



252 |
BRS Physiology |
Ingested
Ca2+
1,25-Dihydroxycholecalciferol
+
Absorption |
|
Bone formation |
|
|
ECF |
|
|
|
Ca2+ |
|
|
Secretion |
|
Bone resorption |
|
|
|
+ |
|
Filtration |
Reabsorption |
– |
|
|
+ |
PTH, |
|
Fecal |
1,25-Dihydroxycholecalciferol |
||
|
Ca2+ |
|
Calcitonin |
|
PTH |
|
|
|
Urinary Ca2+ excretion
Figure 7.13 Hormonal regulation of Ca2+ metabolism. ECF = extracellular fluid; PTH = parathyroid hormone.
1. Positive Ca2+ balance
■is seen in growing children.
■Intestinal Ca2+ absorption exceeds urinary excretion, and the excess is deposited in the growing bones.
2. Negative Ca2+ balance
■is seen in women during pregnancy or lactation.
■Intestinal Ca2+ absorption is less than Ca2+ excretion, and the deficit comes from the maternal bones.
B.Parathyroid hormone (PTH)
■is the major hormone for the regulation of serum [Ca2+].
■is synthesized and secreted by the chief cells of the parathyroid glands.
1. Secretion of PTH
■is controlled by the serum [Ca2+] binding to Ca2+-sensing receptors in the parathyroid cell membrane. Decreased serum [Ca2+] increases PTH secretion, whereas increased serum Ca2+ decreases PTH secretion.
■Decreased serum Ca2+ causes decreased binding to the Ca2+-sensing receptor, which stimulates PTH secretion.
■Mild decreases in serum [Mg2+] stimulate PTH secretion.
■Severe decreases in serum [Mg2+] inhibit PTH secretion and produce symptoms of hypoparathyroidism (e.g., hypocalcemia).
■The second messenger for PTH secretion by the parathyroid gland is cAMP.
2. Actions of PTH
■are coordinated to produce an increase in serum [Ca2+] and a decrease in serum
[phosphate].

|
Endocrine Physiology |
253 |
Chapter 7 |
■ The second messenger for PTH actions on its target tissues is cAMP.
a. PTH increases bone resorption, which brings both Ca2+ and phosphate from bone mineral into the ECF. Alone, this effect on bone would not increase the serum ionized [Ca2+] because phosphate complexes Ca2+.
■Resorption of the organic matrix of bone is reflected in increased hydroxyproline excretion.
b. PTH inhibits renal phosphate reabsorption in the proximal tubule and, therefore, increases phosphate excretion (phosphaturic effect). As a result, the phosphate resorbed from
bone is excreted in the urine, allowing the serum ionized [Ca2+] to increase.
■cAMP generated as a result of the action of PTH on the proximal tubule is excreted in the urine (urinary cAMP).
c. PTH increases renal Ca2+ reabsorption in the distal tubule, which also increases the serum [Ca2+].
d. PTH increases intestinal Ca2+ absorption indirectly by stimulating the production of 1,25-dihydroxycholecalciferol in the kidney (see VII C).
3. Pathophysiology of PTH (Table 7.12) a. Primary hyperparathyroidism
■is most commonly caused by parathyroid adenoma.
