

Gale Encyclopedia of Genetic Disorder / Gale Encyclopedia of Genetic Disorders, Two Volume Set - Volume 1 - A-L - I
.pdfIn Kallmann syndrome, the olfactory neurons are unable to grow into the brain. Hence, the GnRH cells can not follow their pathway. As a result, the olfactory bulb does not form, resulting in the inability to smell. The GnRH cells can not follow the pathway of the axons and do not reach their final destination in the hypothalamus. Hence, no GnRH is made to stimulate the pituitary to make FSH and LH, resulting in hypogonadotropic hypogonadism.
In X-linked recessive KS, the KAL gene instructs the body to make the protein anosmin-1. This protein is involved in providing the pathway in the brain for which the olfactory axons grow. If it is altered in any way, the axons will not know where to grow in the brain and the GnRH cells will be unable to follow. The protein anos- min-1 is also found in other parts of the body, possibly explaining some of the other symptoms sometimes seen in Kallmann syndrome.
Other features
The features of Kallmann syndrome can vary among affected individuals even within the same family. The two features most often associated with Kallmann syndrome are HH and the inability to smell. Males can also have a small penis and undescended testicles at birth (testicles are still in body and have not dropped down into the scrotal sac). Clubfoot, cleft lip and/or cleft palate can also be present at birth. Clubfoot occurs when one or both feet are not properly placed onto the legs and can appear turned. Cleft lip and/or cleft palate occur when the upper lip and/or the roof of the mouth fail to come together during development. Kidney abnormalities, most often unilateral renal agenesis (one kidney did not form) are especially common in those males with X-linked recessive KS. Choanal atresia (pathway from the nose is blocked at birth) and structural heart defects have also been seen in KS.
Central nervous system problems can also occur in Kallmann syndrome. These can include nystagmus (involuntary eye movement), ataxia (involuntary body movement), hearing loss and problems with vision. Synkinesia is especially common in men with the X- linked recessive form of KS. Some people with KS are also mentally retarded. Holoprosencephaly, when the brain fails to develop in two halves, can also be seen in some individuals with KS.
Diagnosis
Individuals with Kallmann syndrome are usually diagnosed when they do not undergo puberty. Hormone testing shows that both LH and FSH are decreased.
Affected individuals often do not realize they cannot smell. MRI can often detect the absence of the olfactory bulb in the brain. Renal ultrasound can determine if a kidney is missing.
As of 2001, genetic testing for alterations in the KAL gene is the only genetic testing available. Even with families with clear X-linked recessive inheritance, genetic testing does not always detect an alteration in the KAL gene. Hence, diagnosis is still very dependent upon clinical features.
Treatment and management
When a child with KS is born with structural abnormalities such as cleft lip and/or palate, clubfoot or heart defects, surgery is often required to fix the defect. Taking sex hormones treats delayed puberty; women take estrogen and men take testosterone. Once puberty is completed, taking GnRH or both LH and FSH can treat hypogonadism. For most affected individuals, treatment is successful and infertility is reversed. However, a small portion of people will not respond to treatment.
When an isolated case of Kallmann syndrome is diagnosed, evaluation of first-degree family members, such as parents and siblings, should be completed. This should include a detailed family history, measuring hormone levels, assessing sense of smell, and renal ultrasound to look for kidney abnormalities. This information may help to diagnosis previously unrecognized cases of Kallmann syndrome. Furthermore, this information may be important for genetic counseling and determining whom in the family is at risk for also having Kallmann syndrome.
Prognosis
For individuals with the most common features of Kallmann syndrome, hypogonadism and the inability to smell, prognosis is excellent. In most cases, hormone treatment is able to reverse the delayed puberty and hypogonadism. For those individuals with other symptoms of Kallmann syndrome, prognosis can depend on how severe the defect is. For example, structural heart defects can be quite complex and sometimes surgery can not fix them. Furthermore, no treatment is available for the mental retardation in the portion of affected individuals with this symptom.
Resources
PERIODICALS
Rugarli, Elena, and Andrea Ballabio. “Kallmann Syndrome: From Genetics to Neurobiology.” JAMA 270, no. 22 (December 8, 1993): 2713–2716.
syndrome Kallmann
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
629 |

Kartagener syndrome
ORGANIZATIONS
American Society for Reproductive Medicine. 1209 Montgomery Highway, Birmingham, AL 35216-2809. (205) 978-5000. http://www.asrm.com .
RESOLVE, The National Infertility Association. 1310 Broadway, Somerville, MA 02144-1779. (617) 623-0744. resolveinc@aol.com. http://www.resolve.org .
WEBSITES
Pediatric Database (PEDBASE) www.icondata.com/health/ pedbase/files/KALLMANN.HTM .
