

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index

Isoechoic
Gland |
Diffuse Changes |
||||
|
|
|
|||
|
|
|
|
Circumscribed Changes |
|
|
|
|
|
||
Thyroid |
|
|
Anechoic |
||
|
|
Hyperechoic |
|||
|
|
|
|
|
Hypoechoic |
|
|
|
|
|
Isoechoic |
|
|
|
|
|
Irregular |
|
|
|
Differential Diagnosis of Hyperthyroidism |
||
|
|
|
|||
Normofollicular Adenoma Hemorrhagic or Colloid Cyst
Regressive Changes in an Adenoma or Adenomatous Nodule
Parathyroid Adenoma/Hyperplasia Lipoma
Normofollicular Adenoma 













































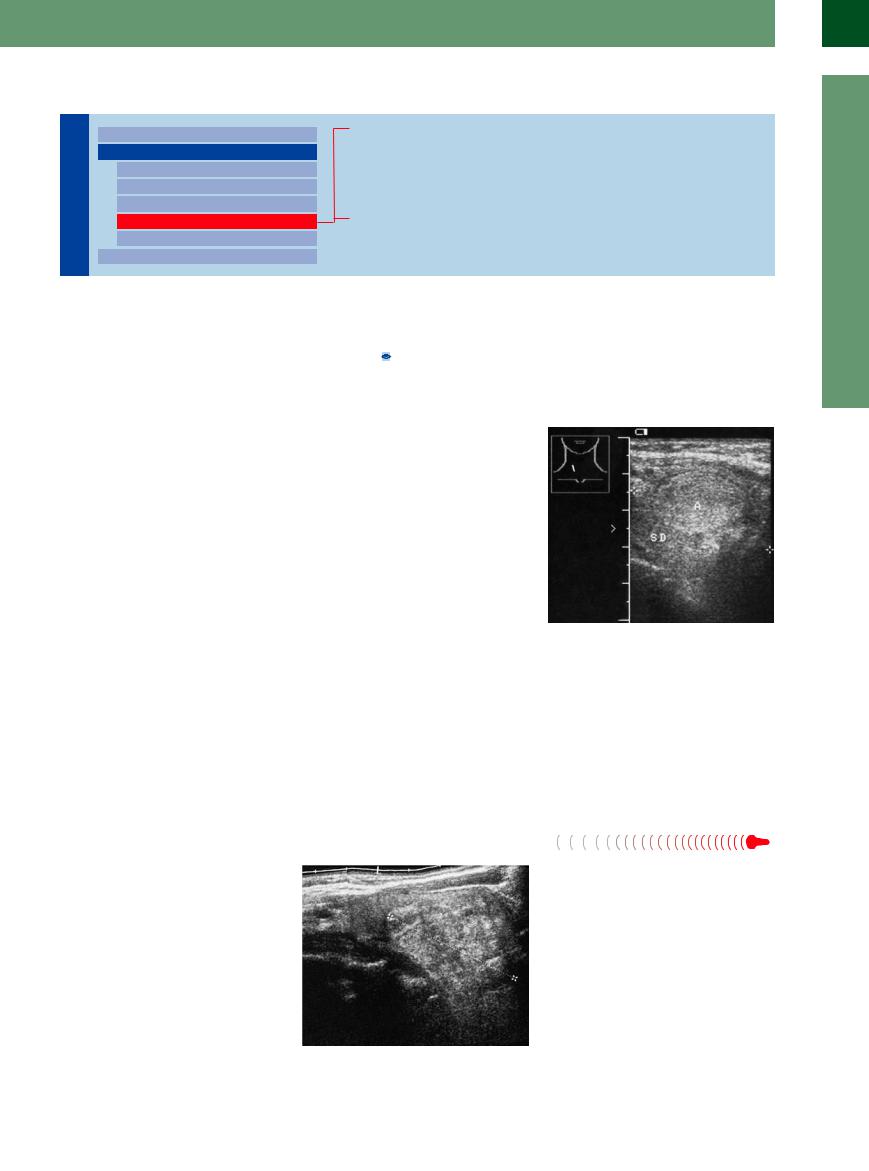
As a rule, solitary isoechoic nodules in the thyroid gland are normofollicular adenomas. They have the same echo structure as the rest of the thyroid parenchyma and can be distinguished only by their hypoechoic or anechoic rim (halo). Normofollicular thyroid nodules, like hypoechoic nodules, may show increased radiotracer uptake at scintigraphy, identifying them as autonomous adenomas. By contrast, hyperechoic adenomas almost never show uptake that indicates autonomy.
Sonographic features. Normofollicular adenomas have the same reflectivity as normal thyroid tissue, with the result that adenomas usually are not detectable with ultrasound unless they are located at the periphery of the gland and cause an appreciable contour bulge. They may be circumscribed by an echo-poor vascular rim (Fig.14.48,  14.3b).
14.3b).
Fig. 14.48 Isoechoic adenoma (A) in a euthyroid patient. M = muscle.
a B-mode image shows an elliptical halo in an otherwise normal-appearing thyroid (TH).
b Color Doppler demonstrates a vascular rim with slight internal vascularity.
Hemorrhagic or  Colloid
Colloid Cyst
Cyst 












































