

Atrial Fibrillation- Anticoagulation
.pdfAtrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
CCS guidelines
•Compared to placebo/control,
the risk reduction with warfarin is 64%
•Patients need anticoagulants if they have AF
31Based on Hart Ann Int Med 1999; 131: 492
It is a mistake to use antiplatelet agents for AF
•The elderly benefit from anticoagulation more than younger patients1, 2
•It would take 295 falls to equal the risk of not anticoagulating in AF3
•Risk of serious bleeding is not higher on anticoagulation than on antiplatelet agents4
1. van Walraven C, et al. Stroke. 2009; 40: 1410-6 2. Spence JD. Nat Rev Cardiol. 2009; 6: 448-50
3. Man-Son-Hing M et al. Arch Intern Med 1999; 159: 677–685
324. Flaker GC, et al. Stroke. 2012; 43: 3291-7
Controlling the INR matters
Annual stroke risk
SPORTIF III 2.3%
SPORTIF V 1.16%
P=0.0004
33Hylek EM et al. Stroke 2008; 39: 3009-3014
The screen versions of these slides have full details of copyright and acknowledgements |
11 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
Warfarin is impossible to use well
•In clinical trials, time in target INR only 60%
•In the real world:
‒Only 35% of patients with AF on warfarin
‒Of those only 50% of the time in target INR1
•One trick to reduce INR turbulence is to use a small dose of vitamin K daily2
1. Samsa GP et al. Arch Intern Med 2000; 160: 967–973
342. Rombouts EK et al. J Thromb Haemost 2007; 5: 2043–2048
Drug interactions with warfarin
35Spence JD J Neural Transm 2013; 120: 1447-1451
Real-world warfarin bleeding,
Gomes T et al. CMAJ. 2013; 185: E121-7
The screen versions of these slides have full details of copyright and acknowledgements |
12 |
Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
Under-anticoagulation doesn’t work
•69 yo woman
with mitral stenosis
•Stroke from AF
•INR 1.5 x 22 days
•Surgical removal of thrombus
at day 54
37Tsuda Y et al. Stroke 1990; 21; 1375-1376
Seek AF, and ye shall find it1
In cryptogenic stroke with no AF at baseline
•1-4 months of telephonic ECG turned up AF in 9.2%2
•7-day loop recorder at 0, 3 and 6 months: AF in 26%3
•Continuous monitoring in stroke unit better than Holter4
•30-day monitoring 11%5
•EMBRACE study 3% on Holter, 16% long-term (30 day)
•Implantable monitor 3 years: 23%
1.Tayal AH, Callans DJ. Neurology 2010; 74: 1662–1663
2.Gaillard N et al. Neurology 2010; 74: 1666–1670
3.Wallman D et al. Stroke 2007; 38: 2292–2294
4.Rizos T et al. Stroke. 2012; 43: 2689-2694
385. Flint AC et al. Stroke. 2012; 43: 2788-2790
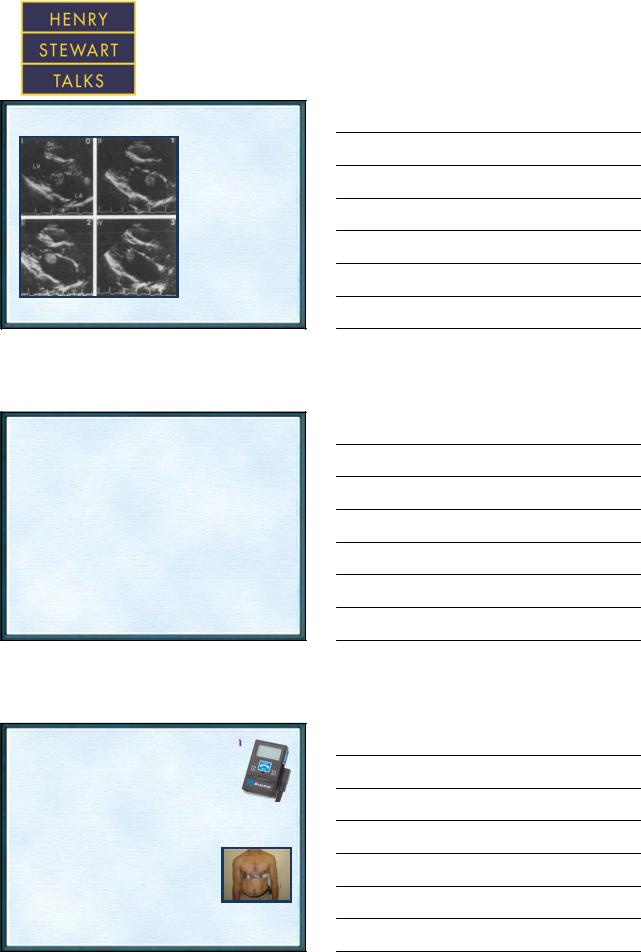
EMBRACE study intervention
•Event-triggered loop recorder (Braemar Inc., ER910AF)
–Automatically records AF
–Memory storage capacity: 30 minutes
–Programmed to record up to 11 events, max. 2.5 minutes per event
•Accuheart electrode belt (Cardiac Bio-Systems Inc.)