Carin Lea Beltz, MS
I Kartagener syndrome
Definition
Kartagener (pronounced KART-agayner) syndrome refers to a condition that involves difficulty with clearing mucus secretions from the respiratory tract, male infertility, and situs inversus. The defining characteristic of this syndrome is the situs inversus, which is a reversal of abdominal and thoracic organs.
Description
This syndrome is named after Kartagener, a physician from Switzerland. In the 1930’s, Kartagener and a colleague described a familial form of bronchiectasis with situs inversus and nasal polyps. This came to be known as Kartagener syndrome. Kartagener syndrome is also known as the Siewert syndrome, after another physician, Siewert, who described the syndrome in the early 1900’s.
Individuals who have Kartagener syndrome form a subset of the disorder called primary ciliary dyskinesia. Originally, primary ciliary dyskinesia was known as immotile cilia syndrome. The name, immotile cilia syndrome, is no longer used since the discovery that the cilia are actually not immotile, but rather, abnormal in movement. Individuals who have Kartagener syndrome, basically have primary ciliary dyskinesia, plus partial or complete situs inversus. The situs inversus is what sets Kartagener syndrome apart from primary ciliary dyskinesia.
Kartagener syndrome is caused by abnormalities of the cilia that line the respiratory tract and also form the flagella of sperm. Cilia are tiny hair-like structures that contain a bundle of small parallel tubes that form a central core. This core is called the axoneme. Ciliary movement is accomplished by the bending of the axoneme. One of the most important associated structures that
enable ciliary movement to occur are sets of tiny arms that project from each tubule. These tiny arms are called dynein arms.
Cilia line the cells of the lungs, nose and sinuses. Before reaching the lungs, air travels through the airway where it is moistened and filtered. The nasal passages and airway are lined with mucus membranes. The mucus covering the mucus membrane traps dirt and other foreign particles that have been breathed in. The cilia, lining the membranes, beat in a wavelike manner moving the layer of mucus and carrying away the dirt and debris that has been trapped. This mucus can then be coughed out or swallowed into the stomach.
In Kartagener syndrome, the cilia do not move, move very little, or move abnormally. Because the cilia do not function properly, the mucus is not cleared from the respiratory tract, which leads to sinus infection (sinusitis) and chronic changes of the lung (bronchiectasis), which make it difficult to exhale. Mucus clearance from the middle ear can also be affected and over time can lead to hearing loss.
The male infertility in Kartagener syndrome is also caused by abnormal cilia movement. One spermatozoon consists of a head, midpiece, and a tail or flagellum. The tail of a spermatozoon is a long flagellum consisting of a central axoneme. This axoneme enables the movement of the flagellum so that the spermatozoon can propel its way to the fallopian tube and burrow through the egg coat to fertilize the egg. In Kartagener syndrome, these cilia are either immotile, or are not able to move normally to complete the journey to the fallopian tubes, nor may they be able to burrow through the egg coat. This results in male infertility.
As stated above, situs inversus is what sets Kartagener syndrome apart from primary ciliary dyskinesia. Complete situs inversus involves reversal of both the abdominal and thoracic organs so that they form a mirror image of normal. In partial situs inversus, the thoracic organs may be reversed, while the abdominal organs are normally positioned, or vice versa. Approximately one in 10,000 adults have situs inversus. Only about 20% of individuals who have complete situs inversus are diagnosed to have Kartagener syndrome. Of those with complete situs inversus who are diagnosed to have Kartagener syndrome, there is only a small risk for associated cardiac defects. Partial situs inversus may occur in individuals who have Kartagener syndrome as well. Partial situs inversus has a higher association with other abnormalities, including polysplenia or asplenia (extra or absent spleen) and cardiac defects.
One theory behind the association of situs inversus with the underlying cause of Kartagener syndrome is that the lack of ciliary movement in the developing embryo
630 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
may result in incorrect organ rotation in approximately 50% of affected individuals. In fact, 50% of patients with PCD will have situs inversus and thus be diagnosed to have Kartagener syndrome. However, this is a theory supported only by some researchers.
Genetic profile
Kartagener syndrome is an autosomal recessive condition. This means that in order to have the condition, an individual needs to inherit two copies of the gene for the condition, one from each parent. Individuals who carry only one gene for an autosomal recessive syndrome are called heterozygotes. Heterozygotes for Kartagener syndrome have normal ciliary function and do not have any clinical features of the condition. If two carriers of Kartagener syndrome have children, there is a 25% chance, with each pregnancy, for having a child with Kartagener syndrome.
The components that form the cilium contain several hundred different proteins. Each is coded for by different DNA sequences, potentially on different chromosomes. A defect in any of these codes could produce an abnormal or missing protein that is a building block for the cilium and thus could cause abnormal ciliary structure and movement, resulting in Kartagener syndrome.
