

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdfSegmentectomies, Sectionectomies
and Wedge Resections
Norihiro Kokudo, Masatoshi Makuuchi
Introduction
Since hepatocellular carcinoma (HCC) and most metastatic diseases of the liver spread via intrahepatic portal branches, anatomical resection of a tumor bearing portal area, resection of a segment or a section, are basic procedures for treating liver tumors.
In this chapter, we feature anatomical resection of segment 8, segment 7, and right anterior sectionectomy as typical procedures, which contain most of basic techniques for anatomical liver resection. Other procedures including left lateral sectionectomy, left medial sectionectomy, central hepatectomy, and wedge resection are briefly presented.
Anatomical Resection of Segment 8
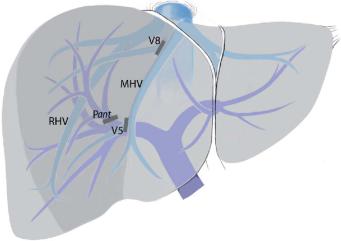
The standard three-dimensional anatomy of Sg8 is shown below.
The portal venous branches in Sg8 consist of two main branches, i.e., the dorsal branch (P8dor) and the ventral branch (P8vent), in 92% of patients. P8vent and one to three branches of Segment 5 (P5) form a trunk in 62% of patients. Between P8vent and P8dor, a thick branch of the middle hepatic vein (MHV) runs and drains Segment 8 (V8).
374 |
SECTION 3 |
Liver |
|
|
|
STEP 1 |
Access and identification of Sg8 |
|
|
|
|
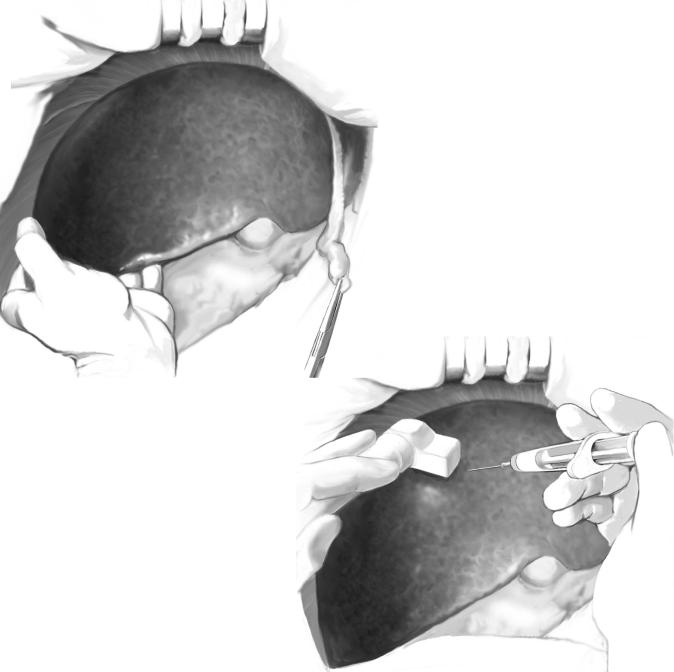
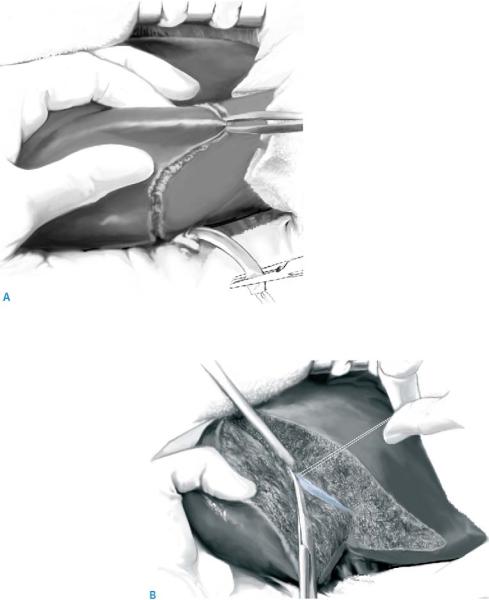
A J-shaped thoracoabdominal incision is made entering via the 9th intercostal space. Using the operator’s left hand, the right liver is easily lifted together with the diaphragm, and a wide surgical field for the right liver is obtained (A).
