

The Eye and Vision |
|
5 |
|
||
|
|
|
It is worth noting that the human eye has approximately 1.2 million neurones leading from the retina to the visual cortex of the brain, while there are only about 50 000 from the inner ears. The eye is about 24 times more sensitive than the ear.
The Fovea and Visual Acuity
Fovea
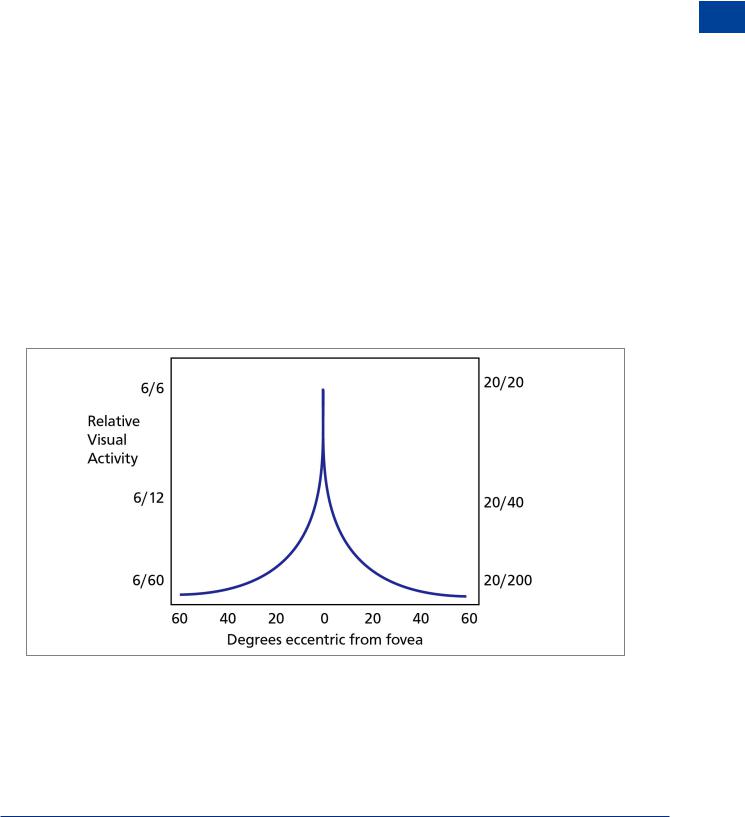
The central part of the retina, the fovea, is composed only of cone cells. Anything that needs to be examined in detail is automatically brought to focus on the fovea. The rest of the retina fulfils the function of attracting our attention to movement and change. Only at the fovea is vision 20/20 or 6/6. This is termed as central vision.
The visual field comprises both the central and peripheral vision.
Note: Alphanumeric information is limited to the foveal area of the retina.
Visual Acuity
This is a measure of central vision and the figures above are a means of measuring visual acuity. It is the ability to discriminate at varying distances. An individual with an acuity of 20/20 vision should be able to see at 20 feet that which the so-called normal person is capable of seeing at this range. It is sometimes expressed in metres (6/6). The figures 20/40 (or 6/12) mean that the observer can read at 20 feet what a normal person can read at 40 feet (6 /12 metres).
Any resolving power at the fovea drops rapidly as the angular distance from the fovea increases. At as little as 5° from the fovea the acuity drops to 20/40 that is half as good as at the fovea. At approximately 25° acuity decreases to a tenth (20/200). See Figure 5.2 below.
Figure 5.2 The change in acuity across the retina
The Eye and Vision 5
77