When the same condition can be caused by different genetic abnormalities, this is known as genetic heterogeneity. In fact, several different defects in cilia have been seen in association with Kartagener syndrome, including; overly long cilia, overly short cilia, absent cilia and randomly oriented cilia, suggesting genetic heterogeneity. Studies have suggested that the most common defect of cilia in Kartagener syndrome is the lack of dynein arms. There have been rare cases in which individuals have Kartagener syndrome, yet have no detectable abnormality of the cilia, even though the ciliary function is abnormal. Results of one study involving a genome-wide linkage search performed on 31 families, with multiple individuals affected with either PCD or Kartagener syndrome, strongly suggested extensive heterogeneity. Potential regions involving genes responsible for PCD or Kartagener syndrome were localized on chromosomes 3, 4, 5, 7, 8, 10, 11, 13, 15, 16, 17 and 19.
Demographics
Kartagener syndrome occurs in approximately one in 32,000 live births, which is half the incidence of primary ciliary dyskinesia (one in 16,000 live births). Kartagener syndrome is not found more commonly in any particular sex, ethnic background or geographic region. Males, however, may be diagnosed more often than females because of infertility investigation.
K E Y T E R M S
Bronchiectasis—An abnormal condition of the bronchial tree, characterized by irreversible widening and destruction of the bronchial walls of the lungs.
Cystic fibrosis—A respiratory disease characterized by chronic lung disease, pancreatic insufficiency and an average age of survival of 20 years. Cystic fibrosis is caused by mutations in a gene on chromosome 7 that encodes a transmembrane receptor.
Dyskinesia—Impaired ability to make voluntary movements.
Tympanoplasty—Any of several operations on the eardrum or small bones of the middle ear, to restore or improve hearing in patients with conductive hearing loss.
Signs and symptoms
Newborns who have Kartagener syndrome may present with neonatal respiratory distress. Often when individuals are diagnosed to have Kartagener syndrome in later childhood, problems such as neonatal respiratory distress may be identified in their history. Symptoms that may present in childhood include; recurrent ear infections (otitis media) that can lead to hearing loss, chronic productive cough, reactive airway disease, pneumonia, chronic bronchitis, runny nose (rhinitis) with a thin discharge, and sinus infection (sinusitis). Situs inversus usually does not present symptomatically, unless it is associated with a congenital heart defect.
The most common clinical expression of Kartagener syndrome in adults includes chronic upper and lower airway disease presenting as sinusitis and bronchiectasis. Clubbing of the digits (fingers) may occur as the result of chronic hypoxia (lack of oxygen) from bronchiectasis. In males of reproductive age, male infertility is almost universal. In females who have Kartagener syndrome, infertility is not usually a characteristic. This suggests that the egg transport down the fallopian tube is associated more with muscle contractions than with ciliary movement.
Several other conditions should be considered when the aforementioned symptoms present, including; Cystic fibrosis (CF), immune deficiencies and severe allergies. Although the causes of Kartagener syndrome and CF are completely different, the symptoms of these two diseases
syndrome Kartagener
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
631 |
Kartagener syndrome
are very similar. Often when the symptoms present, children with Kartagener syndrome are tested for CF first because the incidence of CF is much higher (one in 2,400) than the incidence of Kartagener syndrome. CF is also associated with male infertility.
Diagnosis
Diagnosis of Kartagener syndrome is confirmed by identifying the ciliary abnormalities of structure and movement. This is accomplished by biopsy of the mucus membranes of the respiratory tract and/or by examination of sperm, looking for ciliary dyskinesia. Situs inversus can be identified by x ray or ultrasound examination. Infertility investigation may elicit the possibility of Kartagener syndrome in a patient previously undiagnosed. After a diagnosis is made, genetic counseling should be provided to discuss the inheritance pattern, to help identify other possible affected family members and to discuss reproductive options.
As Kartagener syndrome is an autosomal recessive disorder, individuals who have had a child with Kartagener syndrome have a 25% chance, with each future pregnancy, of having another child with Kartagener syndrome. Prenatal diagnosis may be possible for a couple with a previously affected child, by performing ultrasound examination to identify a fetus who has situs inversus. Although, if the fetus does not exhibit situs inversus, it is still possible for the fetus to have PCD. Also, it is important to remember that identifying a fetus who has situs inversus in a family not known to be at an increased risk for Kartagener syndrome, does not mean that the fetus has Kartagener syndrome as only 20% of individuals who have situs inversus have Kartagener syndrome. As of January 2001, DNA testing for Kartagener syndrome is not possible.
Treatment and management
Treatment for Kartagener syndrome involves treatment of the symptoms. Treatment for sinusitis includes the use of antibiotics to treat and prevent recurrent infection. Occasionally, surgery to relieve the sinusitis and remove nasal polyps that may be present is necessary. Daily chest physiotherapy to loosen mucus secretions is a common therapy as well, and if started early in life can help to prevent or delay development of bronchiectasis. Tympanoplasty in children with recurrent ear infections is often necessary.