–Dry electrode technology (without adhesive skin-contact electrodes)
•Worn for 30 days or until AF detected
•Data handling
–Recorded data transmitted trans-telephonically to central station
–ECG tracings of all events printed and interpreted centrally by one physician blinded to clinical information
39– Results report sent to patient’s study physician
The screen versions of these slides have full details of copyright and acknowledgements |
13 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
EMBRACE trial
•527 patients with cryptogenic stroke
•Age 73 years; 54% male; automated recorder belt vs. repeat Holter
•At 3 months, 16.1% with AF vs. 3.2% p = 0.001
40Gladstone D et al. N Engl J Med 2014; 370: 2467-77
CRYSTAL AF study
•441 patients with cryptogenic stroke
•63% male, age 61.5 years; implantable device
•6 months rate with an implantable device was ~ 10%
•After 36 months it was just above 30%
•Many patients with cryptogenic stroke in whom we suspect a cardio-embolic stroke, have undetected intermittent AF
41Based on: Sanna T et al. N Engl J Med. 2014; 370: 2478-86
CCS guidelines
The CHADS2 score is useful in deciding which patient needs anticoagulation therapy
•If a patient had a stroke and his CHADS2 score is > 2, he needs anticoagulation therapy
•If the CHADS2 score is 6 the adjusted rate of stroke/year is 18%
•These patients should not get anti-platelet agents
42www.ccs.ca
The screen versions of these slides have full details of copyright and acknowledgements |
14 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
CCS guidelines (2)
Recommendations – antithrombotic for AF
When OAC therapy is indicated, most patients should receive (NOA) in preference to warfarin
(Conditional recommendation. High quality evidence)
43www.ccs.ca
Most thrombi in left atrial appendage
>90% of thrombi in non-valvular AF are in the atrial appendage
44
Other approaches
•Prophylactic removal of atrial appendage during cardiac surgery
•Thoracoscopic removal of LA appendage
•Insertion of device in LA appendage
45Onalan O, Crystal E. Stroke 2007; 38; 624-630
The screen versions of these slides have full details of copyright and acknowledgements |
15 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
Protect - AF trial
• AF patients randomized to conventional warfarin vs. Watchman device
After 900 patient-years:
•32% of primary outcome: absence of ischemic & hemorrhagic stroke, CV /unexplained death, systemic embolism
BUT:
•>25% of patients did not take warfarin
•Implantation only successful in 90%
•12.3% had serious complications
–4 had to have device removed
–2.2% required surgery
–Higher risk in low-volume centres
46Maisel WH. N Engl J Med. 2009 Jun 18; 360(25): 2601-3
PLAATO device
•In feasibility studies n=108
•Successful implantation in 97%;
•65% reduction of stroke
•Trial under way
47Onalan O, Crystal E. Stroke 2007; 38; 624-630
European PLAATO study
180 patients with AF and TIA/Stroke or CHADS > 2 and contraindications to warfarin
•Successful occlusion of atrial appendage in 90%
•2 deaths
•6 cardiac tamponade, 2 requiring surgery
•1 device too small and embolized to aorta; snared successfully
•2.3% strokes per year vs. expected 6.6% for CHADS 2
48Bayard YL et al. EuroIntervention. 2010 Jun; 6(2): 220-6
The screen versions of these slides have full details of copyright and acknowledgements |
16 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
New era in anticoagulation
 Intracranial bleeding?
