients with these problems to help arrive at the correct diagnosis and management options. The physician should start with a careful and detailed history of the chief complaint, then with a differential diagnosis in mind should perform a directed but thorough physical examination. Plain radiographs are usually, but not always, indicated. We have developed algorithms beyond this to help streamline a patient’s care and avoid missing important diagnoses. Although the algorithms are overall quite complete, one should be wary of unusual presentations or diagnoses that are not included. These rare occurrences may require further evaluation or consultation by a hand specialist. The algorithms divide patients into groups with or without a specific history of injury (Figs. 10-7, 10-8).
Nearly all patients with a specific injury should be X-rayed. If the initial radiographs show a fracture, dislocation, or carpal instability pattern, appropriate operative or nonoperative treatment should be initiated. When X-rays are negative, a soft tissue injury may have occurred or an occult fracture may be present. When a specific soft tissue injury is noted, appropriate treatment should be initiated. If none is found and the patient’s symptoms cannot be explained, either further imaging should be performed or splinting or casting for a period of time followed by reevaluation should be considered.
Figure 10-8 concerns patients who have had no specific history of trauma or injury. Unless patients have a very classic history and physical examination for a soft tissue process, plain X-rays should be taken. If they are positive for arthritis, tumor, or occult bony injury, appropriate operative or nonoperative management should be undertaken. If they are negative, further evaluation or indicated treatment should be initiated according to the algorithm.
Negative |
Negative |
Negative |
Negative |
Negative |
Positive |
Positive |
Tender Over
Scapholunate
Interval
|
|
|
Scaphoid Shift Test |
|||
Pos |
itive |
|
|
|
Negative |
|
|
|
|
||||
|
|
|
MRF |
|||
|
|
|
|
|||
Treat for |
|
|
||||
|
|
Arthrogram |
||||
Carpal |
|
|
||||
|
|
|
|
|||
Instability |
|
Positive |
|
|
||
|
|
|
|
Negative |
||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|
||
Treat for |
|
|
|
|
||
|
|
Corticosteroid |
||||
Ligament |
|
|||||
|
injection |
|||||
Tear |
rovement |
|||||
|
Recurrence |
|||||
|
|
|
|
|
||
|
Imp |
|
|
|
or |
|
|
|
|
|
No Improvement |
||
Observer |
|
|
Arthroscopic or |
|||
|
|
|
|
|||
Open Treatment for
Occult Ganglion
FIGURE 10-7. Management algorithm for hand and wrist pain with history of acute injury.
Hand The .10
411

Haque .A.M 412
FIGURE 10-8. Management algorithm for hand and wrist pain with no history of injury.

10. The Hand |
413 |
Suggested Readings
Green DP, Hotchkiss RN, Peterson WC (eds) Green’s Operative Hand Surgery. New York: Churchill Livingstone, 1999.
Seiler JG (ed) Essentials of Hand Surgery. American Society for Surgery of the Hand, Chicago, IL, 2002.
Trumbull TE (ed) Hand Surgery Update III. American Society for Surgery of the Hand, Chicago, IL, 2003.
Questions
Note: Answers are provided at the end of the book before the index.
10-1. Which of the following is a particularly uncommon malignancy in the hand?
a.Epithelioid sarcoma
b.Squamous cell carcinoma
c.Malignant fibrous histiocytoma
d.Isolated metastatic prostate carcinoma
e.Synovial cell sarcoma
10-2. Which of the following conditions can be causative factors in carpal tunnel syndrome?
a.Renal failure
b.Pregnancy
c.Hypothyroidism
d.Diabetes
e.All the above
10-3. Which of the following congenital hand differences is associated with visceral anomalies?
a.Syndactyly
b.Radial clubhand
c.Phocomelia
d.Mirror hand
e.Occasional constriction band syndrome
10-4. Which of the following joints is usually spared in osteoarthritis?
a.Metacarpophalangeal joints of the fingers
b.Thumb carpometacarpal joint
c.Distalinterphalangeal joints of the fingers
d.Proximal interphalangeal joints of the fingers
e.None of the above
10-5. A positive Finkelstein’s test suggests which of the following diagnoses?
a.Trigger thumb
b.Thumb carpometacarpal arthritis
c.Scaphotrapeziotrapezoid arthritis
d.de Quervain’s tenosynovitis
e.Carpal tunnel syndrome

414 M.A. Haque
10-6. Which of the following is not a common symptom in carpal tunnel syndrome?
a.Night pain
b.Loss of dexterity
c.Numbness localized to the small finger
d.Global numbness in the hand
e.Weakness of the hand
10-7. When evaluating an open wound in the emergency room, a physician should:
a.Appropriately numb the hand and wrist before further evaluation
b.Explore the wound directly
c.Clamp off any large blood vessels that are clearly cut
d.Cover the wound with a clean sterile dressing and avoid further probing
e.Avoid documentation of injury until definitive management in the Operating Room
10-8. Which of the following bacteria must be covered when a human bite wound is involved?
a.Mycobacterium avium-intracellulare
b.Staphylococcus aureus
c.Borrelia burgdorferi
d.Eikenella corrodens
e.b and d
10-9. Scaphoid fractures are commonly associated with:
a.Anatomic snuff box tenderness
b.Nonunions
c.Avascular necrosis
d.Delays in diagnosis
e.All the above
10-10. Which of the following is not a common finding in infectious flexor tenosynovitis?
a.Fusiform swelling
b.Semiflexed posture of the digit
c.Destructive bone erosions on plain X-ray
d.Tenderness over the flexor tendon sheath
e.Severe pain with passive extension of the digit
10-11. A Stener lesion is associated with which of the following diagnoses?
a.Trigger thumb
b.Deep space infection of the hand
c.de Quervain’s tenosynovitis
d.Gamekeeper’s thumb
e.Extensor tendon rupture