

Theories of pain The Gate Control Theory of Pain
In the 1960s, two scientists, called Ronald Melzack and Patrick Wall, carried out research to understand pain systems. They developed the Gate Control Theory of Pain.
According to this theory, there are ‘gates’ in the nerve junctions, spinal cord and pain centres in the brain. These gates open and let pain messages through the pain system, so that we feel pain. They can also close to stop messages going through the system, so that the pain is reduced or stopped.
In the 1970s, it was discovered that the body can make its own pain-relief chemicals. These are called endorphins and they work like the pain-relieving drug, morphine. The endorphins can help close the gate. This may explain why some athletes sometimes do not feel pain, even when they are stretching themselves to the limit while doing their sport. Physical activity increases endorphin levels in the body, giving a feeling of well-being and helping to close the pain gate.
In chronic pain there are no treatments that can shut the gate and keep it closed all the time. However, there are ways to close the gate as much as possible so that fewer pain messages pass through the pain system. The brain can focus on very distracting activities. So, for example, someone scoring a winning goal, can have a painful muscle injury and not be aware of much pain.
You can use the skills described in Part Two of this book to gain some control over how much the gate is open or closed. In this way, pain can become more manageable and your life more active.
Other theories of pain
Our understanding about chronic pain and theories about its development are constantly changing. One emerging theory is based on the neuromatrix. This theory helps explain the complex changes that occur in the body’s nerve and sensory system for pain as these systems adapt and evolve to deal successfully with threats. This newer theory helps us understand further why getting good pain relief is so difficult. It explains why there are many different problems in different sites, including the brain’s centres for processing and interpreting pain messages. This theory likens the brain’s pain centres to an orchestra, with different groups of instruments trying to play music without a conductor. It highlights the importance of developing coping skills to manage your activities, moods and unhelpful thinking so that you are in control of the pain and independent, and the pain is not in control of you.
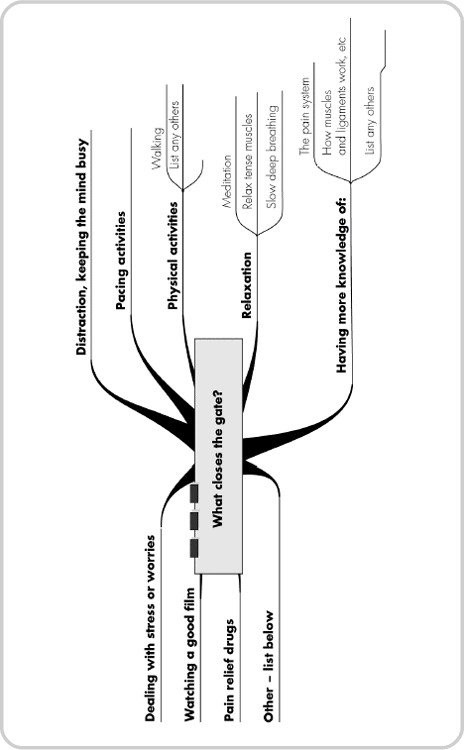
WHAT CLOSES THE GATE AND STOPS PAIN?
Circle those things or activities that you know affect your own gate and add more if you can on page 48.
WHAT OPENS THE GATE AND LETS PAIN THROUGH?
Circle those things or activities that you know affect your own gate and add more if you can.

WHAT OTHER PARTS OF THE BODY CAN SEND PAIN MESSAGES?
The human body is a complex, tough structure, designed to heal itself while still being active. Our bodies are made up of tissues that help them to move: bones, joints and cartilage; muscles and tendons; ligaments; nerves and nerve receptors; and blood vessels.
• Bones are strong supporting structures, linked to each other by thick, strong, elastic tissues called ligaments.
• Joints are places where two bones meet (for example, the shoulder joint, which allows big movements in many directions). Other joints move in fewer directions (like the knee joint, which moves in just two directions).
• Cartilage lines the ends of the long bones, e.g. the thigh bone, and helps with smooth movement during activity.
• Muscles provide power to move the body via joints and to keep it upright. Muscles are very strongly fixed to the bones and around joints by tendons. There are many large and small muscles in the body that are arranged in layers, a bit like an onion.
WHAT HAPPENS TO THESE TISSUES WHEN THEY ARE INJURED?
Following injury, muscles become tight to protect the body and prevent movement for a short time – perhaps hours or days. This helps the body’s healing process.
In chronic pain, when the pain does not reduce, then muscles may stay very tense. The person may be fearful of the pain and avoid being active and stretching. Gradually, over several days and weeks, the muscles, together with the ligaments and tendons, become short and stiff and feel very tight.
The vicious circle shown overleaf may help to explain why people often say, for instance, ‘the pain started in my lower arm and has now gone into other areas’.