

новая папка / 450-550 operativ
.pdf482 |
SRB’s Surgical Operations |
be re-excised and con rmed for clearance. It is done either through same scar or modi ed elliptical incision which includes the scar – `Mexican hat incision.’
QUART Therapy
It is quadrantectomy, axillary dissection of level I and II nodes with separate axillary incision and postoperative radiotherapy to breast (5000 cGy) and axilla (1000 cGy). First it was started by Umberto Veronesi from Milan.
Axillary dissection is done to identify the nodal involvement of the disease which is an indicator of metastatic breast disease. It is also done for staging of malignancy. Number and level of nodes involved are independent predictors of the outcome of the disease. erapeutic bene t of axillary dissection is a debate. It is done basically for in ltrating carcinoma of breast. In situ carcinomas do not require axillary dissection as incidence of nodal spread in situ carcinoma is less than 2%. Axillary aps are elevated superiorly and inferiorly. Level I and II nodes are removed with fat and fascia. External mammary, lateral, subscapular and central nodes are removed. A minimum of 10 nodes should be removed. Wound is closed with a suction drain.
required pectoralis muscle should be divided from its insertion to coracoid process; index finger is passed around the insertion of the pectoralis minor tendon and muscle is traced towards coracoid process and is divided. Axillary vein is dissected to clear adipose tissue and lymph nodes on it. Now dissection should be done from lateral to medial using sharp and blunt dissection. Apex of the axilla should be cleared. Blood supply to pectoralis major muscle should be retained. Lower ap is dissected further to identify the serratus anterior muscle. Intercostobrachial nerve is identi ed and is preserved. Long thoracic nerve of Bell is 2 cm posterior to intercostobrachial nerve. It is in the serratus fascia. It should be identi ed and preserved. Further dissection exposes the thoracodorsal nerve (nerve to latissimus dorsi). oracodorsal vein is rst identi ed; thoracodorsal nerve is most medial in thoracodorsal neurovascular bundle. is entire neurovascular bundle should be preserved if latissimus dorsi ap is needed at later period to patient. Dissection is continued laterally and behind to remove all the tissues up to the axillary tail. Specimen is removed. Its directions are marked. Single suction drain is placed. Skin ap is sutured from its deeper plane to chest wall as quilting to prevent seroma formation. Wound is closed in layers. Pressure dressing is placed.
AXILLARY DISSECTION |
omplications |
It is done under general anaesthesia. Sandbag is placed under the shoulder to elevate the axilla. Arm, axilla, shoulder and same side chest wall is cleaned and draped. Forearm and hand are draped to facilitate holding and moving it as needed.
Incision is along the crease just below the hair bearing area of axilla. A lazy S incision between pectoralis major and latissimus dorsi muscle or an incision along the anterior axillary fold also can be used
(Fig. 16-25).
Fig. 16-25: Different incisions for axillary dissection.
Skin ap is elevated behind up to the edge of latissimus dorsi muscle. Upper skin ap is raised. Medial part of the dissection is done by identifying the pectoral muscles. Medial pectoral nerve which winds the lateral margin of the pectoralis minor muscle is identi ed. One must remember that medial pectoral nerve arises from the medial cord of the brachial plexus and often passes through the bres of the lateral part of the pectoralis minor muscle. Medial margin of the pectoralis minor is reached above to identify the part of clavipectoral fascia which contains few lymph nodes. It is upper medial limit of the dissection. Axillary vein meets the subclavius muscle here. When
 SKIN SPARING MASTECTOMY SSM
SKIN SPARING MASTECTOMY SSM
It is like a key-hole surgery of breast. Skin sparing/limited skinexcision (5-10%) will not alter/a ect the recurrence rate.
Indicationsarecentraltumour/multicentric/extensive intraductal/ T1/not feasible for breast conservation.
