

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdf426 |
SECTION 3 |
Liver |
|
|
|
|
Procedures |
|
|
Laparoscopic Unroofing of a Simple Cyst |
|
|
|
|
STEP 1 |
Access and exploration |
|
|
Usually three ports are used: camera, grasper for the cyst wall, and cutting instrument |
|
|
||
|
(cautery, harmonic scalpel, or scissors). Placement varies according to the anatomic |
|
|
location of the cyst . One of the working ports should be 10mm for clip application. |
|

Unroofing and Resection for Benign Non-Parasitic Liver Cysts |
427 |
|
|
|
|
STEP 2 |
Unroofing |
|
|
|
|
The dome of the cyst is elevated with a grasper. Incising the cyst and draining its contents makes the cyst wall flaccid and easier to handle (A, B). The wall of the cyst is resected with electrocautery. Excision should be as close as possible to the interface between the cyst and the remnant liver. It is very important to resect the maximal amount of the wall of the cyst to enhance retraction of the remnant edge of the cyst, thus preventing reapproximation of the rim by contraction with subsequent recurrence. Cytology of the aspirate is performed if indicated and if the cyst is complex with mural nodules. Effaced ducts or vessels at the cyst-liver interface should be stapled or clipped. After removal, the cyst wall is assessed histologically.
A
B
428 |
SECTION 3 |
Liver |
|
|
|
STEP 3 |
Inspection of the cyst |
|
|
After unroofing, the residual cyst wall is inspected carefully. Irregularities within the |
|
|
|
|
|
concavity of the cyst are biopsied. When less than 50% of the cyst has been removed, |
|
|
ablation of the remnant cyst lining directly by cautery, argon beam coagulation, or |
|
|
topical sclerosant may reduce the incidence of recurrence. Omentum can be placed |
|
|
within the cyst remnant to prevent recurrence in this circumstance. |
|
|
Open Unroofing of a Simple Cyst |
|
|
|
|
STEP 1 |
Access and approach |
|
|
Cysts located superiorly in segments 7 and 8 are usually unroofed in an open fashion. |
|
|
||
|
A right subcostal incision is indicated in these cases; the triangular and a portion of |
|
the coronary ligaments are divided to rotate the liver (see chapter “Right Hemihepatectomy”). Using the nondominant hand, the surgeon pulls the liver toward the midline to complete the exposure of the cyst. The same principles dictated for the laparoscopic
approach are followed and the cyst is unroofed. Alternatively, the cyst can be enucleated en toto.
Unroofing and Resection for Benign Non-Parasitic Liver Cysts |
429 |
|
|
|
|
STEP 2 |
Inspection of the cyst |
|
|
|
|
There is no cyst wall left above the level of the hepatic parenchyma. Occasionally, blood vessels or bile ducts can be seen on the cavity. No drains are necessary after cyst excision.
430 |
SECTION 3 |
Liver |
|
|
|
|
Enucleation of Biliary Cystadenoma |
|
|
|
|
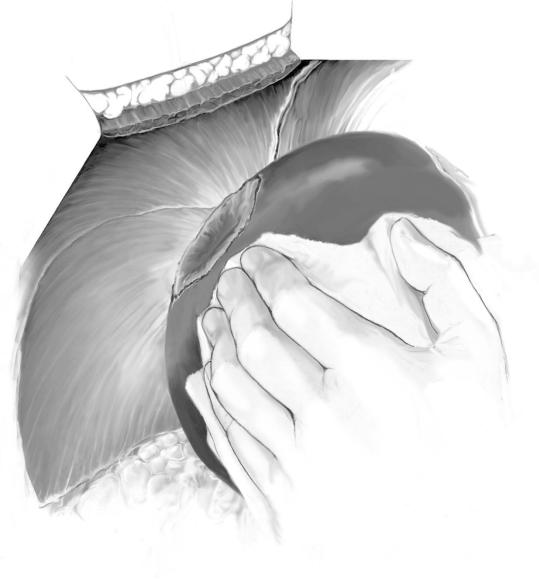
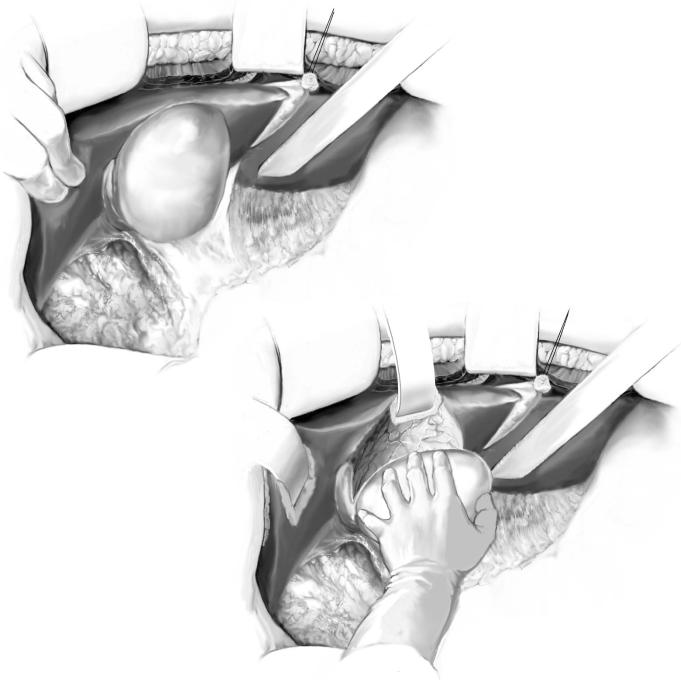
STEP 1 |
Enucleation of the cyst (A) |
|
|
After mobilization of the liver, countertraction is maintained by the nondominant hand |
|
|
||
|
of the surgeon (B). The interface between the cyst and the hepatic parenchyma is identi- |
|
|
fied and developed; the wall of the cyst is usually thick and rarely ruptures. With deeper |
|
dissection, compressed vessels and bile ducts become evident and should be preserved. The dissection is completed circumferentially and the cystadenoma is enucleated and sent for histologic analysis to exclude occult cystadenocarcinoma.
A
B
Unroofing and Resection for Benign Non-Parasitic Liver Cysts |
431 |
|
|
|
|
STEP 2 |
Repair of vasculobiliary injuries |
|
|
|
|
When inadvertent injury of the bile ducts occurs, a fine (4-0 or 5-0 absorbable) interrupted suture is used for repair. Abdominal drainage is optional. Importantly, complete excision of the cystadenoma eliminates risk of recurrence.
432 |
SECTION 3 |
Liver |
|
|
|
|
Laparoscopic Resection of Cysts |
|
|
|
|
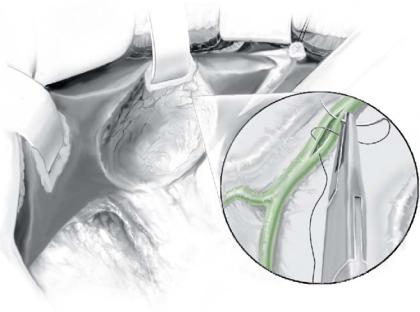
STEP 1 |
Access, approach and parenchymal transection |
|
|
Laparoscopic resection is used to treat peripheral cysts, especially those in the left lateral |
|
|
||
|
sector (Sg2 and 3) or in the anterior segments (Sg4B, 5, and 6). The CT scan and the |
|
|
picture illustrate a simple cyst in Sg3. The approach described previously is undertaken. |
|
|
Three ports are usually used, and their placement depends on the site of the cyst. |
|
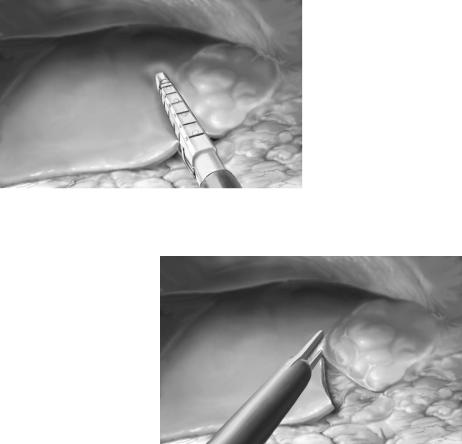
The most common instruments used for this purpose are the Harmonic Scalpel, Tissuelink, CUSA, and surgical staplers. The surgeon needs to determine the most direct route for positioning the instrument to achieve a complete cyst resection with sparing of healthy parenchyma. Since these lesions are usually peripheral and the parenchyma is thin, at times the stapler has the capability of securing tightly both the superior and the inferior edges of the line of transection and results in a nearly bloodless margin. Identification of individual vasculobiliary structures in this situation is not necessary (A). When the tissue is too thick for stapling devices, the initial transection can be done with ultrasonic shears (B) or any other method of vascular sealing, and the pedicle taken with the staplers. The Pringle maneuver is usually not required for this type of transection.
A
B