■is characterized by the following:
(1) ↑ serum [Ca2+] (hypercalcemia)
(2) ↓ serum [phosphate] (hypophosphatemia)
(3) ↑ urinary phosphate excretion (phosphaturic effect of PTH)
(4) ↑ urinary Ca2+ excretion (caused by the increased filtered load of Ca2+)
(5) ↑ urinary cAMP
(6) ↑ bone resorption
|
|
|
|
|
|
||
t a b l e |
7.12 |
Pathophysiology of PTH |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
1,25-Dihydroxy |
|
|
Serum [Ca2+] |
|
Disorder |
PTH |
cholecalciferol |
Bone |
Urine |
Serum [P] |
||
Primary |
↑ |
↑ (PTH stimulates |
↑ Resorption |
↑ P excretion |
↑ |
↓ |
|
hyperparathyroidism |
|
1α-hydroxylase) |
|
(phosphaturia) |
|
|
|
|
|
|
|
|
↑ Ca2+ excretion |
|
|
|
|
|
|
|
(high filtered |
|
|
|
|
|
|
|
load of Ca2+) |
|
|
|
|
|
|
|
↑ urinary cAMP |
|
|
Humoral hypercalcemia |
↓ |
— |
↑ Resorption |
↑ P excretion |
↑ |
↓ |
|
of malignancy |
|
|
|
|
|
|
|
Surgical |
↓ |
↓ |
↓ Resorption |
↓ P excretion |
↓ |
↑ |
|
hypoparathyroidism |
|
|
|
↓ urinary cAMP |
|
|
|
Pseudohypopara |
↑ |
↓ |
↓ Resorption |
↓ P excretion |
↓ |
↑ |
|
thyroidism |
|
|
(defective Gs) |
↓ urinary cAMP |
|
|
|
|
|
|
|
|
(defective Gs) |
|
|
Chronic renal failure |
↑ (2°) ↓ (caused by |
Osteomalacia |
↓ P excretion |
↓ (caused by |
↑ (caused |
||
|
|
|
renal failure) |
(caused by |
(caused by |
↓ 1,25-dihydroxy |
by ↓ P |
|
|
|
|
↓ 1,25-dihydroxy |
↓ GFR) |
cholecalciferol) |
excretion) |
|
|
|
|
cholecalciferol) |
|
|
|
↑ Resorption (caused by ↑ PTH)
cAMP = cyclic adenosine monophosphate; GFR = glomerular filtration rate. See Table 7.1 for other abbreviation.

254Brs Physiology
b. Humoral hypercalcemia of malignancy
■is caused by PTH-related peptide (PTH-rp) secreted by some malignant tumors (e.g.,
breast, lung). PTH-rp has all of the physiologic actions of PTH, including increased bone resorption, increased renal Ca2+ reabsorption, and decreased renal phosphate reabsorption.
■is characterized by the following:
(1) ↑ serum [Ca2+] (hypercalcemia)
(2) ↓ serum [phosphate] (hypophosphatemia)
(3) ↑ urinary phosphate excretion (phosphaturic effect of PTH-rp)
(4) ↓ serum PTH levels (due to feedback inhibition from the high serum Ca2+) c. Hypoparathyroidism
■ is most commonly a result of thyroid surgery, or it is congenital. ■ is characterized by the following:
(1) ↓ serum [Ca2+] (hypocalcemia) and tetany
(2) ↑ serum [phosphate] (hyperphosphatemia)
(3) ↓ urinary phosphate excretion
d. Pseudohypoparathyroidism type Ia—Albright hereditary osteodystrophy
■ is the result of defective Gs protein in the kidney and bone, which causes end-organ resistance to PTH.
■Hypocalcemia and hyperphosphatemia occur (as in hypoparathyroidism), which are not correctable by the administration of exogenous PTH.
■Circulating PTH levels are elevated (stimulated by hypocalcemia).
e.Chronic renal failure
■Decreased glomerular filtration rate (GFR) leads to decreased filtration of phosphate, phosphate retention, and increased serum [phosphate].
■Increased serum phosphate complexes Ca2+ and leads to decreased ionized [Ca2+].
■Decreased production of 1,25-dihydroxycholecalciferol by the diseased renal tissue also contributes to the decreased ionized [Ca2+] (see VII C 1).
■Decreased [Ca2+] causes secondary hyperparathyroidism.
■The combination of increased PTH levels and decreased 1,25-dihydroxycholecalcif- erol produces renal osteodystrophy, in which there is increased bone resorption and osteomalacia.
f.familial hypocalciuric hypercalcemia (fHH)
■autosomal dominant disorder with decreased urinary Ca2+ excretion and increased serum Ca2+
■caused by inactivating mutations of the Ca2+-sensing receptors that regulate PTH secretion.
