

|
|
|
Chapter 4 |
|
|
|
|
|
Equipment, Instruments, |
4 |
|
|
and Materials |
||
|
F. D. Fragiskos |
|
|
|
|
|
|
This chapter describes the necessary armamentarium, that is equipment and instruments, as well as the rest of the materials the dentist may use in oral surgery.
4.1
Surgical Unit and Handpiece
The surgical unit includes the following:
ΟSurgical micromotor. This is a simple machine with quite satisfactory cutting ability.
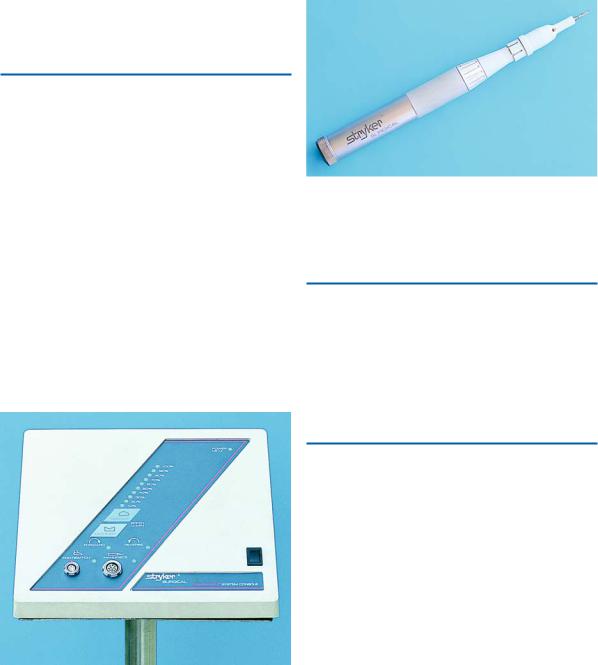
ΟTechnologically advanced machines, which function with nitrous dioxide or electricity (Fig. 4.1) and have a much greater cutting ability than the aforementioned micromotor.
The surgical handpiece is attached to the above unit, includes many types, and is manufactured to suit the needs of oral surgery (Fig. 4.2). Its advantages are as follows:
ΟIt functions at high speeds and has great cutting ability.
ΟIt does not emit air into the surgical field.
ΟIt may be sterilized in the autoclave.
Fig. 4.1. Electric surgical micromotor with adjustable speed
Fig. 4.2. High-speed surgical handpiece
ΟThe handpiece may receive various cutting instruments.
4.2
Bone Burs
The burs used for the removal of bone are the round bur and fissure bur (Fig. 4.3). A large bone bur similar to an acrylic bur may be used when the surgical procedure involves greater bone surface area (torus) or smoothing of bone edges of the wound.
4.3
Scalpel (Handle and Blade)
Handle. The most commonly used handle in oral surgery is the Bard–Parker no. 3. Its tip may receive different types of blades.
Blade. Blades are disposable and are of three different types (nos. 11, 12, and 15) (Fig. 4.4). The most common type of blade is no. 15, which is used for flaps and incisions on edentulous alveolar ridges. Blade no. 12 is indicated for incisions in the gingival sulcus and incisions posterior to the teeth, especially in the maxillary tuberosity area. Blade no. 11 is used for small incisions, such as those used for incising abscesses. The scalpel

44 F. D. Fragiskos
Fig. 4.3. Various types of surgical burs
Fig. 4.4. Scalpel and various types of scalpel blades (nos. 11, 12, 15) commonly used in oral surgery
Fig. 4.5. Correct way to load the scalpel blade on the handle of the scalpel
Fig. 4.6. Sliding of scalpel blade, with the male portion of the fitting facing upward, with the aid of a hemostat
blade is placed on the handle with the help of a needle holder, or hemostat, with which it slides into the slotted receiver with the beveled end parallel to that of the
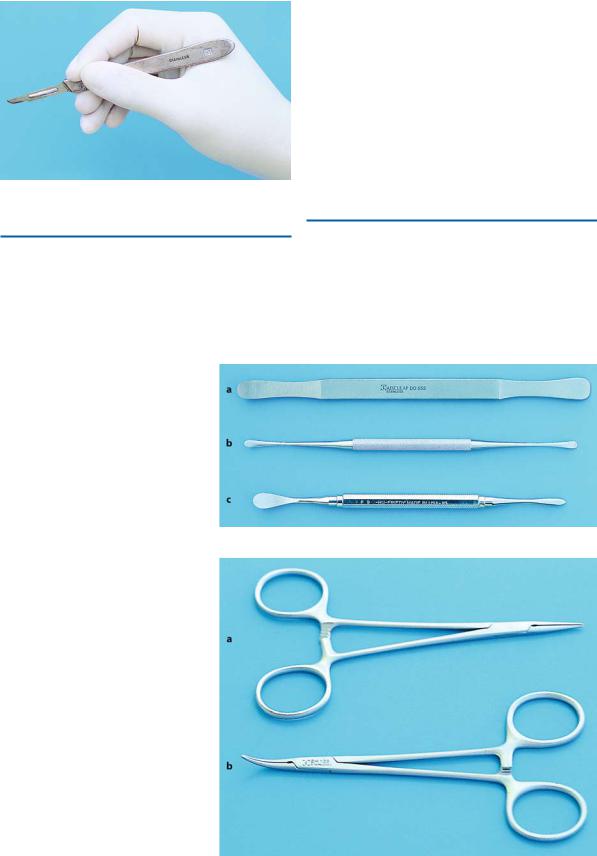
handle (Figs. 4.5, 4.6). The scalpel is held in a pen grasp and its cutting edge faces the surface of the skin or mucosa that is to be incised (Fig. 4.7).
