

Old sins
Like all of medicine, psychiatry’s history includes what now appear dangerous and even barbaric treatments. Before being too critical think what it must have been to live at a time when early and sudden death was a constant threat and excruciating pain had to be endured, often for weeks and months on end. There were few certainties and even fewer effective treatments. What doctors were willing to do two centuries ago, and what patients were prepared to endure, have to be judged against quite different standards. Folk treatment of the mad was also far from gentle, despite our tendency to romanticize pre-industrial societies. Disabled individuals were often accepted and occasionally revered but the more disturbed were often excluded (which could mean death) or mistreated as witches or such like.
Early psychiatrists used the standard medical treatments of their time including bleeding, purging, and cupping (attaching hot cups to the back to ‘draw out’ toxins). The early asylums moved away from these, emphasizing moral treatments (Chapter 2), although various desperate measures were tried to calm ‘furiously’ agitated patients. These included cold baths (still used well into the 20th century) and a series of ingenious devices which worked by simply exhausting the patient, such as the notorious ‘whirling chair’. However, the major sins of the asylum era were those of neglect – restraint rather than attention, undignified and humiliating conditions rather than active abuse.
Long-term fluctuating illnesses are particularly prone to accumulate far-fetched theories and treatments. This is a mixture of desperation and pure chance (an illness may simply recover just when some irrelevant treatment is being used). There was a vogue for removing otherwise healthy organs in the mentally ill in the late 19th century because they were thought to be the site of ‘sepsis’ (low grade infection). Thousands of healthy teeth and tonsils were removed and even large parts of the bowel. In Trenton State Hospital, New Jersey, Dr Henry Cotton championed this approach right up until his death in 1933 (including taking out all the teeth from his own two sons and even subjecting one to an abdominal operation). These treatments were controversial but still supported by distinguished psychiatric figures.
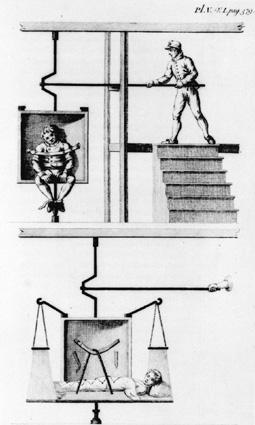
12. Whirling chair: one of the many devices developed to ‘calm’ overexcited patients by exhausting them
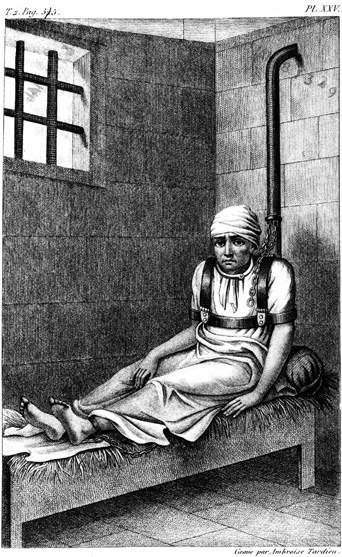
13. William Norris chained in Bedlam, in 1814 The Hawthorn effect
A complicating factor is that the fuss and attention surrounding treatments can make a real difference even if the treatment itself is ineffective. This was shown with insulin coma treatment. Insulin had been long used in psychiatry to stimulate appetite and calm agitated patients (who could otherwise literally starve to death). A course of insulin comas was believed to be effective in schizophrenia and this became a common treatment from the 1930s through to the 1960s. It was a potentially dangerous treatment requiring skilled and attentive nursing – if the coma went too deep the patient could die. It was the first psychiatric treatment subject to a controlled trial to establish its effect. Half the patients were put into a light sleep using tranquillizers and half into an insulin coma, without the staff knowing which was which. The results were the same for both groups, forcing the conclusion that it was the nursing attention and hope inspired by the treatment that made the difference, not the insulin. The treatment was abandoned. This effect is known as the ‘Hawthorn’ effect and psychiatric research always has to account for enthusiasm.
Enthusiasm shouldn’t be written off in psychiatry. Much of medicine may be best conducted in a dispassionate, scientific frame of mind but psychiatry requires hope and optimism from its staff. Patients have so often lost hope and need help regaining it. Hope is therapeutic in its own right as the insulin coma study indicated. Many studies have confirmed that optimism makes a difference to outcome (even in cancer patients). It can, however, lead to over-enthusiasm and treatments, including effective treatments, being given well beyond their indications.