C.vitamin D
■provides Ca2+ and phosphate to ECF for bone mineralization.
■In children, vitamin D deficiency causes rickets.
■In adults, vitamin D deficiency causes osteomalacia.
1.vitamin D metabolism (Figure 7.14)
■ Cholecalciferol, 25-hydroxycholecalciferol, and 24,25-dihydroxycholecalciferol are inactive.
■ The active form of vitamin D is 1,25-dihydroxycholecalciferol.
■ The production of 1,25-dihydroxycholecalciferol in the kidney is catalyzed by the
enzyme 1α-hydroxylase.
■ 1a-hydroxylase activity is increased by the following:
a.↓ serum [Ca2+]
b.↑ PTH levels
c.↓ serum [phosphate]


 [Ca
[Ca [phosphate]
[phosphate]
256 |
Brs Physiology |
|
Male |
|
Female |
|
XY |
|
XX |
|
Testes |
|
Ovaries |
Sertoli |
|
Leydig |
|
cells |
|
cells |
|
Anti-müllerian |
Testosterone |
No anti-müllerian hormone |
|
hormone |
|
|
No testosterone |
Male phenotype |
|
Female phenotype |
|
fIGUre 7.15 Sexual differentiation in males and females.
B.female phenotype
■The ovaries of gonadal females secrete estrogen, but not anti-müllerian hormone or testosterone.
■Without testosterone, the wolffian ducts do not differentiate.
■Without anti-müllerian hormone, the müllerian ducts are not suppressed and therefore develop into the female internal genital tract.
Ix. mAle rePrODUCTIOn
A.synthesis of testosterone (figure 7.16)
■Testosterone is the major androgen synthesized and secreted by the leydig cells.
■Leydig cells do not contain 21β-hydroxylase or 11β-hydroxylase (in contrast to the adrenal cortex) and, therefore, do not synthesize glucocorticoids or mineralocorticoids.
■LH (in a parallel action to ACTH in the adrenal cortex) increases testosterone synthesis by stimulating cholesterol desmolase, the first step in the pathway.
■Accessory sex organs (e.g., prostate) contain 5a-reductase, which converts testosterone to its active form, dihydrotestosterone.
■5a-reductase inhibitors (finasteride) may be used to treat benign prostatic hyperplasia because they block the activation of testosterone to dihydrotestosterone in the prostate.
B.regulation of testes (figure 7.17)
1.Hypothalamic control—GnrH
■Arcuate nuclei of the hypothalamus secrete GnRH into the hypothalamic–hypophysial portal blood. GnRH stimulates the anterior pituitary to secrete FSH and LH.
2.Anterior pituitary—fsH and lH
■fsH acts on the sertoli cells to maintain spermatogenesis. The Sertoli cells also secrete inhibin, which is involved in negative feedback of FSH secretion.
■lH acts on the leydig cells to promote testosterone synthesis. Testosterone acts via an intratesticular paracrine mechanism to reinforce the spermatogenic effects of FSH in the Sertoli cells.