Chapter 4 Equipment, Instruments, and Materials |
45 |
Fig. 4.7. Scalpel is held in a pen grasp
4.4
Periosteal Elevator
This instrument has many different types of end (Fig. 4.8). The most commonly used periosteal elevator in intraoral surgery is the no. 9 Molt, which has
two different ends: a pointed end, used for elevating the interdental papillae of the gingiva, and a broad end, which facilitates elevating the mucoperiosteum from the bone. The Freer elevator is used for reflecting the gingiva surrounding the tooth before extraction. This instrument is considered suitable, compared to standard elevators, because it is easy to use and has thin anatomic ends.
The elevator may also be used for holding the flap after reflecting, facilitating manipulations during the surgical procedure. The Seldin elevator is considered most suitable for this purpose.
4.5 Hemostats
The hemostats used in oral surgery are either straight or curved (Fig. 4.9). The most commonly used hemostat is the curved mosquito type or micro-Halsted hemostat, which has relatively small and narrow beaks
Fig. 4.8 a–c. Various types of periosteal elevators. a Seldin. b Freer. c No. 9 Molt
Fig. 4.9 a, b. Micro-Halsted hemostats. a Straight. b Curved
46 F. D. Fragiskos
Fig. 4.10 a, b. Surgical forceps.
a Standard. b Adson tissue forceps
so that they may grasp the vessel and stop bleeding. Hemostats may also be used for firmly holding soft tissue, facilitating manipulations for its removal.
4.6
Surgical – Anatomic Forceps
Surgical forceps are used for suturing the wound, firmly grasping the tissues while the needle is passed.
There are two types of forceps: the long standard surgical forceps, used in posterior areas, and the small, narrow Adson forceps, used in anterior areas (Fig. 4.10).
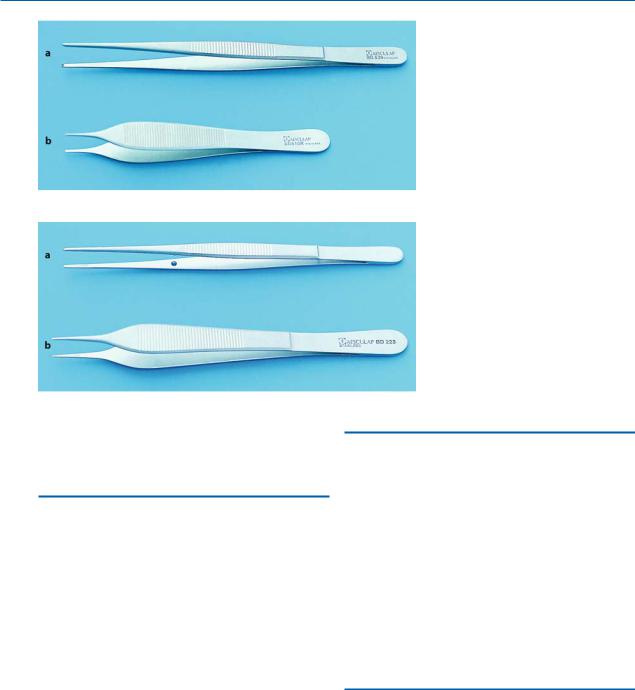
The beak of the forceps has a wedge-shaped projection or tooth on one side, and a receptor on the other, which fit into each other when the handles are locked. This mechanism allows the forceps to grasp the soft tissues found between the beaks very tightly. Anatomic forceps (Fig. 4.11) do not have a wedge-shaped projection, but parallel grooves. This type of forceps is used to aid in the suturing of the wound, as well as grasping small instruments, etc., during the surgical procedure.
Fig. 4.11 a, b. Anatomic dissecting forceps. a Standard. b Adson dissecting forceps
4.7
Rongeur Forceps
This instrument is used during intraoral surgery as well as afterwards, to remove bone and sharp bone spicules. The ends and sides of the sharp blades become narrow, so that when the handles are pressed, they cut the bone found in between without exerting particular pressure. There is a spring between the handles, which restores the handles to their original position every time pressure is applied for cutting bone.
The most practical rongeur in oral surgery is the Luer–
Friedmann, because its blades are both end-cutting and side-cutting (Fig. 4.12).
4.8 Bone File
This instrument has two ends: one small end and another with a large surface (Fig. 4.13). The cutting surface is made up of many small parallel blades, which are set in such a way that only pulling is effective. The bone file is used in oral surgery to smooth bone and not to remove large pieces of bone.