Advances in reproductive technology allow for men who have Kartagener syndrome to have the opportunity to have children. A procedure called intracytoplasmic sperm injection or ICSI, now allow immotile or dys-
motile sperm to fertilize an egg. ICSI involves injection of a single sperm into single eggs in order for fertilization to occur. This procedure first involves ovulation induction and egg retrieval to obtain eggs for attempt at fertilization by ICSI. In Vitro Fertilization (ICSI) pregnancy rates vary from center to center. Overall pregnancy rates of 10%-40% have been quoted worldwide, utilizing these procedures.
The chance for an affected male and his unaffected partner to have a child who has Kartagener syndrome is small. If the disease incidence is one in 32,000, then the chance for the unaffected woman to be a carrier of Kartagener syndrome is approximately one in 100 and the chance for having an affected child would be expected to be approximately one in 200 (0.5%). However, all children of affected males or females will be carriers for Kartagener syndrome.
Prognosis
The severity of Kartagener syndrome is variable. With the advent of antibiotic use for infection control, the life expectancy of a patient with Kartagener syndrome is close to or within the normal range, if there are no immediate problems in the newborn period.
Resources
BOOKS
Jones, Kenneth Lyons. Smith’s Recognizable Patterns of
Human Malformation. Philadelphia: W.B.Saunders
Company, 1997.
PERIODICALS
Guichard, Cècile, et al. “Axonemal Dynein Intermediate-Chain Gene (DNAI1) Mutations Result in Situs Inversus and Primary Ciliary Dyskinesia (Kartagener Syndrome).”
American Journal of Human Genetics (April 2001): 1030.
ORGANIZATIONS
American Lung Association. 1740 Broadway, New York, NY 10019-4374. (212) 315-8700 or (800) 586-4872.http;//www.lungusa.org .
National Organization for Rare Disorders (NORD). PO Box 8923, New Fairfield, CT 06812-8923. (203) 746-6518 or (800) 999-6673. Fax: (203) 746-6481. http://www
.rarediseases.org .
WEBSITES
OMIM Online Mendelian Inheritance in Man. Entries 244400
and 242650. http://www.ncbi.nlm.nih.gov/entrez/query
.fcgi?db OMIM .
Tucker, Michael. “Clinical In Vitro Fertilization and Culture”.
IVF.com. http://www.ivf.com/insem.html .
Renee A. Laux, MS
632 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
I Karyotype
Definition
Karyotype refers to the arrangement of chromosomes in their matched (homologous) pairs. For the purposes of this definition, we will be referring to human chromosomes, although there is a karyotype characteristic for each species. The human chromosomes are arranged and numbered according to the International System for Human Cytogenetic Nomenclature (ISCN). The most recent recommendations of the ISCN are from 1995. Karyotype either refers to the actual composition of the chromosomes in a body cell of an individual or species, or to the actual diagram or photograph of those chromosomes, arranged in their pairs.
Description
The normal human karyotype consists of 23 pairs of chromosomes. There are 22 pair of autosomes, which are the chromosomes that are not the sex chromosomes. The genes on these chromosomes instruct our bodies as to how they look and function. The 23rd pair of chromosomes are the sex chromosomes. Typically, females have two X sex chromosomes and males have one X sex chromosome and one Y sex chromosome.
Karyotype construction
In the construction of the karyotype, the chromosomes are numbered 1 to 22 from longest to shortest. The last pair are the sex chromosomes and are placed on the karyotype after the 22nd pair. The chromosomes can be separated into groups, based on their length and the position of the centromere. Group A consists of chromosome pairs 1, 2 and 3. They are the longest chromosomes and their centromeres are in the center of the chromosomes (metacentric). Group B consists of chromosome pairs 4 and 5. They are long; however, their centromeres lie toward the top of the chromosomes (submetacentric). Group C consists of chromosome pairs 6, 7, 8, 9, 10, 11 and 12 and also includes the X chromosome. They are medium-sized and their centromeres either lie in the middle or toward the top of the chromosomes. Group D consists of chromosome pairs 13,14 and 15. They are medium-sized and their centromeres lie at the top of the chromosomes (acrocentric). Additionally, the D group chromosomes have satellites. Group E consists of chromosome pairs 16, 17 and 18. They are relatively short chromosomes and their centromeres lie in the center or towards the top of the chromosomes. Group F consists of chromosomes 19 and 20. They are short chromosomes with centromeres that lie in the center of the chromo-
K E Y T E R M S
Acrocentric—A chromosome with the centromere positioned at the top end.
Centromere—The centromere is the constricted region of a chromosome. It performs certain functions during cell division.
Homologous chromosomes—Homologous chromosomes are two chromosomes of a doublet set that are identical, particularly for the genes that are on them.
Metacentric—When a chromosome has the centromere in the middle of the chromosome it is called a metacentric chromosome.
Satellites of chromosomes—Small segments of genetic material at the tips of the short arms of chromosomes 13, 14, 15, 21, and 22.