 Dihydrotestosterone
Dihydrotestosterone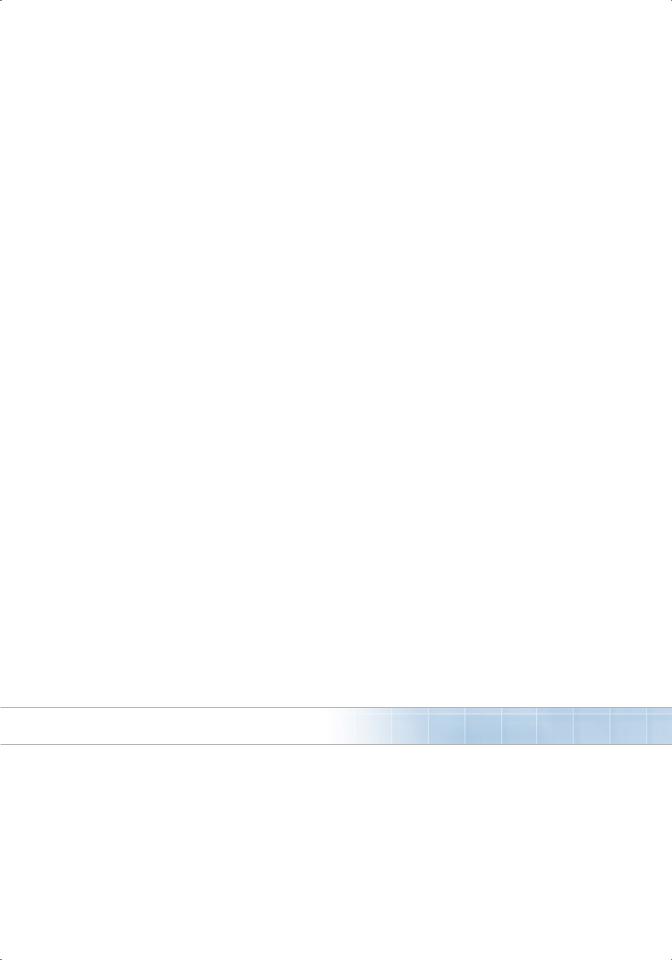
258Brs Physiology
3.negative feedback control—testosterone and inhibin
■Testosterone inhibits the secretion of lH by inhibiting the release of GnRH from the hypothalamus and by directly inhibiting the release of LH from the anterior pituitary.
■Inhibin (produced by the Sertoli cells) inhibits the secretion of fsH from the anterior pituitary.
C.Actions of testosterone or dihydrotestosterone
1.Actions of testosterone
■Differentiation of epididymis, vas deferens, and seminal vesicles
■Pubertal growth spurt
■Cessation of pubertal growth spurt (epiphyseal closure)
■Libido
■Spermatogenesis in Sertoli cells (paracrine effect)
■Deepening of voice
■Increased muscle mass
■Growth of penis and seminal vesicles
■Negative feedback on anterior pituitary
2.Actions of dihydrotestosterone
■Differentiation of penis, scrotum, and prostate
■Male hair pattern
■Male pattern baldness
■Sebaceous gland activity
■Growth of prostate
3.Androgen insensitivity disorder (testicular feminizing syndrome)
■is caused by deficiency of androgen receptors in target tissues of males.
■Testosterone and dihydrotestosterone actions in target tissues are absent.
■There are female external genitalia (“default”), and there is no internal genital tract.
■Testosterone levels are elevated due to lack of testosterone receptors in the anterior pituitary (lack of feedback inhibition).
D.Puberty (male and female)
■is initiated by the onset of pulsatile GnrH release from the hypothalamus.
■FSH and LH are, in turn, secreted in pulsatile fashion.
■GnRH up-regulates its own receptor in the anterior pituitary.
e.variation in fsH and lH levels over the life span (male and female)
1.In childhood, hormone levels are lowest and FSH > LH.
2.At puberty and during the reproductive years, hormone levels increase and LH > FSH.
3.In senescence, hormone levels are highest and FSH > LH.
x. femAle rePrODUCTIOn
A.synthesis of estrogen and progesterone (figure 7.18)
■Theca cells produce testosterone (stimulated at the first step by LH). Androstenedione diffuses to the nearby granulosa cells, which contain 17β-hydroxysteroid dehydrogenase,
which converts androstenedione to testosterone, and aromatase, which converts testosterone to 17β-estradiol (stimulated by FSH).
B.regulation of the ovary
1. Hypothalamic control—GnrH
■ As in the male, pulsatile GnRH stimulates the anterior pituitary to secrete FSH and LH.