Besides adenomas, isoechoic nodules may be caused by fresh bleeding within a cyst or by large colloid-containing cysts. These cystic lesions can be identified as such by noting their compressibility at ultrasound. Subtle movements of the cyst contents may also be observed. FNA can quickly resolve any doubts as to whether the mass is liquid or solid (Fig.14.49,  14.2f). Carcinomas are rarely isoechoic and are almost never hyperechoic.
14.2f). Carcinomas are rarely isoechoic and are almost never hyperechoic.
Fig. 14.49 A cyst with internal hemorrhage is predominantly isoechoic and creates a bulge in the thyroid contour. Fine-needle aspiration identified this lesion as a chocolate cyst.
14
Circumscribed Changes
499

14
Thyroid Gland
Regressive Changes
Changes in an
in an Adenoma or
Adenoma or Adenomatous Nodule
Adenomatous Nodule 


























Adenomas tend to undergo regressive changes over time. As collagenous connective tissue is formed, the initially hypoechoic nodules become more echogenic. The adenomas lose their homogeneous structure, and other regressive changes such as cyst formation and calcification may supervene, giving the nodule an irregular or heterogeneous echo structure (Fig.14.50).
Fig. 14.50 |
b CDS: incomplete vascular rim, one internal vascular |
a Isoechoic adenomas (cursors), longitudinal scan of the |
spot. In total, there are no definite criteria for malignancy. |
right thyroid lobe: the caudal nodule shows incomplete |
|
rim calcification, one internal calculus. |
|
Parathyroid Adenoma/Hyperplasia


















