

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdfSegmentectomies, Sectionectomies and Wedge Resections |
383 |
|
|
|
|
STEP 2 |
Hepatic parenchymal transection along the right intersectional plane |
|
|
|
|
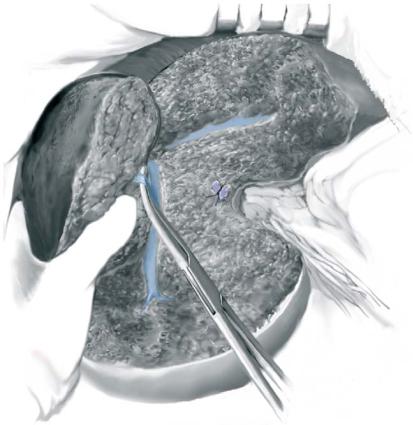
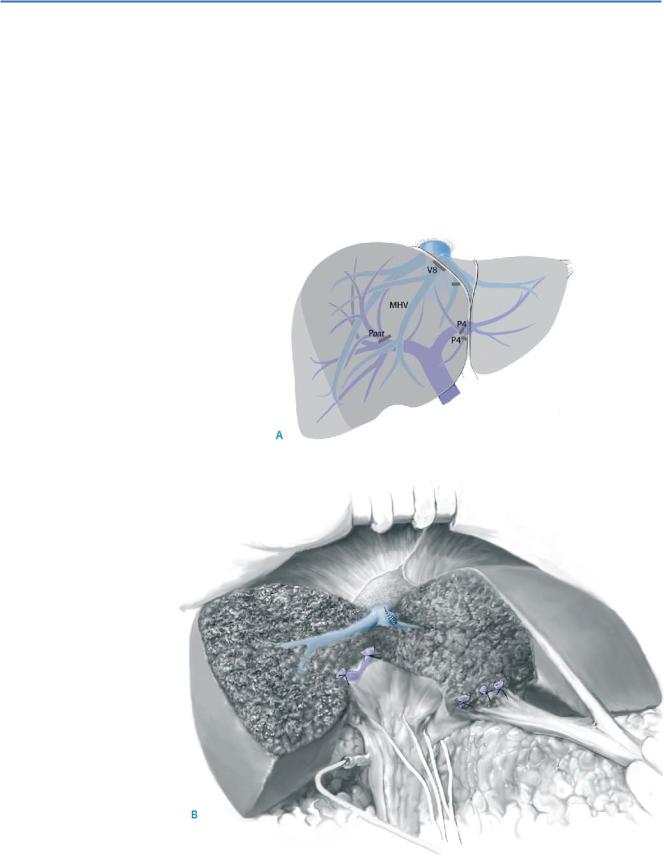
Under a right hemihepatic vascular occlusion, hepatic parenchymal transection along the right intersectional plane is started (A). The anterior section is lifted with the operator’s left hand and the portal pedicle for the anterior section (Pant) is ligated and divided (B)
384 |
SECTION 3 |
Liver |
|
|
|
STEP 3 |
Transsection of the RHV branch |
|
|
|
|
The RHV is exposed and a thick venous branch draining the anterior section is divided.
After removal of the anterior section, landmarks including MHV, RHV, and the stump of
Pant are exposed.
Segmentectomies, Sectionectomies and Wedge Resections |
385 |
|
|
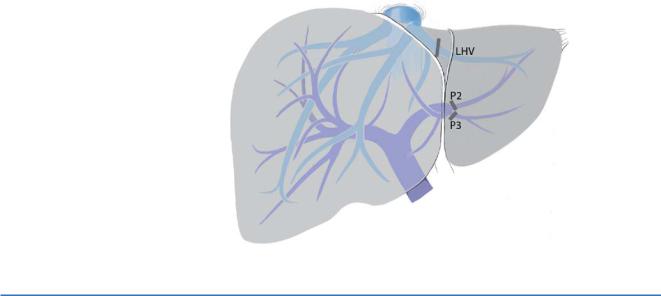
Left Lateral Sectionectomy
(Anatomical Resection of Segments 2 and 3)
The Figure depicts the important anatomical structures for this procedure.