Submetacentric—Positioning of the centromere between the center and the top of the chromosome.
some. Lastly, group G consists of chromosome pairs 21, 22 and the Y chromosome. These are short chromosomes with their centromeres at the top. Chromosome pairs 21 and 22 have satellites. The Y chromosome does not have satellites.
The actual chromosomes are only individually distinguishable during a certain stage of cell division. This stage is called the metaphase stage. Chromosome preparations are made from pictures of the chromosomes during the metaphase stage of division. The metaphase spread is what the technician sees in one cell under the microscope and what the photograph of that one cell is referred to. Usually, the chromosomes in a metaphase preparation are banded by special staining techniques used in the laboratory. Each numbered chromosome is unique in its banding pattern so that all number 1s look the same and all number 2s look the same, etc. Although, there can be small normal familial variations in chromosomes. Because of banding, the chromosomes are more easily distinguishable from each other and the banding makes it is easier to see differences or abnormalities. For example, if a chromosome is missing a piece, or two chromosomes are attached to each other (translocation), it is much easier to see with banded chromosomes than with unbanded chromosomes.
Chromosome preparations can be made from any potentially dividing cells, including; blood cells, skin cells, amniotic fluid cells (the fluid surrounding an
Karyotype
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
633 |

Kennedy disease
Karyotype showing three copies of chromosome 21. This indicates Down syndrome. (Custom Medical Stock Photo, Inc.)
unborn baby), placental tissue or chorionic villi (tissue that forms the placenta and can be used in prenatal diagnosis).
ISCN formulas exist to describe any chromosome complement. The basic formula for writing a karyotype is as follows. The first item written is the total number of chromosomes, followed by a comma. The the second item written is the sex chromosome complement. The typical female karyotype is written as 46,XX and the typical male karyotype is written as 46,XY.
Formulas for abnormal karyotypes
Many formulas for writing abnormal karyotypes have been determined. Some common examples follow. A plus or a minus sign before a chromosome number is used to show that the entire chromosome is extra or missing. Also, the total number of chromosomes will be different than 46. For example, the condition Down syndrome occurs when an individual has an extra number 21 chromosome. For a male, this karyotype is written as 47,XY, 21. An individual may also have extra or missing parts of chromosomes. The short arm of a chromosome is called the p arm and the long arm is called the q arm. For example, the condition Wolf-Hirschhorn syndrome is caused by a missing part of the top arm of chromosome 4. For a female, this karyotype would be written as 46,XX,del(4)(p16). The chromosome that is involved in the change is specified within the first set of parentheses and the breakpoint for the missing material is defined in the second set of parentheses. A final example
is a balanced translocation karyotype. A balanced translocation means that there is no missing or extra genetic material as the result of the translocation. There are many types of translocations. One type is called a robertsonian translocation. A robertsonian translocation occurs when two acrocentric chromosomes are attached together. One common example is a translocation involving chromosomes 13 and 14. If a male has a balanced robertsonian translocation of chromosomes 13 and 14, this is written as 45,XY,der(13;14). The “der” stands for derivative, as the new 13;14 chromosome is considered a derivative. There are only 45 separate chromosomes now, which is why 45 is the number written in the karyotype. There are many more formulas for the abundant abnormal chromosome findings in individuals. For further detailed information, please refer to the resource listed below.
Resources
BOOKS
Mitelman, Felix, ed. An International System for Human
Cytogenetic Nomenclature (1995). Farmington, CT: S. Karger AG, 1995.
Renee A. Laux, MS
Karyotype analysis see Karyotype
Keller syndrome see FG syndrome
I Kennedy disease
Definition
Kennedy disease (KD) is a disorder characterized by degradation of the anterior horn cells of the spinal cord resulting in slow progressive muscle weakness and atrophy. Men with Kennedy disease often have breast enlargement (gynecomastia), testicular atrophy, and may have infertility.
Description
Kennedy disease, also referred to as spinobulbar muscular atrophy (SBMA), arises primarily from degradation of the anterior horn cells of the spinal cord, resulting in proximal weakness and atrophy of voluntary skeletal muscle. Anterior horn cells control the voluntary muscle contractions from large muscle groups such as the arms and legs. For example, if an individual wants to move his/her arm, electrical impulses are sent from the brain to the anterior horn cells to the muscles of the arm, which then stimulate the arm muscles to contract, allow-
634 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |

ing the arm to move. Degradation is a rapid loss of functional motor neurons. Loss of motor neurons results in progressive symmetrical atrophy of the voluntary muscles. Progressive symmetrical atrophy refers to the loss of function of muscle groups from both sides of the body. For example, both arms and both legs are equally affected by similar degrees of muscle loss and the inability to be controlled and used properly. Progressive loss indicates that muscle loss is not instantaneous, rather muscle loss occurs consistently over a period of time. These muscle groups include those skeletal muscles that control large muscle groups such as the arms, legs and torso. The weakness in the legs is generally greater than the weakness in the arms.