Intracranial bleeding?
Apixaban
Rivaroxaban
Dabigatran
49Atarashi H. Circ J. 2011; 75: 1819-20
Novel oral anticoagulants – pharmacological properties
Characteristic |
Rivaroxaban1 |
Dabigatran2 |
Apixaban3 |
Target |
Factor Xa |
Factor IIa |
Factor Xa |
Prodrug |
No |
Yes |
No |
|
|
|
|
Dosing |
OD |
BID |
BID |
|
|
|
|
Bioavailability, % |
80-100%* |
6.5% |
50% |
|
|
|
|
Half-life |
5-13h |
12-14 h |
8-15 h |
Renal clearance |
|
|
|
(unchanged |
~33% |
85% |
~25%4† |
bioavailable drug) |
|
|
|
Cmax |
2-4 h |
1-2 h |
3-4 h |
|
|
|
|
|
Strong inhibitors |
|
Strong inhibitors |
Drug interactions |
of both CYP3A4 |
P-gp inhibitors |
of both CYP3A4 and |
|
and P-gp |
|
P-gp |
P-gp = P glycoprotein
501. Xarelto® PM, July 18, 2012; 2. Pradaxa ® PM November 12, 2012;
3. Eliquis® PM November 27, 2012; 4. Goette Trends Cardiovasc Med. 2013; 23: 128-34
Dabigatran vs. warfarin in atrial fibrillation
Risk/year |
Warfarin |
Dabigatran |
Dabigatran |
p |
|
(INR 2-3) |
110 mg |
150 mg |
|
Major |
3.36% |
2.71% |
3.11% |
0.001 |
bleeding |
|
|
|
|
Hemorrhagic |
0.33% |
0.12% |
0.10% |
0.001 |
stroke |
|
|
|
|
Major vasc. |
7.64% |
7.09% |
6.91% |
0.04 |
event, major |
|
|
|
|
bleed, death |
|
|
|
|
n =18,113 Median follow up 2yrs
51Connolly SJ et al. N Engl J Med 2009; 361
The screen versions of these slides have full details of copyright and acknowledgements |
17 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
Dabigatran plasma concentration and outcomes
52Reilly PA et al. J Am Coll Cardiol. 2014; 63: 321-8
Therapeutic range for dabigatran
53Reilly PA et al. J Am Coll Cardiol. 2014; 63: 321-8
New oral anticoagulants: total drug exposure
(AUC) with declining renal function
Rivaroxaban |
Dabigatran |
Apixaban |
(33% cleared renally*)1 |
(85% cleared renally)2 |
(40-50% cleared renally†)3 |
AUC ratio vs. Normal renal function
1. Xarelto® PM, July 18, 2012; 2. Pradaxa ® PM November 12, 2012; 3. Goette Trends Cardiovasc Med. 542013 [Epub ahead of print]; 4. Eliquis® PM November 27, 2012
The screen versions of these slides have full details of copyright and acknowledgements |
18 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
Need for blood levels of dabigatran
•Only 3-7% bioavailable
•Subject to large effects of:
–Drug interaction
–Renal function
55Moore TJ et al. BMJ 2014; 349: g4517
Rivaroxaban vs. warfarin in AF
•Stroke or systemic embolism occurred in:
–188 patients in the rivaroxaban group (1.7% per year)
–241 patients in the warfarin group (2.2% per year)
(hazard ratio in the rivaroxaban group, 0.79;
95% confidence interval [CI], 0.66 to 0.96; P<0.001 for noninferiority)
1 outcome HR 0.79 p=0.001
|
Riva |
Warf |
|
Fatal bleeding |
0.2% |
0.5% |
p=0.003 |
Intracranial Bleeding |
0.5% |
