

If asleep, blood runs down on both sides of the neck and collects behind the neck and shoulder; stains found on both palms, for the victim attempts to cover the wound.
May be cut corresponding in position to those in the body; disarrangement, tears and loss of buttons. Disturbance at the scene\ such as dis¬arrangement of furniture in a room; trampling and crushing of vegetable matter and shrubs, or' confused foot¬prints outside.
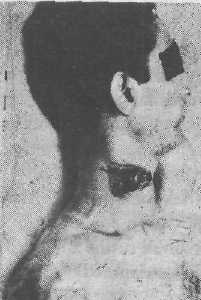
Fig. (8-7). Suicidal cut-throat with hesitation marks.

Fig. (8-8). Homicidal cut-throat wound.
Circumstances of Incised Injuries : Suicide:
The important features of self-inflicted wounds are:
(1) They are multiple and parallel or nearly so, in
any one area. (2) They are uniform in depth and
direction. (3) They are relatively minor. (4) The fatal
wounds are present on several limited accessible
areas of the body, such as front of the neck, wrists,
groin, and occasionally on the back of legs or on
chesu(5) Hesitation marks or tentative cuts or
trial wounds: They are cuts which are multiple,
small and superficial often involving only the skin
and are seen at the beginning of the incised wound.
The sites of election of suicidal incised
wounds are: throat, wrist and front of chest. When
preliminary incisions are inflicted with some violence
they may be few, but commonly they are superficial
and multiple. The fatal incisions are usually made
with great violence, and the large gaping wound
produced by suicide should not be mistaken for
homicidal wounds. When a safety razor blade is
used, unintentional cuts are found on the fingers,
where the blade has been gripped. Suicidal incised
wounds of extremities are usually found on the
flexor surface of the wrists, outer side of the left
arm, and forearm, the front and outer side of the
thighs, and the front of the abdomen and chest. Fatal
Incised wounds of the arms are almost always
suicidal. Suicidal wounds of chest are usually on
(he left side and directed downwards and inwards.
A wound caused by running on knife tends to be
more horizontal in direction. A person who commits
suicide usually exposes the portion of the body to
be incised, e.g. he may open his collar before cutting
his throat, or pull up his shirt before cutting his chest
or abdomen. Suicides usually do not injure the face.
Homicidal wounds: They are usually multiple
and can occur in any region of the body. Wounds
of the chest are usually present over a wider area
and are more horizontal. They may be directed from
below upwards which is rarely seen in suicidal
wounds. Incised wounds situated on the back, or
in such a position as cannot be easily reached by
a suicide, are homicidal. Incised wounds on nose,
ears and genitals are usually homicidal, and are
inflicted; on account of jealousy or revenge in cases
of adultery, causing disfiguration. Cut-throat wounds
cause immediate death from haemorrhage, air
embolism, or inhalation of effused blood into the respiratory tract.
Accidental incised wounds may be caused by falling upon a sharp-cutting weapon held in the hand, or upon a sharp-pointed object or by a sharp piece of broken glass. They may be situated anywhere on the body, but are commonly seen about the hands.
Some mentally disordered persons may inflict hundreds of small wounds upon themselves. A knife, razor or broken glass may be used and a large number of cuts produced on the arms which may cross each other in groups. Small stabs may be produced on the chest or temples. Paranoid schizophrenics with a strong religious flavour to their delusions may remove penis, scrotum, and testes. Ears and nose may be mutilated.
In a decomposed body, it is difficult to differentiate a laceration from an incised wound. When a body with incised wounds or lacerations is immersed in water soon after infliction of injuries, the blood in the wounds is lysed by water and passes into the water, and whether the injuries are antemortem or postmortem cannot be made out.
CHOP WOUNDS : They are deep gaping wounds caused by a blow with the sharp-cutting edge of a fairly heavy weapon, like a hatchet, an axe, machete sabre, or meat cleaverJThe dimensions of the wound correspond to cross-section of penetrating blade. The margins are sharp and may show slight abrasion and bruising with marked destruction of underlying organs. If the edge is blunt, the margins are ragged and bruised. Undermining occurs in the direction towards which the chop is made. When the whole blade strikes the body at the same time, the depth may be same throughout the wound. Usually the lower end (heel) of the axe strikes the surface first, which produces a deeper wound than the upper (toe) end. The deeper end indicates the position of the assailant. In the skull, the undermined edge of the fracture defect is the direction in which the force is exerted, and the slanted edge is the side from which the force was directed. In case of long bones, the bone fragments get loosened on the opposite side of the force. A twisting force, after the chopping weapon has been embedded in bone, and as it is being
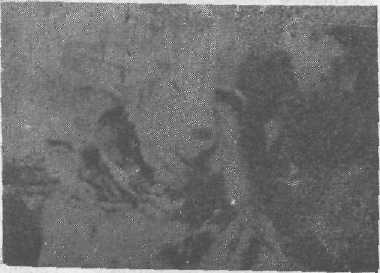
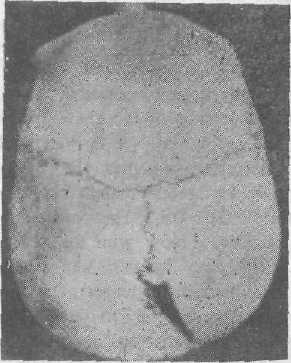
Fig. (8-10). Cut injury of the skull. The wide gap anteriorly is caused by the heel of the axe in a frontal attack.
removed can cause splintering of the bone, particularly near the ends of the chop wound. If the extremities are attacked, there may be complete or incomplete amputation of the fingers or other bones, and the joints may be separated or disarticulated. Wounds on the head and trunk are usually associated with injuries to important structures and are fatal. The cranium may be depressed, but if the weapon strikes obliquely, a piece of the skull may be removed. The neck may be almost completely separated.
Most of these injuries are homicidal and usually inflicted on the exposed portions of the body like the head, face, neck, shoulders and extremities.
Accidental injuries are caused by power fans, band saws or ship or airplane propellers, which may lacerate the soft tissues extensively or amputate parts of the body. Suicidal chop injuries are very rare.
STAB OR PUNCTURED WOUNDS
A stab wound is produced from penetration by long narrow instruments with blunt or pointed ends, such as knife, dagger, nail, needle, spear. arrow, screw driver, etc. into the depths of the body. penetrating the skin and the underlying tissues, thai is deeper than its length and width on skin.*i This can occur by driving the object into the body, or from the body's pressing or falling against the object The most common stabbing instruments are kitchen knives, sheath knives or pen-knives. They are called penetrating wounds, when they enter a cavity of body. When the weapon enters the body on one side and comes out from the other side, perforating wounds or through-and-through puncture wounds are produced. The wound of entry is larger with inverted edges, and the wound of exit is smaller with everted edges, due to tapering of blade. The victim of a fatal penetrating injury may not show signs and symptoms of injury until many hours have passed. Characters : (1) Margins: The edges of the wound are clean-cut. There is usually no abrasion or bruising of the margins, but in full penetration of the blade, abrasion and bruising may be produced by the hilt-guard (metal piece between the blade and handle) striking the skin?)The margins may be abraded, and ragged if the cutting edge is blunt. The mark will be symmetrical, if the knife,strikes the skin at right angle. If the knife strikes in a downward angle, the mark will be prominent above the stab wound, and if the knife strikes in an upward angle, the abrasion will be below the stab wound. In oblique stab wounds, a knife striking from the right will have an abrasion on the right side and vice versa. In such cases, the suspected knife should be examined to determine the compatibility of the shape of the abrasion around the stab wound, with the handle of the knife in question.
(2) Length : The length of the wound is slightly less than the width of the weapon up 10 which it has been driven in, because of stretching of the skin^ For measuring the length of stab wound, the edges of the wound should be brought together. Deliberate lateral, forward, or backward movemenl
of the weapon during its withdrawal from the body lends to widen the wound, and the length will be more lhan the maximum width of the blade. If (he instrument is thrust in, and is then completely withdrawn with the cutting edge dragging against one end, the wound would be extended superficially, producing a tail.
(3) \Viclth : By examining multiple stab
wounds in the body, the length and width of the
knife blade can be determined approximately. The
maximum possible width of the knife blade can be
approximately determined if the edges of a gaping
wound are brought together. Elasticity or laxness
of [he skin can change the width by one to two
millimeters. A stab wound inflicted when the skin
is stretched will be long and thin, which becomes
shorter and broader when the skin is relaxed.
(4) Depth : The depth (length of track) is
greater than the width and length of the external
injury. It is not saf$ to find out the depth of a stab
wound by introducing a probe, because it may
disturb a loose clot and may lead to fatal haemorrhage,
or cause serious damage and may produce multiple
erroneous wound tracks. The depth of a stab wound
is usually equal to, or less than the length of the
blade that was used in producing it, but on yielding
surfaces like the anterior abdominal wall, the depth
of the wound may be greater, because the force
of the thrust may press the tissues underneath. In
young persons the chest is mobile and may be
compressed during the stabbing. Expansion and
retraction of the chest during breathing must also
be considered. Many of the internal organs are not
fixed but have a variable degree of mobility. This
should be taken into account when estimating the
depth of the wounds. After the withdrawal of the
weapon, the wound tends to close by expansion of
[lie tissues along the track. Hie depth should be
determined in the operation theatre when the wound