Proximal weakness is in contrast to distal weakness, and indicates that muscles such as the arms and the legs are affected rather than the muscles of the hands, feet, fingers, and toes. However, the motor neuron of the brainstem and sensory neurons of the dorsal root ganglia are also affected in KD. Motor neurons are the neurons that control large muscle groups (arms, legs, torso) of which anterior horn cells are a subgroup. Sensory neurons are a distinct class of neurons that control an individual’s senses. An example would be pain receptors that cause an involuntary reaction to a stimuli such as when a person accidentally grasps a boiling hot kettle and immediately releases the kettle. Dorsal root ganglia are analogous to a headquarters for neurons, through which essentially all neuronal stimuli are processed.
Diagnosis
Kennedy disease is suspected clinically in a male with an early adulthood onset of proximal muscle weakness of the limbs, fasticulations (small local contractions of the musculature that is visible through the skin) of the tongue, lips or area around the mouth, absence of hyperactive reflexes and spasticity, and often evidence of enlarged breasts and/or small testes with few or no sperm.
The diagnosis is made by a specific molecular genetic test that measures the number of “repeats” in a particular part of the androgen receptor (AR) gene. The alteration of the AR gene that causes Kennedy disease is an expansion of a CAG trinucleotide repeat in the first PART of the gene. In unaffected individuals, between 11 to 33 copies OF the CAG trinucleotide are present. In patients with Kennedy disease, this number rises to 40 to 62. The greater the number of expanded repeats, the earlier the age of onset.
Genetic profile
Kennedy disease is an X-linked recessive disease, meaning the abnormal gene is found on the X chromo-
K E Y T E R M S
Anterior horn cells—Subset of motor neurons within the spinal cord.
Atrophy—Wasting away of normal tissue or an organ due to degeneration of the cells.
Degradation—Loss or diminishing.
Dorsal root ganglia—The subset of neuronal cells controlling impulses in and out of the brain.
Intragenic—Occuring within a single gene.
Motor neurons—Class of neurons that specifically control and stimulate voluntary muscles.
Motor units—Functional connection with a single motor neuron and muscle.
Sensory neurons—Class of neurons that specifically regulate and control external stimuli (senses: sight, sound).
Transcription—The process by which genetic information on a strand of DNA is used to synthesize a strand of complementary RNA.
Voluntary muscle—A muscle under conscious control, such as arm and leg muscles.
some and two copies of the abnormal gene must be present for the disorder to occur. Since males only inherit one X chromosome (the other is the Y chromosome) they will always express an X-linked disorder if the abnormal gene is on the X chromosome they receive. Females on the other hand inherit two X chromosomes. Even if one X chromosome contains the abnormal gene, the second X chromosome with a normal functioning gene can usually compensate for the other. Males lack the second X chromosome that may be able to mask the effect of the abnormal gene.
The disease was first characterized in 1968. The KDdetermining gene, androgen receptor (AR), maps to the proximal long arm of the X-chromosome.
The AR protein is a member of the steroid-thyroid hormone receptor family and is involved in transcription regulation. Transcription regulation is the molecular process that controls the “reading” of the genetic DNA information and turning it into RNA which is the material which generates proteins.
Demographics
Because of the X-linked inheritance pattern of Kennedy disease, only males are affected by this disor-
disease Kennedy
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
635 |

Klinefelter syndrome
der. Females may be carriers of the disease if they possess an abnormal gene on one of her X chromosomes. Due to the rare nature of this disease, and the fact that it may frequently be misdiagnosed as another form of neuromuscular disease, no particular race or ethnicity appears to be at greater risk than another.
Kennedy disease is primarily an adult disease, with an onset between the third and fifth decade of life. Once symptoms present, the disease is slowly progressive. In addition to neuronal cell loss, breast enlargement (gynecomatia), reduced fertility and testicular atrophy have also been reported in affected males.
Treatment and management
To date, there is not treatment for SBMA. However, there are possible mechanisms through which treatment could be developed. Gene therapy could be used for SBMA to replace the abnormal gene associated with SBMA with a copy carrying fewer CAG repeats. Currently this is not possible or available.
As the bulbar muscles of the face are affected, eating and swallowing can become difficult. Due to the weakening of the respiratory muscles, breathing can also be labored. It is therefore essential for patients to undergo chest physiotherapy (CPT). CPT is a standard set of procedures designed to trigger and aid coughing in patients. Coughing is important as it clears the patient’s lungs and throat of moisture and prevents secondary problems, such as pneumonia.
As symptoms progress, patients may require a ventilator to aid breathing.
Prognosis
The majority of patients with SBMA have a normal life span. About 10% of older, severely affected patients with SBMA may die from pneumonia or asphyxiation secondary to weakness of the bulbar muscles.
