

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdf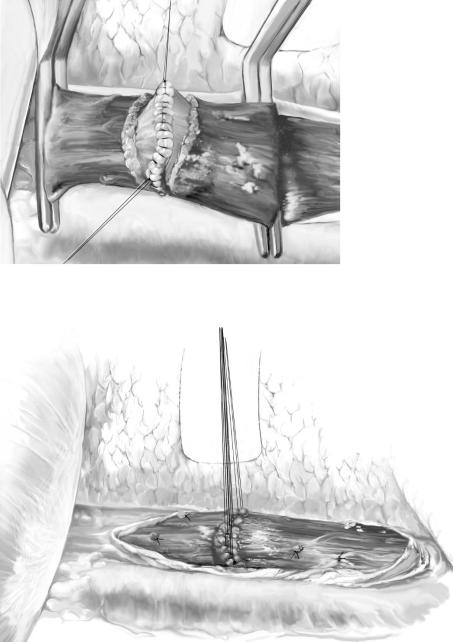
Gastroesophageal Devascularization: Sugiura Type Procedures |
709 |
|
|
|
|
STEP 4 (continued) |
Esophageal transection 2 |
|
|
|
|
A-3
A-4

710 |
SECTION 5 |
Portal Hypertension |
|
|
|
STEP 5 |
Diaphragmatic incision |
|
|
|
|
After completion of esophageal transection, the diaphragm is incised, with care taken not to damage the phrenic nerve and pericardiacophrenic vessels.
The spleen is then exposed and the left triangular ligament of the liver is divided and ligated.
STEP 6 |
Splenectomy 1 |
|
The splenophrenic, splenorenal, and splenocolic ligaments are divided and the spleen is |
|
|
|
completely mobilized. The gastrosplenic ligament is divided and short gastric vessels are |
|
transected. The dissection is directed toward the hilus of the spleen. |

Gastroesophageal Devascularization: Sugiura Type Procedures |
711 |
|
|
|
|
STEP 7 |
Splenectomy 2 |
|
|
|
|
After the ligamentous attachments and short gastric vessels have been divided, all that remains are the main splenic artery and vein. They are doubly ligated and divided. Care should be taken not to damage pancreatic tissue, because even a small tear may cause pancreatic leakage.

712 |
SECTION 5 |
Portal Hypertension |
|
|
|
STEP 8 |
Paraesophagogastric devascularization |
|
|
|
|
The abdominal esophagus and the cardia are devascularized from the greater curvature and the posterior of the stomach to the esophagus. The posterior gastric vagus nerve is divided by this procedure because the nerve runs very close to the stomach. Devascularization of the lesser curvature of the stomach and the abdominal esophagus follows, and the cardioesophageal branches of the left gastric vessels are ligated and divided. The length of devascularization is about 7cm at the lesser curvature of the cardia.
The esophagus and the cardia are completely mobilized and freed from the adjacent structures. A common pyloroplasty is performed because the gastric vagus nerves are divided.

714 |
SECTION 5 |
Portal Hypertension |
|
|
|
|
Tricks of the Senior Surgeon |
|
■During the devascularization procedure, every shunting vein between the dilated paraesophageal collateral veins and esophageal wall should be ligated. Care should be taken not to damage the truncus vagalis and collateral veins, which are theoretically very important in preventing variceal recurrence. Although this is not always practically achievable, collateral channels in the mediastinum are believed to be preserved during the operation.
■A lasting extirpation of esophageal varices after nonshunting operation may depend on the portosystemic collateral changes that take place after the operation. Preserved paraesophageal and mediastinal collateral channels after the Sugiura operation are expected to function as a spontaneous shunt.
Acknowledgements
The authors thank Dr. Shunji Futagawa (Professor Emeritus of the 2nd Department of Surgery, Juntendo University) for supplying original drawings for this chapter.

Gastroesophageal Devascularization: Sugiura Type Procedures |
715 |
|
|
Procedure 2:
Complete Porto-azygos Disconnection with Spleen Preservation
Hector Orozco, Miguel A. Mercado
Introduction
Complete porto-azygos disconnection requires both abdominal and thoracic procedures. The following series of illustrations offers the alternative of a spleen preserving abdominal devascularization.
Indications, testing, and preoperative management are the same as for the full thoracoabdominal procedure described in the previous chapter.
Overview of the Abdominal Procedure
The abdominal part of the procedure includes the following components:
■Dividing the gastrohepatic ligament – gastrocolic ligament – left gastric artery and vein.
■Ligature the right gastric artery and vein over the lesser curvature.
■Ligature the right gastroepiploic vein.
■Devascularization of the great curvature with preservation of the spleen.
■Devascularization of the abdominal esophagus and transection of the main vagus nerves.
■Pyloroplasty.

716 |
SECTION 5 |
Portal Hypertension |
|
|
|
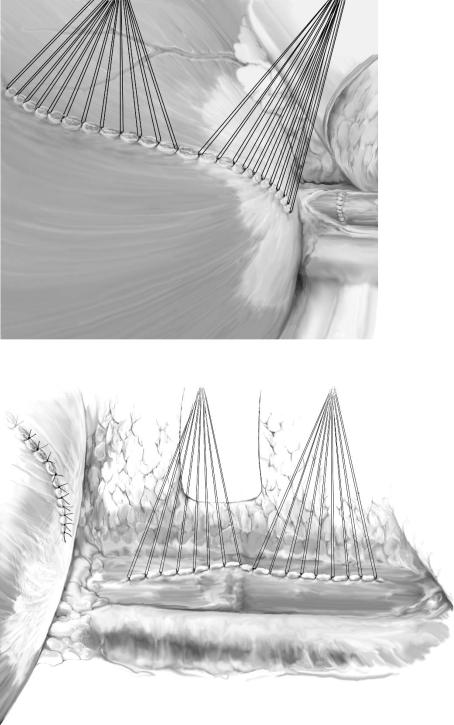
STEP 1 |
Devascularization of the greater curvature |
|
|
|
|
From the left side, showing the complete devascularization of the greater curvature of the stomach, with all vessels divided from the pylorus up to the esophagus. The short gastric vessels are divided, leaving the spleen in situ.

Gastroesophageal Devascularization: Sugiura Type Procedures |
717 |
|
|
|
|
STEP 2 |
Completion of the devascularization of the lesser curvature |
|
|
|
|
Complete devascularization of the stomach from the right side of the patient. This shows the upper two-thirds of the lesser curvature devascularized up to the esophagus.