Parathyroid adenoma and hyperplasia are predominantly hypoechoic but also isoechoic and rarely hyperechoic (regression). They are to be found at the usual positions dorsally, laterally of the thyroid poles, and most commonly at the lower poles (Fig.14.51).
Lipoma
Fig. 14.51 Parathyroid adenoma (cursors), located dorsally and close to the aorta (AO).
A lipoma is occasionally misinterpreted clinically as a nodular goiter. While its ultrasound features resemble those of adenoma or microcystic nodular transformation, it can be distinguished (when considered in the differential diagnosis) by its typical mottled or streaky isoechoic appearance and by the lack of vessels in the CDS. The thyroid can usually be clearly delineated from the lipoma embedded in the anterior subcutaneous fat (Fig.14.52).
Fig. 14.52 Patient had received replacement therapy for a goiter for years. A nodule extends far toward the right side. A lipoma is delineated only by its lack of vascularity on color duplex examination of the thyroid gland (TH). AC = common carotid artery.
500
Hyperechoic
Gland |
Diffuse Changes |
||||
|
|
|
|||
|
|
|
|
Circumscribed Changes |
|
|
|
|
|
||
Thyroid |
|
|
Anechoic |
||
|
|
Hyperechoic |
|||
|
|
|
|
|
Hypoechoic |
|
|
|
|
|
Isoechoic |
|
|
|
|
|
Irregular |
|
|
|
|
|
|
|
|
|
Differential Diagnosis of Hyperthyroidism |
||
|
|
|
|||
Macrofollicular Adenoma or Nodule Hemorrhagic Cyst, Colloid Cyst Nodule with Regressive Changes
Hemangioma, Myolipoma, Thyroid Regressive Changes Calcifications
Hyperechoic lesions in the thyroid gland may |
Regressive changes may consist of cystic trans- |
connective tissue is very echogenic. Thus, high |
be macrofollicular adenomas, adenomatous |
formation, fibrous changes with collagenous or |
echogenicity in a nodule may by caused by a |
nodules, nodules with regressive fibrous |
hyaline connective tissue formation, and calci- |
histomorphological macrofollicular structure |
changes, or in rare cases benign tumors such |
fications. Hyaline connective tissue has a very |
or by the presence of collagenous connective |
as hemangiomas, lipomas, and myolipomas. |
low reflectivity ( 14.1a), whereas collagenous |
tissue in the nodule. |
Macrofollicular Adenoma or Nodule
or Nodule 








































Solitary hyperechoic nodules in an otherwise normal thyroid gland are generally macrofollicular adenomas. They show no tracer uptake at scintigraphy, appearing as cold nodules. Scintigraphy cannot evaluate the structural changes that underlie cold nodules, which may represent carcinoma, fibrous regressive nodules, or cysts. Sonography is an ideal complement to scintigraphy in making this kind of differentiation (Table 14.5).
Hyperechoic adenomas are less common than hypoechoic microfollicular adenomas. Macrofollicular nodules show little or no internal vascularity when evaluated by color Doppler.
Nodules with fibrous regressive changes, like macrofollicular adenomas, are more echogenic than normal thyroid tissue but tend to display a coarsely granular to patchy echo texture (Fig.14.53).
Fig. 14.53 Hyperechoic adenoma (A) in a normal thyroid gland (TH, cursors), delineated by peripheral vascularity.
Hemorrhagic Cyst, Colloid Cyst











































Hemorrhagic or colloid cysts may exhibit a hyperechoic or irregular echo structure. They are sharply marginated compared with other hyperechoic masses. The nature of the mass is determined by FNA ( 14.2f, Fig.14.49).
14.2f, Fig.14.49).
Nodule with Regressive
Regressive Changes
Changes



















A nodular goiter of long standing will generally |
Fig. 14.54 Hyperechoic, nonhomogeneous thyroid nodule |
contain nodules with regressive changes. |
(cursors) with regressive changes. |
Cystic transformation and calcification are |
|
common along with fibrous changes |
|
(Fig.14.54). |
|
14
Circumscribed Changes
501

14
Thyroid Gland
Hemangioma, Myolipoma,
Myolipoma,  Thyroid Regressive Changes
Thyroid Regressive Changes 





























Parathyroid adenoma and hyperplasia demonstrate a predominantly hypoechoic structure; in very rare conditions they may also present a very high reflectivity due to regressive changes. As a differential diagnosis, hemangiomas and myomas should also be taken into consideration. When these lesions are found, it is difficult to tell what histopathological elements are responsible for their high echogenicity. They have no real clinical significance (Fig.14.55).
Fig. 14.55 Small, round, hyperechoic nodule (cursors) in a hypoechoic thyroid gland. The differential diagnosis consists of hemangioma, lipoma, and thyroid adenoma with regressive changes. The patient presented with renal failure and mild hyperparathyroidism.
Calcifications 




















