Resources
BOOKS
Zajac, J.D., and H.E. MacLean. “Kennedy’s Disease: Clinical Aspects.” In Genetic Instabilities and Hereditary Neurological Diseases, edited by R.D. Wells and S.T. Warren. New York: Academic Press, 1998, pp. 87-100.
PERIODICALS
Crawford, T.O., and C.A. Pardo. “The Neurobiology of Childhood Spinal Muscular Atrophy.” Neurobiology of Disease 3 (1996): 97-110.
Ferlini, A., et al. “Androgen Receptor CAG Repeat Analysis in the Differential Between Kennedy’s Disease and Other Motoneuron Disorders.” American Journal of Human
Genetics 55 (1995): 105-111.
ORGANIZATIONS
Kennedy Disease (SBMA) Support Group. 1804 Quivira Road, Washington, KS 66968. (785) 325-2629. gryphon @grapevine.net. http://www.geocities.com/HotSprings/ Villa/1989 .
National Ataxia Foundation. 2600 Fernbrook Lane, Suite 119, Minneapolis, MN 55447. (763) 553-0020. Fax: (763) 5530167. naf@mr.net. http://www.ataxia.org/ .
WEBSITES
Families of Spinal Muscular Atrophy. http://www.fsma.org . The Andrew’s Buddies web site. FightSMA.com
http://www.andrewsbuddies.com/news.html .
Muscular Dystrophy Association. http://www.mdausa.org .
Philip J. Young
Christian L. Lorson, PhD
Ketotoic hyperglycinemia see Propionic acidemia
Kinky hair disease see Menkes syndrome
Klein-Waardenburg syndrome, see
Waardenburg syndrome
I Klinefelter syndrome
Definition
Klinefelter syndrome is a chromosome disorder in males. People with this condition are born with at least one extra X chromosome.
Description
Klinefelter syndrome is a condition where one or more extra X-chromosomes are present in a male. Boys with this condition appear normal at birth. They enter puberty normally, but by mid-puberty have low levels of testosterone causing small testicles and the inability to make sperm. Affected males may also have learning disabilities and behavior problems such as shyness and immaturity and are at an increased risk for certain health problems.
Genetic profile
Chromosomes are found in the cells in the body. Chromosomes contain genes, structures that tell the body how to grow and develop. Chromosomes are responsible for passing on hereditary traits from parents to child. Chromosomes also determine whether the child will be
636 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |

male or female. Normally, a person has a total of 46 chromosomes in each cell, two of which are responsible for determining that individual’s sex. These two sex chromosomes are called X and Y. The combination of these two types of chromosomes determines the sex of a child. Females have two X chromosomes (the XX combination); males have one X and one Y chromosome (the XY combination).
In Klinefelter syndrome, a problem very early in development results in an abnormal number of chromosomes. Most commonly, a male with Klinefelter syndrome will be born with 47 chromosomes in each cell, rather than the normal number of 46. The extra chromosome is an X chromosome. This means that rather than having the normal XY combination, the male has an XXY combination. Because people with Klinefelter syndrome have a Y chromosome, they are all male.
Approximately one-third of all males with Klinefelter syndrome have other chromosome changes involving an extra X chromosome. Mosaic Klinefelter syndrome occurs when some of the cells in the body have an extra X chromosome and the other have normal male chromosomes. These males can have the same or milder symptoms than non-mosaic Klinefelter syndrome. Males with more than one additional extra X chromosome, such as 48,XXXY, are usually more severely affected than males with 47,XXY.
Klinefelter syndrome is not considered an inherited condition. The risk of Klinefelter syndrome reoccurring in another pregnancy is not increased above the general population risk.
Demographics
Klinefelter syndrome is one of the most common chromosomal abnormalities. About one in every 500 to 800 males is born with this disorder. Approximately 3% of the infertile male population have Klinefelter syndrome.
Signs and symptoms
The symptoms of Klinefelter syndrome are variable and not every affected person will have all of the features of the condition. Males with Klinefelter syndrome appear normal at birth and have normal male genitalia. From childhood, males with Klinefelter syndrome are taller than average with long limbs. Approximately 20–50% have a mild intention tremor, an uncontrolled shaking. Many males with Klinefelter syndrome have poor upper body strength and can be clumsy. Klinefelter syndrome does not cause homosexuality. Approximately one-third of males with Klinefelter syndrome have breast growth, some requiring breast reduction surgery.
K E Y T E R M S
Chromosome—A microscopic thread-like structure found within each cell of the body and consists of a complex of proteins and DNA. Humans have 46 chromosomes arranged into 23 pairs. Changes in either the total number of chromosomes or their shape and size (structure) may lead to physical or mental abnormalities.
Gonadotrophin—Hormones that stimulate the ovary and testicles.
Testosterone—Hormone produced in the testicles that is involved in male secondary sex characteristics.