Unroofing and Resection for Benign Non-Parasitic Liver Cysts |
433 |
|
|
|
|
STEP 2 |
Resection of the specimen |
|
|
|
|
After the transection of the hepatic parenchyma is completed, hemostasis must be confirmed by direct inspection. Sometimes it is useful to “feel” or abrade the transection line to exclude a vessel that has stopped bleeding temporarily but may act as a site of remnant bleeding once the pneumoperitoneum is evacuated and normal intra-abdom- inal pressure returns. If identified, hemostasis is secured by electrocautery, surgical clips, and hemostatic agents or devices when still available.
Postoperative Tests
■Routine postoperative surveillance for most patients
■Intermediate care or intensive care units for complicated cases of polycystic disease of the liver
Postoperative Complications
See chapter “Right Hepatectomy.”
434 |
SECTION 3 |
Liver |
|
|
|
|
Tricks of the Senior Surgeon |
|
■Although unroofing is simple, enucleation carries risk of hemorrhage. Make certain the hepatic duct and ligament is accessible for a Pringle maneuver if needed.
■Look for small biliary radicals after enucleation; drainage is not a good alternative to repair or suture ligation.
■During laparoscopic resection of hepatic cysts, be aware that major pedicles may not be amenable to sealing devices. Surgical staplers are still the best mechanism to secure structures.
■Like in any laparoscopic procedure with potential bleeding, do not hesitate to open up the patient in the presence of significant bleeding. Safety is still better than pride!
Pericystectomy for Hydatid Liver Cyst
Lucas McCormack
Patients with hydatid cysts in the liver used to present a therapeutic challenge. Although surgical techniques have improved, considerable controversy still exists regarding the most effective operative technique. The main principle of the surgery is to eradicate the parasite and prevent intraoperative spillage of cyst contents avoiding peritoneal spread. Pericystectomy provides a radical treatment removing the whole cyst “en bloc” including the adventitia without resection of healthy liver tissue.
Preoperative Treatment
Albendazol orally 10–14mg/kg/day in two doses administered 2–4weeks before and after surgery.
Indications and Contraindications
Indication |
■ |
Peripheral hydatid cyst of the liver |
|
|
Intrahepatic major vascular invasion |
Contraindications |
■ |
|
|
■ |
Invasion of right or left hepatic duct |
|
■ |
Deep cyst within the liver parenchyma (>2–3cm from liver surface) |
|
■ |
General contraindication of liver resections |