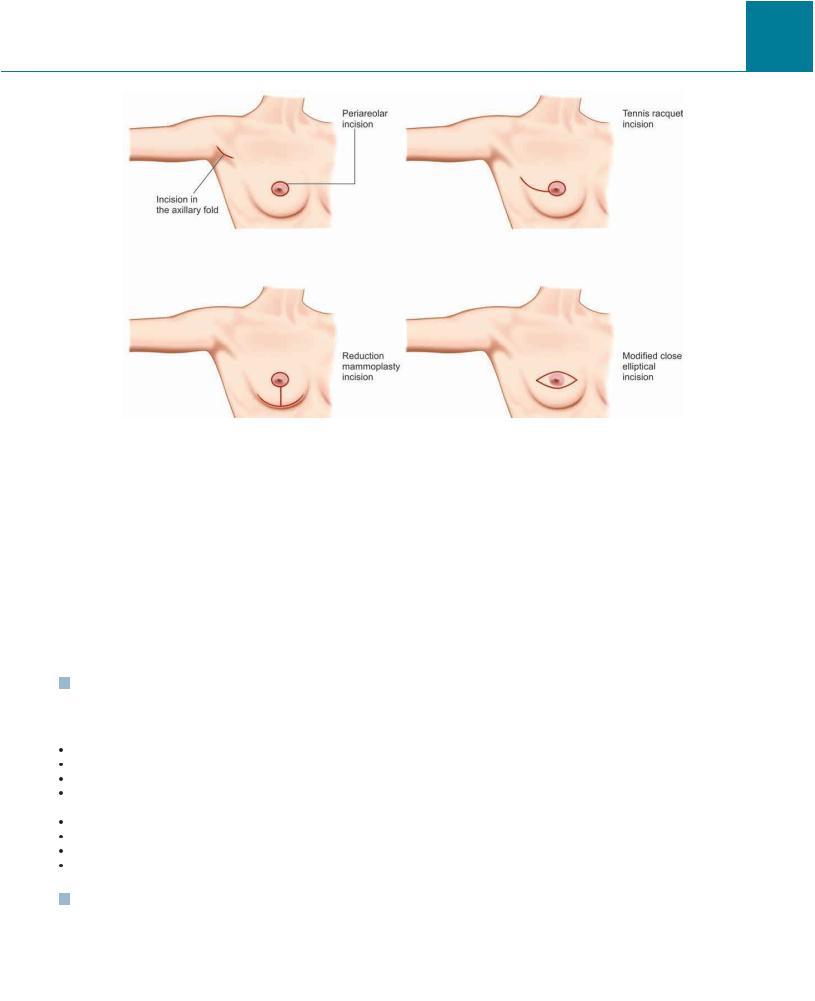
It includes excision of nipple-areola complex with very limited skin removal; marginal skin excision over the tumour/biopsy site; total glandular mastectomy; axillary dissection using either same (extension of SSM incision) or separate incision in the axilla.
Incision is either periareolar/tennis racquet/modi ed elliptical. Tennis racquet has got lateral extension to axilla. Reduction mammoplasty incision is also used with a periareolar incision extending vertically into an inframammary horizontal incision. Prior biopsy site should be included in the mastectomy incision or should be removed widely through a separate elliptical incision (Fig. 16-26).
Skin apsareelevatedbetweenbreastparenchymaandsubcutaneous adipose tissue allowing 5-10 mm thick skin ap. Circumferential ap is raised around using scissor/no. 15 scalpel blade/cautery (cutting is used; coagulation cancause cautery artifact). Skin hooks and retractors are used to facilitate the dissection. Headlight may be used to have a better visualisation during dissection. Parasternal and infraclavicular perforating vessels are preserved to maintain adequate blood supply of the retained skin. Superiorly dissection is done up to second rib; medially to sternum; below to inframammary crease; laterally to latissimus dorsi muscle. Entire breast tissue, nipple areolar complex
Chapter 16 Surgeries for Breast Diseases |
483 |
Fig. 16-26: Incisions used for skin sparing mastectomy (SSM).
are removed. Usually pectoral fascia is removed except in case of super cial tumours. Breast is raised o the pectoralis major muscle from the medial end towards lateral side. As it is raised it is delivered out of the wound to reach the dissection towards axillary tail. Axillary tail of Spence is separated from pectoralis major, minor and serratus anterior muscles. Junction of axillary tail and axillary tissue is clamped, ligated and cut. Axillary dissection may be added as decided. Wound is closed with a suction drain.
Immediate reconstruction with latissimus dorsi or TRAM ap is done with tissue expanders placed underneath the subcutaneous or submuscular plane.
Problems with SSM are – di culty in raising aps, haematoma/ seroma formation, infection (Figs 16-27 and 16-28).
INDICATIONS FOR TOTAL MASTECTOMY/ MODIFIED RADICAL MASTECTOMY IN BREAST CANCER
When tumour is more than 4 cm. Multicentric tumour.
Poorly di erentiated tumour.
Tumour margin is not clear of tumour after breast conservative surgery.
Recurrence after BCS.
Prior radiotherapy to breast.
Scleroderma or association with other collagen disease. Stage I invasive/Stage II, III diseases.
MODIFIED RADICAL MASTECTOMY MRM
In MRM, breast tissue, nipple areolar complex, skin over the breast tissue are removed along with axillary clearance with or without removal of pectoralis minor.
Patey’s operation – It is total mastectomy with clearance of all levels of axillary lymph nodes with removal of pectoralis minor muscle.
Scanlon operation – Here along with total mastectomy, pectoralis minor is not removed but incised to reach level III lymph nodes
Auchincloss operation – It is total mastectomy with axillary clearance (level I and II) keeping pectoralis minor intact. It is commonly advocated now.
Patey’s operation: It is total mastectomy along with clearance of all levels of axillary nodes and removal of pectoralis minor muscle. It is en bloc dissection of breast and axilla.
General anaesthesia is used for the procedure. Patient lies in supine position with sandbag under the same side thorax and shoulder. Side of the chest wall, breast area, axilla, neck and sides are cleaned and draped. Same side entire arm and forearm is cleaned and is covered with drape and stockings. Shoulder should have free movement as needed during dissection of the axilla. Shoulder is kept in abducted and extended position. Surgeon stands on the side; first assistant near the shoulder on the same side; second assistant on opposite side; scrub nurse stands next to the surgeon near the leg side.
Di erent incisions are used as shown in Figures 16-29 to 16-35.
Classic elliptical Stewart incision is commonly used. Incisionis decided by the surgeon who is operating.
An elliptical incision is made from medial aspect of the second and third intercostals space enclosing the nipple, areola and tumour extending laterally into the axilla along the anterior axillary fold. Upper and lower skin aps are raised. Flap is raised mainly using scissor/scalpel/cutting cautery along with blunt gauze dissection in between. It extends medially up to the midline on the sternum; laterally to anterior margin of the latissimus dorsi muscle; above up to second rib/subclavius muscle; below 3 cm down the inframammary fold. Skin with subcutaneous fat is dissected o while raising the ap.

484 |
SRB’s Surgical Operations |
Fig. 16-27: Skin sparing mastectomy for carcinoma breastdifferent approaches. Skin sparing mastectomy (SSM) does not affect the recurrence rate.
Breast with tumour is raised from the medial aspect of the pectoral major muscle with pectoral fascia by making a deep incision close to midline, adjacent to sternum. Dissection is proceeded laterally ligating perforating vessels derived from lateral thoracic and anterior intercostal arteries. Once dissection reaches axilla, lateral border of pectoralis major muscle and pectoralis minor is exposed in deeper plane. Medial pectoral nerve (is lateral arises from medial cord of brachial plexus) which supplies lateral part of the pectoralis major muscle is identi ed here and preserved.
Axillary lymph node dissection is now started in continuity with mastectomy. Investing layer of deep fascia is divided. Fascia in front of the axillary vein is dissected to expose the vein in front. Small tributaries are ligated. Pectoralis major is retracted superomedially. Finger is swept between the two pectori to clear the Rotter’s nodes. Lateral pectoral nerve is identi ed and preserved (it arises from lateral cord and is located medially supplies the medial part of pectoralis major). Attachment of pectoralis minor tendon is feltwith index nger and with
nger dissection it is hooked round the nger close to coracoid process

Chapter 16 Surgeries for Breast Diseases |
485 |
Fig. 16-28: Skin sparing mastectomy incision with prosthesis implant for placement.
Fig. 16-29: A horizontal or oblique incision is commonly used for total mastectomy or modi ed radical mastectomy.

486 |
SRB’s Surgical Operations |
Fig. 16-30: Gray incision crosses the midline towards the opposite side.
Fig. 16-31: Greenough incision.
Fig. 16-32: Kocher’s incision for mastectomy. |
Fig. 16-33: Orr incision for mastectomy. |

Chapter 16 Surgeries for Breast Diseases |
487 |
Fig. 16-34: Rodman incision for mastectomy with two branches in the nal wound.
Fig. 16-35: Classical Stewart incision for mastectomy.

488 |
SRB’s Surgical Operations |
and is divided from coracoid process to clear level II nodes. Later from the apex of axilla level III nodes are cleared. Pectoralis minor muscle, after cutting from the coracoid process may or may not be removed. Axillary vein is cleared up to subclavius muscle medially. Posterior and lateral group of lymph nodes are cleared. Subscapularis medially and teres major laterally are exposed posteriorly. Nerve to serratus anterior (long thoracic nerve of Bell), nerve to latissimus dorsi with vessels (thoracodorsal neurovascular bundle), intercostobrachial nerve, axillary vein, cephalic vein and pectoralis major muscle are preserved. Long thoracic nerve is located in front of the subscapularis medially on the chest wall within the investing fascia. Once specimen is removed it is marked with orientation markers or clips (Figs 16-36 to 16-38).
Fig. 16-36: Nerve to serratus anterior (long thoracic nerve of Bell), thoracodorsal nerve, medial pectoral and lateral pectoral nerves and intercostobrachialnervesusuallycomeacrossduringMRM.Medialpectoral nerve arising from medial cord of brachial plexus (hence the name) winds around the lateral margin of the pectoralis minor muscle (40%) or passes through its lateral part of bres (60%), supplies part of the pectoralis major muscle. Lateral pectoral nerve arising from lateral cord of the brachial plexus runs close to the medial margin of pectoralis minor muscle to supply mainly pectoralis major muscle as its dominant nerve.
Wound is washed with saline. Haemostasis is maintained. Two silastic suction drains are placed, one laterally adjacent to latissimus dorsi muscle; another in front of the pectoralis major muscle. Wound is closed with a suction drain. Suction drain is kept for 5 – 7 days or until drainage becomes less than 30 ml per day (Fig. 16-39).
Complications of MRM/mastectomy
•Injury/thrombosis ofaxillary vein
•Seroma50% - It should be aspirated repeatedly supported with compression dressing.
•Shoulder dysfunction10%
•Pain (30%) and numbness (70%)
•Flap necrosis/infection
•Haematoma formation – Iflarge needs drainage under general anaesthesia.
•Lymphoedema(15%) and its problems – Dissection above the axillary vein level increases the incidence of lymphoedema.
•Axillary hyperesthesia (0.5-1%)
•Winged scapula –Prominent medial border and inferior angle of scapula during punching action.
Contd...
Contd...
•Stewart – Treves syndrome is development of lymphangiosarcoma of upper limb in patient who develop lymphoedema (after5 years)after mastectomy
•Weakened shoulder adduction due to injuryto thoracodorsal nerve.
•Anaesthesia over the medialaspect of the upper arm (dysesthesia) due to injuryto intercostobrachial nerve.
•Atrophy of pectoralis major muscle with loss of chest wall contour due to injuryto medialpectoral nerve.
Mastectomy specimen should be carefully inspected and sent to pathology department
•Specimen is sent in formalin for histology.
•It is sent in saline in low temperature for ER/PR/Her 2 neu status study (histochemistry).
•Tumor grading, tumor clearance, nodal involvement - its number and capsular breach are assessed histopathologically.
Points to be remembered
Subcutaneous fat is included while elevating the flap of the breast skin; but it shouldbe removed inaxillary flaps.
Dissection inthe axilla shouldbe kept below the levelofaxillary vein.
All nerves in the axilla which will come across should be preserved as much as possible.
Subscapular/thoracodorsal vessels should be retained if LD flap is planned. Proper haemostasis is essential.
Doubletubesilasticdrainisamust.Drainisremovedwhenonlythedischarge drained becomes less than 30 ml/day for 2 days.
 DIFFERENT MASTECTOMIES
DIFFERENT MASTECTOMIES
Total mastectomy also called as simple mastectomy – Here tumour, entire breast, nipple areola complex, axillary tail are removed. Axillary dissection is not done.
Extended total (simple) mastectomy is doing total mastectomy with clearance of level I axillary lymph nodes.
Modi ed radical mastectomy (MRM) is total mastectomy with axillary clearance. In Patey’s MRM all levels of axillary nodes are cleared with division of tendonof pectoralis minor muscle close to coracoid process with or without removal of the pectoralis muscle. In Scanlon’s MRM pectoralis minor is incised to reach the level III nodes. In Auchincloss MRM only level I and II are removed, pectoralis minor is left intact.
Breast conservative surgery (BCS) is done only when indications mentioned earlier is met with. It is often added with axillary dissection. Radiotherapy to breast is a must. Wide local excision is the commonly done procedure. Veronesi designed quadrantectomy, axillary dissection and radiotherapy (QUART) in BCS.
Skin sparing mastectomy (SSM) is keyhole surgery in which total mastectomy is done with removal of nipple areolar complex, earlier biopsy scar and entire breast and tumour. Skin over the breast is retained as the outcome of the disease will not be altered by removal or not removal of the skin widely over the breast.
Radical mastectomy (Halsted) is removal of tumour, entire breast, nipple, areola, and skin over the breast and tumour, pectoralis major and minor muscles, fat, fascia, nodes in the axilla. Axillary vein, long thoracic nerve and cephalic vein are retained (Fig. 16-40).