Calcifications occur in large, long-standing |
range in size from tiny specks to coarse flecks |
roid calcifications. Positioning the thyroid at |
nodules that have undergone regressive |
of calcification and vary markedly in their |
the center of the image can help to avoid this |
change. They appear sonographically as high- |
shape and conspicuity. Air echoes from the |
confusion (Fig.14.56). |
amplitude echoes with acoustic shadows. They |
trachea may occasionally be mistaken for thy- |
|
Fig. 14.56 Regressive calcification of the thyroid gland. a Some small calcification with shadowing in a goiter. AC = common carotid artery.
b Calcification in the right thyroid lobe with a dense acoustic shadow (S). Not to be confused with the trachea.
c Broad band of calcification in the left thyroid lobe with acoustic shadows (S).
Irregular
Gland |
Diffuse Changes |
||||
|
|
|
|||
|
|
|
|
Circumscribed Changes |
|
|
|
|
|
||
Thyroid |
|
|
Anechoic |
||
|
|
Hyperechoic |
|||
|
|
|
|
|
Hypoechoic |
|
|
|
|
|
Isoechoic |
|
|
|
|
|
Irregular |
|
|
|
|
|
|
|
|
|
Differential Diagnosis of Hyperthyroidism |
||
|
|
|
|||
Nodular Goiter
Regressive Nodular Goiter
Tumor
Nodular Goiter
A nodular goiter generally develops in the setting of a long-standing diffuse goiter in an io- dine-deficient geographic region. But nodules can form and multinodular goiters can develop even in normal thyroid glands, regardless of iodine intake, as a consequence of heterogeneous thyrocyte populations and genetic cell
changes. This type of goiter is based on true adenomatous growth. For this reason alone, the goal of surgically resecting a nodular goiter is to remove all grossly visible nodules as completely as possible. Although the nodules will still be present after radioiodine treatment, their hyperthyroid activity will be eradicated.
Sonographic features. Ultrasonography is the most sensitive study for delineating nodules.21 A nodular goiter is marked by thyroid enlargement and a disordered or heterogeneous echo structure, depending on how pronounced the regressive changes are. In the ideal case of discrete nodules in a side-by-side arrangement,
502

14
Fig. 14.57 Nodular goiter. The individual adenomatous nodules (A) are clearly delineated by their hypoechoic rims.
the nodular goiter is easily recognized at ultrasound by the halos that surround the nodules. Frequently, however, the nodules are confluent and of variable size, making it extremely difficult to delineate them in the B-mode image.
Fig. 14.58 Nodular goiter (TH).
a The adenomatous nodules (AN) are partially confluent.
Only color Doppler can define individual nodules in these cases (Figs. 14.57, 14.58, 14.59). It is virtually impossible, however, to distinguish autonomous nodules with ultrasound. Patients with multiple thyroid nodules have the same
Circumscribed Changes
b When viewed with color Doppler, however, the nodules are individually defined by their scalloped margins. On the whole, the thyroid appears hypoechoic to the adjacent muscle (M).
Fig. 14.59 Nodular giant goiter.
a Diffuse hyperechoic structure without detectable nodules. Volume measurement by the curved probe.
b CDS: irregular vessel structure, incomplete outlined vascular rim.
risk of malignancy. Sonographic characteristics are superior to nodule size for identifying malignant nodules.
Regressive Nodular Goiter
Nodular Goiter 






















The ultrasound appearance of a long-standing nodular goiter becomes increasingly difficult to interpret over time. The already diverse sonomorphologic features of nodules are made more complex by the addition of regressive changes such as cystic transformation, hyperechoic collagenous connective tissue, hypoechoic hyaline connective tissue, and microcalcifications or macrocalcifications, which create an extremely heterogeneous appearance (Fig. 14.60, Fig. 14.61).
Fig. 14.60 Regressive nodular goiter. SieScape panoramic image shows an irregular thyroid structure with anechoic inclusions (cysts), hyperechoic areas (collagenous connective tissue), and hypoechoic elements (blood vessels, hyaline connective tissue?).
Fig. 14.61 Amyloidosis of the thyroid. a Right lobe.
b Left lobe, CDS: enlarged, swollen thyroid, slightly inhomogeneous structure and diminished vascularization (AA—amyloid with kidney and intestinal involvement in Mediterranean fever).
503