STEP 1 |
Hepatic parenchymal transection along the left edge of the falciform ligament |
|
(the left intersectional plane) |
|
|
|
By pulling up the left liver via the round ligament, hepatic parenchymal transection is |
|
done along the left edge of the falciform ligament. The left wall of the portal pedicle for |
|
the umbilical portion of the portal vein is exposed, and all of the tributaries running |
|
into the lateral section are ligated and divided. When liver parenchyma of segment 3 and |
|
4 is connected in the visceral side of the umbilical portion, the connecting part is |
|
divided during parenchymal transection. |
|
|
STEP 2 |
Division of portal pedicles for segment 2 and 3 |
|
Along the left wall of the umbilical portion of the portal vein, there are a few thick portal |
|
|
|
pedicles for segment 3 (P3). All of them are ligated and divided. Portal pedicles for |
|
segment 2 (P2) are located in the cranial edge of the umbilical portion of the portal vein. |
|
They are usually thicker than P3s and only 2 or 3cm caudal to the root of the left hepatic |
|
vein (LHV). They are ligated and divided. |
386 |
SECTION 3 |
Liver |
|
|
|
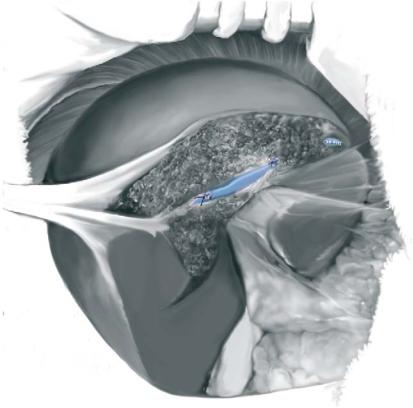
STEP 3 |
Division of the left hepatic vein (LHV) |
|
|
At the end of the hepatic parenchymal transection, the root of the left hepatic vein |
|
|
|
|
|
(LHV) is exposed and divided. The stump of LHV is ligated or is closed by running |
|
|
suture. The Figure shows the situation at the end of the procedure. |
|
Segmentectomies, Sectionectomies and Wedge Resections |
387 |
|
|
Left Medial Sectionectomy
(Anatomical Resection of Segment 4)
Figure A depicts the important anatomical structures for this procedure.
Hepatic parenchymal transection is done along the midplane of the liver and the right side of the umbilical portion of the portal vein (the left intersectional plane). After removal of the left lateral section, landmarks including MHV and stumps of P4s are exposed (B).
388 SECTION 3 Liver
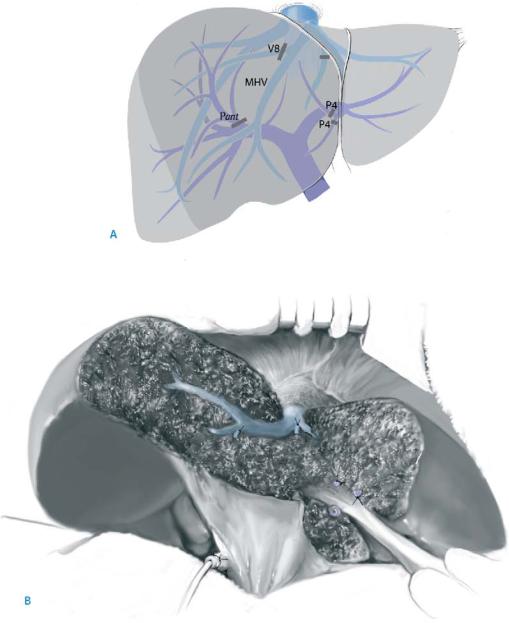
Central Hepatectomy
(Anatomical Resection of Segments 4, 5, and 8)
Figure A depicts the important anatomical structures for this resection.
Hepatic parenchymal transection is done along the right and left intersectional plane (i.e., the umbilical portion of the portal vein). The MHV is divided at its root. After removal of the left lateral section, landmarks including RHV and stumps of Pant and P4s are exposed (B).
For preparation of the right and anterior portal vein/right hepatic artery, and identification of the right intersectional plane, see also steps for anterior sectionectomy above.
Segmentectomies, Sectionectomies and Wedge Resections |
389 |
|
|
Wedge Resection (Limited Resection)
The aim of this procedure is a non-anatomical complete removal of the tumor with sufficient margin. A wide surgical margin (e.g., wider than 10mm) is not necessary, but care should be taken not to expose the tumor on the cut surface.
Tricks of the Senior Surgeon
■Complete exposure of major hepatic veins, the landmarks for the intersegmental planes, is the key for successful segmentectomy and sectionectomy.
■Before starting hepatic parenchymal transection, branching patterns of the major hepatic veins in each patient should be examined thoroughly with intraoperative ultrasound.
■Major hepatic veins are first exposed at their root and distal edge in the cut surface. Then the middle part of the venous trunks is exposed from both ends.
■A tip of the Metzenbaum scissors is useful for dissecting hepatic veins, and all venous branches larger than 1mm should be ligated.
■Very tiny branches can be pulled out from the parenchyma (not from the venous wall) with vascular pickups.
■CVP should be kept low (<3 mm Hg) to reduce blood loss during the parenchymal transection.