Most boys enter puberty normally, though some can be delayed. The Leydig cells in the testicles usually produce testosterone. With Klinefelter syndrome, the Leydig cells fail to work properly causing the testosterone production to slow. By mid-puberty, testosterone production is decreased to approximately half of normal. This can lead to decreased facial and pubic hair growth. The decreased testosterone also causes an increase in two other hormones, follicle stimulating hormone (FSH) and luteinizing hormone (LH). Normally, FSH and LH help the immature sperm cells grow and develop. In Klinefelter syndrome, there are few or no sperm cells. The increased amount of FSH and LH cause hyalinization and fibrosis, the growth of excess fibrous tissue, in the seminiferous tubules where the sperm are normally located. As a result, the testicles appear smaller and firmer than normal. With rare exception, men with Klinefelter syndrome are infertile because they can not make sperm.
While it was once believed that all boys with Klinefelter syndrome were mentally retarded, doctors now know that the disorder can exist without retardation. However, children with Klinefelter syndrome frequently have difficulty with language, including learning to speak, read, and write. Approximately 50% of males with Klinefelter syndrome are dyslexic.
Some people with Klinefelter syndrome have difficulty with social skills and tend to be more shy, anxious, or immature than their peers. They can also have poor judgement and do not handle stressful situations well. As a result, they often do not feel comfortable in large social gatherings. Some people with Klinefelter syndrome can also have anxiety, nervousness, and/or depression.
The greater the number of X-chromosomes present, the greater the disability. Boys with several extra X-chro- mosomes have distinctive facial features, more severe
syndrome Klinefelter
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
637 |

Klinefelter syndrome
|
A |
B |
C |
|
Egg |
|
|
Meiosis I |
Nondisjunction |
Disjunction |
Disjunction |
Meiosis II |
Disjunction |
Nondisjunction |
Disjunction |
Fertilization
Sperm
Zygote
Mitosls |
|
Nondisjunction |
Disjunction |
47,XXY |
47,XXY |
47,XY/47,XXY |
|
|
|
Mosaic |
|
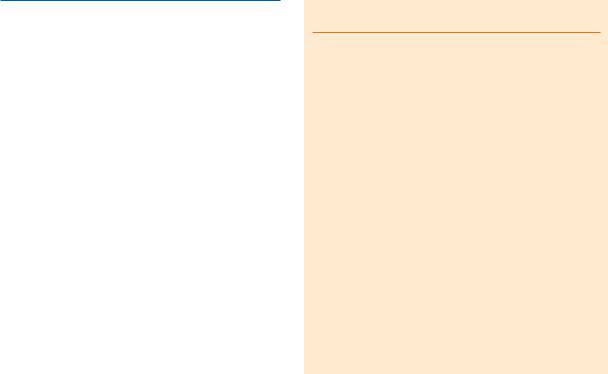
Nondisjunction, failure of paired chromosomes to separate, can result at different stages of meiosis or mitosis. When nondisjunction occurs in the first (A) or second (B) phase of meiosis the resulting karyotype will be 47,XXY. If the chromosomes fail to separate during mitosis (C) a mosaic kayrotype (46,XY/47,XXY) will result. (Gale Group)
retardation, deformities of bony structures, and even more disordered development of male features.
Diagnosis
Diagnosis of Klinefelter syndrome is made by examining chromosomes for evidence of more than one X chromosome present in a male. This can be done in pregnancy with prenatal testing such as a chorionic villus sampling or amniocentesis. Chorionic villus sampling is a procedure done early in pregnancy (approximately 10–12 weeks) to obtain a small sample of the placenta for testing. An amniocentesis is done further along in pregnancy (from approximately 16–18 weeks) to obtain a sample of fluid surrounding the baby for testing. Both procedures have a risk of miscarriage. Usually these procedures are done for a reason other than diagnosing Klinefelter syndrome. For example, a prenatal diagnostic procedure may be done on an older woman to determine if her baby has Down syndrome. If the diagnosis of Klinefelter syndrome is suspected in a young boy or adult male, chromosome testing can also be on a small blood or skin sample after birth.
Treatment and management
There is no treatment available to change chromosomal makeup. Children with Klinefelter syndrome may benefit from a speech therapist for speech problems or other educational intervention for learning disabilities. Testosterone injections started around the time of puberty may help to produce more normal development including more muscle mass, hair growth, and increased sex drive. Testosterone supplementation will not increase testicular size, decrease breast growth, or correct infertility.
Prognosis
While many men with Klinefelter syndrome go on to live normal lives, nearly 100% of these men will be sterile (unable to produce a child). However, a few men with Klinefelter syndrome have been reported who have fathered a child through the use of assisted fertility services. Males with Klinefelter syndrome have an increased risk of several conditions such as osteoporosis, autoimmune disorders such as lupus and arthritis, diabetes, and both breast and germ cell tumors.
638 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |