


The Eye and Vision |
|
5 |
|
||
|
|
|
•Be impact resistant.
•Have thin metal frames (minimum obstruction of the visual field).
•Be coated with polycarbonate for strength.
•Be of good optical quality.
•Have a luminance transmittance of 10-15%.
•Have appropriate filtration characteristics.
Pilots are strongly advised to avoid using cheap sunglasses as they can allow the light to be over diffused across the eye thus causing perceptional problems in flight. The use of Polaroid sunglasses should be avoided since problems can occur when used with laminated aircraft windscreens.
Light sensitive lenses (photochromic) are also generally forbidden for use in flight due to the time taken for the lens to clear when moving from a bright situation to one of low light. This delay may significantly reduce visual acuity at a critical time.
Polarised lenses reduce the amount of light passing through the lens by selective filtering of certain electromagnetic spectral planes. These lenses can cause distortion patterns from certain laminated cockpit windshields. They can also alter cloud appearance and reduce ground reflections useful for VFR pilots. The use of these sunglasses is therefore discouraged.
Eye Movement
Movement of the eye is achieved by 6 extraocular muscles that allow movement in two planes; up/down and left/right. Normally both eyes move together to view an object. The surface of the eye is lubricated by a liquid secreted by the lacrimal glands. Tears are drained by the tear ducts into the nose. At low humidity levels the eyes can become dry and may feel painful. Tears also have a slight antiseptic property.
Visual Defects
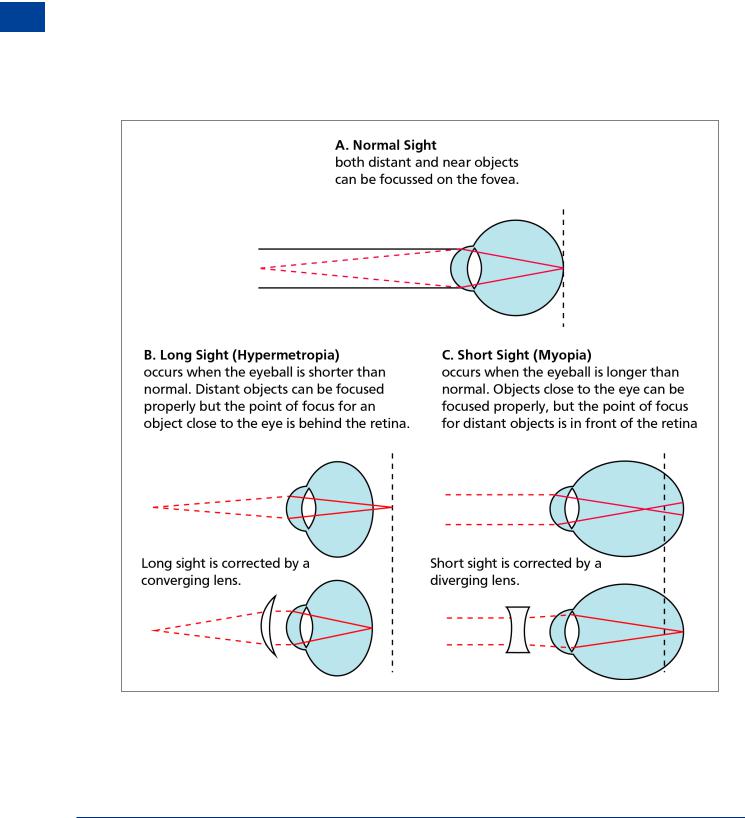
Hypermetropia (long-sightedness) and myopia (short-sightedness) are caused by the distorted shape of the eyeball.
Hypermetropia
In long sightedness, hypermetropia, a shorter than normal eyeball along the visual axis results in the image being formed behind the retina and, unless the combined refractive index of the cornea and the lens can combine to focus the image in the correct plane, a blurring of the vision will result when looking at close objects. A convex lens will overcome this refractive error by bending the light inwards before it meets the cornea.
Myopia
In short-sightedness, Myopia, the problem is that the eyeball is longer than normal and the image forms in front of the retina. If accommodation cannot overcome this, then distant objects are out of focus whilst close up vision may be satisfactory. A concave lens will correct the situation by bending the light outwards before it hits the cornea. Pilots with either hypermetropia or myopia may usually retain their licences provided that their corrected vision allows them to read normal small print in good lighting at a distance of 30 cm and have at least 6/9 vision in each eye, but with 6/6 vision with both eyes. This is equivalent to reading a car number plate at about 40 metres, as compared to the driving test requirement of 23 metres. Bifocal spectacles may be used when flying.
The Eye and Vision 5
81
5 |
|
The Eye and Vision |
|
||
|
|
|
Vision and Eye The 5
Presbyopia
The ability of the lens to change its shape and therefore focal length (accommodation) depends on its elasticity and normally this is gradually lost with age. After the age of 40 to 50 the lens is usually unable to accommodate fully and a form of long-sightedness known as presbyopia occurs. The effects start with difficulty in reading small print in poor light. The condition normally requires a minor correction with a weak convex lens. Half lenses or lookover spectacles will suffice.
Astigmatism
The surface of a healthy cornea is spheroidal in shape. Astigmatism is usually caused by a misshapen or oblong cornea and objects will appear irregularly shaped. Although astigmatism can be cured by the use of cylindrical (toric) lenses, modern surgical techniques can reshape the cornea with a scalpel or, more easily, with laser techniques.
Figure 5.4 Correction of myopia with a concave lens & correction of hypermetropia with a convex lens
It is a requirement that aircrew who have to wear correcting spectacles, in order to exercise the privileges of their licence, are to carry a spare (easily accessible) pair during flight.
82

The Eye and Vision |
|
5 |
|
||
|
|
|
Cataracts
Cataracts are normally associated with the ageing process though some diseases can cause cataracts at any age. With time, the lens can become cloudy causing a marked loss of vision. For severe cases, traditional surgery is carried out in which a section of the lens is removed and replaced with an artificial substitute. Surgery utilizes local anaesthesia on an outpatient basis and, following successful treatment, pilots will normally be allowed to return to flying.
Glaucoma
Glaucoma is a disease of the eye which causes a pressure rise of the liquid in the eye (aqueous humour). The fluid protects the lens and nourishes the cornea. It passes through a small shutter which can either be flawed or can become jammed causing a rise in pressure of the eye. The normal pressure range is 10 - 20 mm Hg. Glaucoma damages the optic nerve and may cause severe pain and if left untreated, blindness. Part of the JAA medical examination is a test for glaucoma. The symptoms can be treated either be by eye drops (timitol) or by an operation in which a hole is made in the shutter. Glaucoma can be inherited or may result from the ageing process.
The main symptoms of Glaucoma are:
•Acute pain in the eye - in extreme cases.
•Blurred vision.
•Sensitivity to high light levels.
•Visual field deterioration.
•Red discolouration of the eye.
Use of Contact Lenses
Contact lenses provide better peripheral vision and are not subject to misting. Therefore many pilots are attracted to the idea of wearing them instead of spectacles. But there are a number of problems:
•As the cornea does not have its own blood supply, it obtains its oxygen from the ambient air. Mild hypoxia and dehydration, caused by low humidity on the flight deck, increase the potential for corneal damage when using contact lenses.
•Cabin decompression may result in bubble formation under the contact lens.
•The lens may be dislodged by careless rubbing of the eyes (for example when the humidity is low), an accidental knock or increased g-forces.
Whereas the use of contact lenses by aircrew is permitted, under authorised medical supervision, bifocal contact lenses are prohibited.
Note: Should a pilot be cleared by the authorities to use contact lenses for flying it will be on the proviso that a pair of ordinary spectacles is carried at all times while practising the privileges of his/her licence.
The Eye and Vision 5
83

5 |
|
The Eye and Vision |
|
||
|
|
|
Vision and Eye The 5
Colour Vision
Good colour vision is essential for flight crew because of use of colour associated with the following:
•Navigation lights of aircraft.
•Runways and airfields.
•Ground obstructions.
•Cockpit displays and instruments.
•Maps and charts.
•Emergency flares.
•Light signals.
Colour Blindness
Total colour blindness is a bar to the issue of a flying licence. It is caused by a defect in the structure of the colour sensitive cones in the retina - normally when a single group is missing. Whereas total colour blindness is extremely rare, many people suffer from this defect to a degree (colour defective). The most common form is red/green blindness. These colours are seen in shades of yellow, brown or grey. It does not affect acuity and many people go through their lives with no knowledge that they suffer from this imperfection.
Colour blindness is rare in women, however they do act as carriers of this incurable and congenital flaw.
Vision and Speed
In high speed flight (greater than approximately 450 knots), particularly at very low altitudes of below 500 ft, the principle problem is extension of the total reaction time (visual input, brain reaction, perception, recognition, evaluation, decision, action and response). In the ideal circumstances this takes about 5 - 7 seconds. Although many factors - including workload and fatigue - may prolong this period, it is the initial triggering of visual input, brain reaction, perception and recognition (or the “visual perception cascade)” that is especially important. In perfect conditions the visual perception cascade takes approximately 1 second however the following factors may extend this time period:
•Poor atmospheric conditions.
•Darkness.
•Size and contrast of object.
•Angular approach. An aircraft, for example, approaching head-on will stimulate the retina less than one tracking tangentially across the visual field.
Monocular and Binocular Vision
Binocular vision is not essential for flying and there are many one-eyed (monocular) pilots, currently flying with a class II medical certificate. However should a pilot lose an eye it normally takes some time for the brain to learn to compensate for the loss of binocular vision and for the individual to regain his/her medical certificate. However, a person with vision in only one eye cannot be accepted under EASA as fit to fly.
84