Laparoscopic Liver Resection
Daniel Cherqui, Elie Chouillard
Introduction
Unroofing of symptomatic simple liver cysts was the first laparoscopic liver procedure to be performed followed by resection of superficial, small-sized benign tumors. The first laparoscopic anatomical liver resection, a left lateral sectionectomy, was reported in 1996. More recently, larger hepatectomies and liver resections for malignant tumors have been described. Today, about 15–20% of liver resections might be considered for a laparoscopic approach.
Indications and Contraindications
Indications |
The indications for laparoscopic liver resections are the same as for open liver |
|
|
resections. Based on tumor size and location of the lesion, the following situations |
|
|
are most suitable for a laparoscopic approach: |
|
|
■ |
Non-pedunculated lesions less than 5cm in diameter |
|
■ |
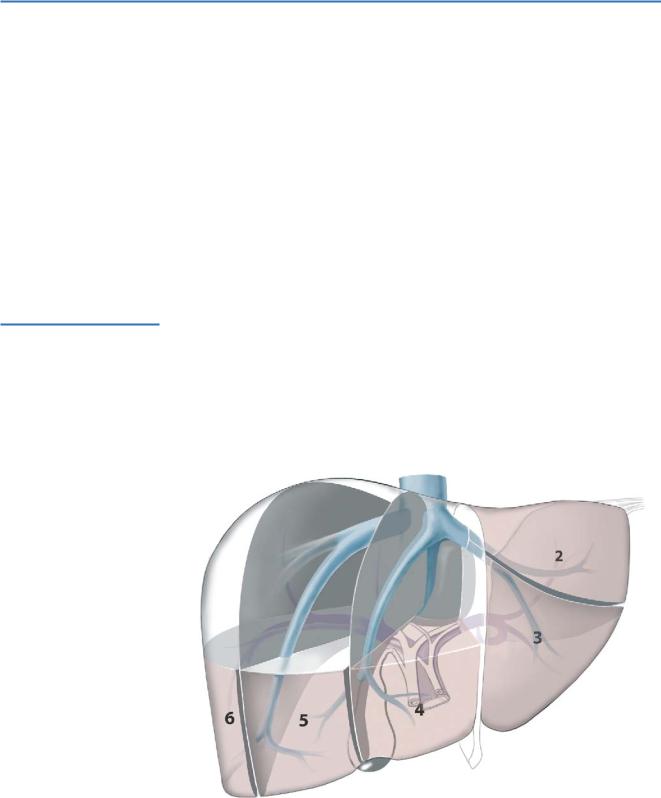
Lesions located in the anterior segments of the liver (segments 2–6; see Figure) |
|
■ |
Pedunculated lesions of any size |
392 |
SECTION 3 |
Liver |
|
|
|
|
|
|
The contraindications are mainly anatomical and related to the size and location |
|
|
Contraindications |
|
||
|
of the lesions. |
|
|
|
■ |
Large non-pedunculated tumors (>5cm in diameter) |
|
|
■ |
Lesions of the hepatic dome (i.e., segments 7 and 8) |
|
|
■ |
Lesions located in the vicinity of major hepatic veins, the inferior vena cava and the |
|
|
|
hepatic hilum |
|
|
■ |
Severe portal hypertension (e.g. portal pressure >12 mm Hg) |
|
|
■ |
Severe coagulopathy (e.g. platelet count <30000 ml) |
|
Laparoscopic Liver Resection |
393 |
|
|
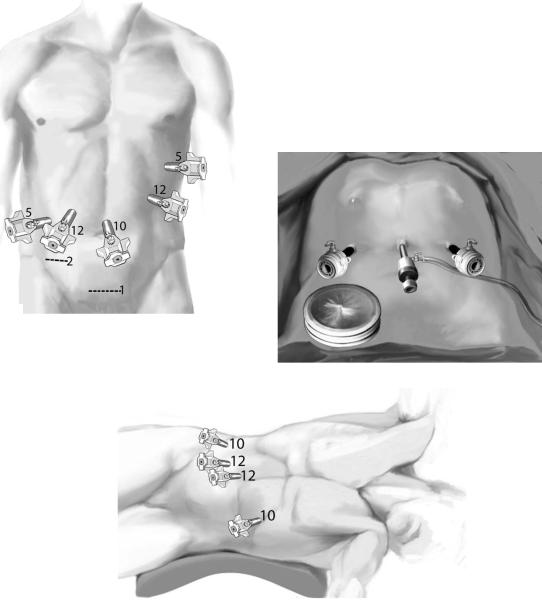
Patient Position, Port Sites and Pneumoperitoneum
■For lesions in segments 2 through 5: Supine position with lower limbs apart and 5 ports are inserted (A). A gas-tight hand port placed in the right iliac fossa can be used for hand assistance. The same incision is then used for the specimen extraction (B)
■For limited resection of segment 6: A left lateral position may be used (C)
■We recommend the use of a 30° laparoscope. A low pressure CO2 (12mmHg) pneumoperitoneum is used
A
B
C