Chapter 16 Surgeries for Breast Diseases |
489 |
Figs 16-37(1)
490 |
SRB’s Surgical Operations |
Figs 16-37(2)

Chapter 16 Surgeries for Breast Diseases |
491 |
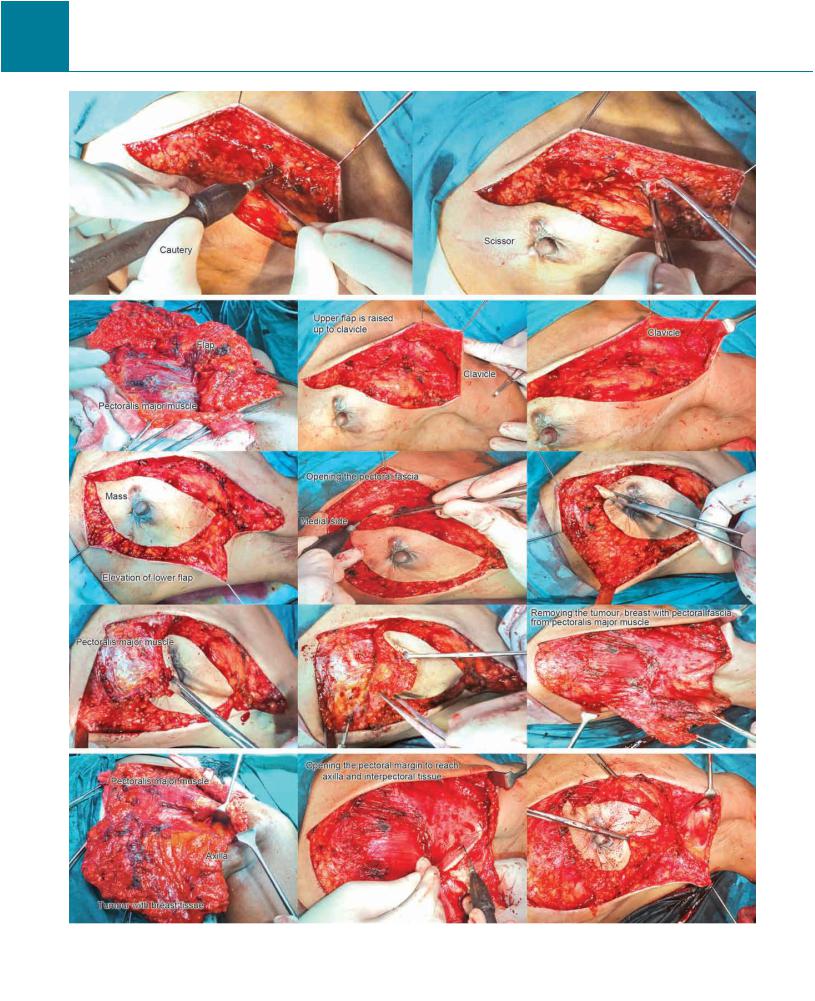
Figs 16-37(3)
Figs 16-37(1 to 3): Technique of modi ed radical mastectomy (MRM). Skin over the breast, whole of ipsilateral chest wall, axilla, shoulder, supraclavicular region with neck, part of abdomen and part of opposite chest wall are prepared with antiseptic solution. Slight head up (Fowler’s) position with same side tilting of the table upwards often with a sandbag under the shoulder region is used. Hand and forearm is often covered with a sterile towel so that to achieve a free movement of the arm and shoulder during axillary dissection. Incision placed depends on the need, either transverse or oblique which will be 5 cm beyond the tumour margin as an elliptical type. Upper ap is elevated rst usually up to the level of clavicle above; up to sternum medially. Lower ap is elevated up to rectus sheath and costal margin below. Lateral ap is elevated up to the margin of latissimus dorsi muscle. Flaps are elevated using either cautery or scissor or scalpel or often with gauze dissection. In axillary region, subcutaneous tissue and fat is also cleared. Fascia on the lateral margin of pectoralis major is incised to expose the pectoralis minor. Deeper part of the pectoralis minor is dissected to expose the axillary vein beyond the subscapular vessels. Clavipectoral fascia is incised to clear the nodes, taking care not to injure the medial pectoral nerve which passes through the pectoralis minor (60%) or its lateral margin (40%) to supply pectoralis major muscle. Main supply of pectoralis major is lateral pectoral nerve which passes medial to the pectoralis minor close to acromiothoracic artery. Pectoralis minor is retracted to clear the apical nodes. Often pectoralis minor tendon is detached from its insertion to coracoid process (Patey’s). The fascia over serratus anterior is cleared without injuring long thoracic nerve. Intercostobrachial nerve, if possible, is saved. Posteriorly dissection is continued over subscapular muscle preserving the subscapular vessels and thoracodorsal nerve. At the end specimen is freed from latissimus dorsi.