0.7% |
p=0.03 |
|
N= 14,264 |
|
56 |
INR therapeutic 55% |
|
of the time |
||
Rocket trial. Patel MR et al. N Engl J Med. 2011; 365: 883-91 |
||
|
Apixaban vs. warfarin in AF
•The primary outcome of stroke or systemic embolism:
–212 patients in the apixaban group (1.27% per year)
–265 patients in the warfarin group (1.60% per year)
(hazard ratio in the apixaban group, 0.79; 95% confidence interval [CI], 0.66 to 0.95;
P<0.001 for noninferiority and P = 0.01 for superiority)
•Major bleeding (defined according to ISTH criteria):
–327 patients in the apixaban group (2.13% per year)
–462 patients in the warfarin group (3.09% per year)
(hazard ratio, 0.69; 95% CI, 0.60 to 0.80; P<0.001)
57Aristotle trial. Granger CB et al. N Engl J Med 2011; 365: 981-92
n= 18,201 |
|
CHADS2 score |
|
Apixa |
Warf |
Mean 2.1±1.1 |
2.1±1.1 |
INR therapeutic 62.2% of time
The screen versions of these slides have full details of copyright and acknowledgements |
19 |

Atrial Fibrillation, Anticoagulation
and Vitamins for Homocysteine
Prof. J. David Spence M.D.
ICH in ROCKET
58Hankey GJ et al. Stroke 2014; 45: 1304-1312
New oral anticoagulants vs. warfarin in atrial fibrillation; apixaban, dabigatran, rivaroxaban
|
|
Outcomes |
|
Weighted event rates |
At a median 657 to 730 d |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
NOA |
War |
RRR (95% CI) |
|
|
|
|
|
|
|
|
|
|
Stroke and systemic embolism |
|
2.7% |
3.5% |
22% (8 to 33) |
|
|
|
|
|
|
|
|
|
|
|
Ischemic or unspecified stroke |
|
1.9% |
2.2% |
13% (1 to 23) |
|
|
|
|
|
|
|
|
|
|
|
Hemorrhagic stroke |
|
|
0.4% |
0.8% |
55% (32 to 69) |
|
|
|
|
|
|
|
|
|
|
All-cause mortality |
|
|
5.6% |
6.3% |
12% (5 to 18) |
|
|
|
|
|
|
|
|
|
|
Vascular mortality |
|
|
3.4% |
3.9% |
13% (2 to 23) |
|
|
|
|
|
|
|
|
|
|
Myocardial infarction |
|
|
1.3% |
1.4% |
4% (−26 to 27) |
|
|
|
|
|
|
|
|
|
|
Major bleeding |
|
|
5.0% |
5.7% |
12% (−9 to 29) |
|
|
|
|
|
|
|
|
|
|
Intracranial bleeding |
|
|
0.7% |
1.3% |
51% (34 to 64) |
|
|
|
|
|
|
|
|
|
|
Gastrointestinal bleeding |
|
|
2.2% |
1.8% |
RRI 25% (−9 to 72) |
|
|
59 |
|
|
|
|
|
|
157 |
(6): JC3-2 |
|
|
|||
Klein L. Ann Intern Med. 2012 Sep 18; |
|
|
|
|
|||
Reversal of Xa inhibitor
with prothrombin complex concentrate (PCC)
|
PT |
|
|
ETP |
|
|
Seconds |
|
|
Percentages (%) |
|
|
|
|
Time |
Placebo |
|
Time |
Placebo |
|
Rivaroxaban |
PCC or placebo |
Rivaroxaban |
|
|||
|
PCC or placebo |
|
||||
20mg BID |
infusion |
PCC |
PCC |
|||
20mg BID |
infusion |
|||||
for two |
|
|
|
|||
|
|
for two |
|
|
||
and a half days |
|
|
|
|
||
|
|
and a half days |
|
|
||
|
|
|
|
|
60Eerenberg ES et al. Circulation. 2011; 124: 1573-9
The screen versions of these slides have full details of copyright and acknowledgements |
20 |