5 |
|
The Eye and Vision |
|
||
|
|
|
Vision and Eye The 5
Limitations of Acuity
In effect acuity will be limited by many factors among which are:
•Angular distance from the fovea.
•Physical imperfections within the visual system.
•Age.
•Hypoxia.
•Smoking.
•Alcohol.
•Visibility (dust,mist etc.).
•Amount of light available
•Size and contours of an object.
•Distance of the object from the viewer.
•Contrast of an object with its surroundings
•Relative motion of a moving object.
•Drugs or medication.
Light and Dark Adaptation
Light Adaptation
When experiencing sudden high levels of illumination the eye quickly adjusts (approximately 10 seconds). However, if a person has been in bright light for a long time, large proportions of the photochemicals in both the cones and rods are reduced thereby reducing the sensitivity of the eye to light. Thus going quickly from outside on a sunny day into a darkened room has the effect of vision being severely reduced until dark adaptation takes place.
Dark Adaptation
On the other hand, if the person remains in darkness for a long time the reverse takes place and both the cones and rods gradually become supersensitive to light so that even the minutest amount of light causes excitement of the receptors.
Night Vision
You may have noticed that in dim light it is easier to focus on an object if you look slightly away from it. As the fovea contains no rods, which would be required for vision in very low brightness levels, the centre part of the eye becomes blind to dim light. It is then necessary to look away from the visual target so that the peripherally located rods can perform their sensing task. This is most noticeable when night flying.
You can demonstrate this to yourself by looking at dim stars on a clear night. Some of them will be invisible with direct viewing but will be discernible if you look 10° to 15° off to one side.
It takes time for our eyes to adapt to darkness. This adaptation does take time - about 7 minutes for the cones and 30 minutes for the rods. However even a brief exposure to bright light will require a further period of adaptation to recover effective night vision.
It is good airmanship to avoid bright lights about 30 minutes prior to a night flight. It is also advisable to turn up cockpit lights when approaching a weather pattern which might produce the possibility of lightning. It is possible that fatigue may also necessitate the increase of instrument lighting.
78
The Eye and Vision |
|
5 |
|
||
|
|
|
From sea level to 3000 m is known as the “indifferent zone” because ordinary daytime vision is unaffected up to this altitude. There is, however, a slight impairment of night vision. Without supplemental oxygen, the average percent decrease in night vision capability is:
5% at 1100 metres
18% at 2800 metres
35%at 4000 metres
50%at 5000 metres
The most common factors affecting night vision are:
•Age (see presbyopia later in this chapter).
•Mild hypoxia.
•Cabin altitudes above 5000 ft (but not detrimental below approximately 12 000 ft).
•Smoking (a consumption of 20 cigarettes a day results in a night vision degradation of approximately 20%).
•Alcohol.
•Minor illnesses.
•Deficiency of vitamin ‘A’.
The Blind Spot
The point on the retina where the optic nerve enters the eyeball has no covering of lightdetecting cells. Any image falling on this point will not be detected. This has great significance when considering the detection of objects which are on a constant bearing from the observer. If the eye remains looking straight ahead it is possible for a closing aircraft to remain in the blind spot until a very short time before impact. Safe visual scanning demands frequent eye movement with minimal time spent looking in any direction.
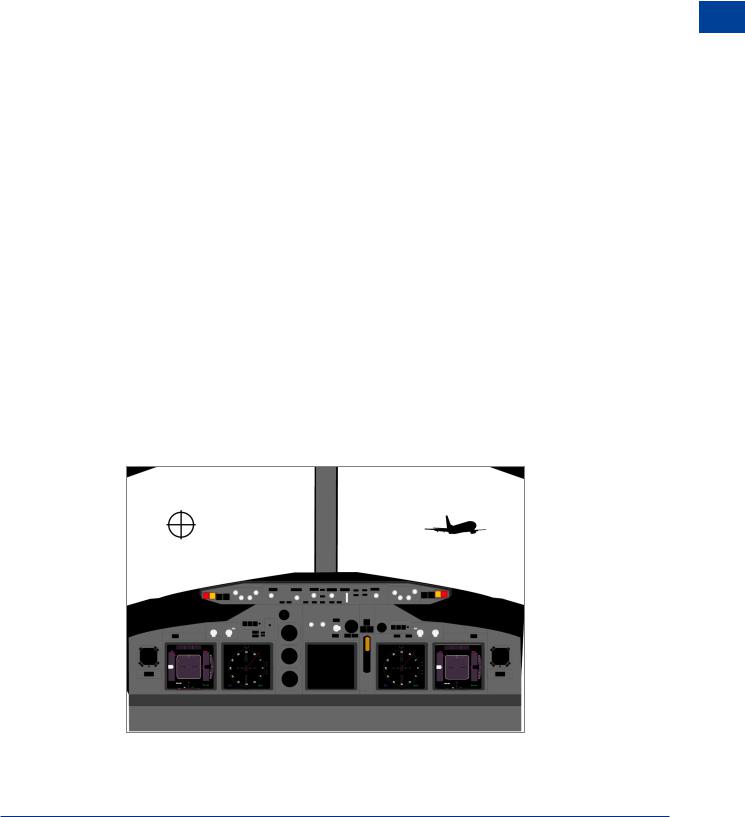
Use Figure 5.3 to demonstrate to yourself the existence of the blind spot. Hold the drawing at arm’s length, close the left eye and keep the right eye open. Now move the picture towards the face keeping the right eye focused on the cross. The aircraft will disappear, then reappear as it gets close.
The Eye and Vision 5
Figure 5.3 The blind spot
79

5 |
|
The Eye and Vision |
|
||
|
|
|
Vision and Eye The 5
If both eyes of the observer are open and unobscured the blind spot is not a problem as each eye is able to see the detail in the other eye’s blind spot. However there is a very real possibility that an approaching aircraft on a constant bearing will not be seen since it remains in the blind spot of one eye and an object/person within the cockpit is obscuring the aircraft from the pilot’s other eye.
Stereopsis (Stereoscopic Vision)
Some of the optic nerve fibres cross over in the brain. Because one eye is a little more than 2 inches (5 cm) to one side of the other eye, the images on the two retina are different from one another. This enables the brain to compare the slight differences seen by each eye. The brain interprets this as depth/distance perception. Thus a person with two eyes has a far greater ability to judge relative distances when objects are nearby than a person who only has one eye. However stereopsis is virtually useless for depth perception at distances beyond 200 ft/60 m.
Empty Visual Field Myopia
In the absence of anything to focus on (empty field) the natural focus point of the eye is not at infinity, as was long assumed, but on average at a distance of between just under 1 metre and 1.5 metres, although there are wide variations between individuals.
This is very significant in searching for distant targets when visual cues are weak, as the eye will not be adjusted to detect them. The condition is aggravated when there are other objects close to the empty field range, rain spots on the windscreen for example, as the eye will naturally be drawn to them.
This phenomena can occur in cloudless skies at high altitudes, in total darkness, under a uniformly overcast sky or when resting the eyes.
Aircrew should minimize the risks associated with empty visual field by periodically and deliberately focusing on objects thus exercising the eyes.
High Light Levels
It is possible for too much light to fall on the eye. Pilots are exposed to much higher light levels than most people. Very high light levels occur at altitude where light may be reflected from cloud and more importantly, where there is less scattering of the light rays by atmospheric pollution.
Normal sunlight contains all the colours of the spectrum but at high altitudes pilots are exposed to light that contains more of the high energy blue and ultra violet wavelengths than is experienced at sea level. The higher energy blue light can cause cumulative damage to the retina over a long period. Ultra violet wavelengths can also cause damage, mainly to the lens of the eye, but most are filtered out by the cockpit windows.
Sunglasses
Wearing appropriate sunglasses can provide complete protection against the above problems. When purchasing sunglasses always consult a knowledgeable supplier. Sunglasses should have the following characteristics:
80