Under hepatic arterial occlusion with a soft jaw clamp, P8vent and P8dor are punctured with a 22G needle using intraoperative ultrasound. Approximately 5ml of indigo carmine is slowly injected into each vessel (B). The liver surface of Sg8 is stained blue and the border is marked with electrocautery. Cholecystectomy and hilar dissection are performed when hemihepatic vascular occlusion is applied during hepatic parenchymal transection. No hilar dissection is needed when Pringle’s maneuver is applied.
A
B
Segmentectomies, Sectionectomies and Wedge Resections |
375 |
|
|
|
|
STEP 2 |
Hepatic parenchymal transection along the main portal fissure |
|
|
|
|
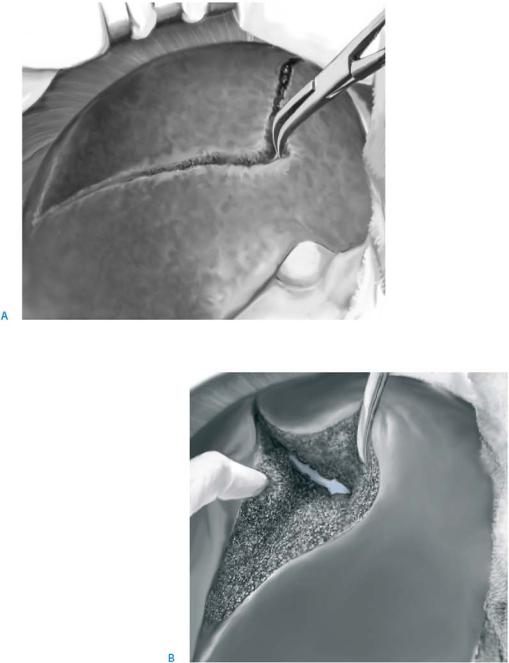
Using a curved forceps, hepatic parenchymal transection begins along the main portal fissure following the burned mark on the liver surface (A).
The trunk of the MHV is exposed and its tributaries draining Segment 8 are carefully ligated and divided (B).

376 |
SECTION 3 |
Liver |
|
|
|
STEP 3 |
Division of the portal pedicles for Segment 8 |
|
|
|
|
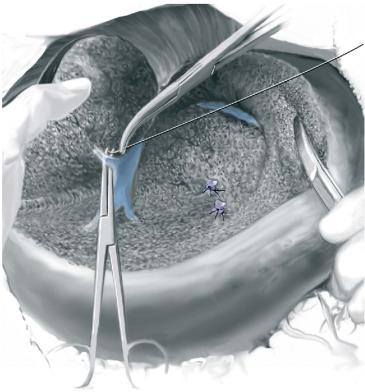
The intersegmental plane between Sg8 and Sg5 is divided and the portal pedicle for the ventral part of Sg8 (P8vent) is isolated and divided. The dorsal portal pedicle (P8dor) is then ligated and divided. Hepatic parenchymal transection along the right portal fissure is done and the right hepatic vein (RHV) is exposed.
Segmentectomies, Sectionectomies and Wedge Resections |
377 |
|
|
|
|
STEP 4 |
Exposure of RHV trunk |
|
|
|
|
The root of the RHV is exposed and a thick venous tributary draining Sg8 is divided. The specimen can now be removed and the procedure is completed with careful hemostasis and suture-ligation of bile leaks. After removal of Segment 8, landmarks including MHV, RHV, and stumps of P8vent and P8dor are exposed.
378 SECTION 3 Liver
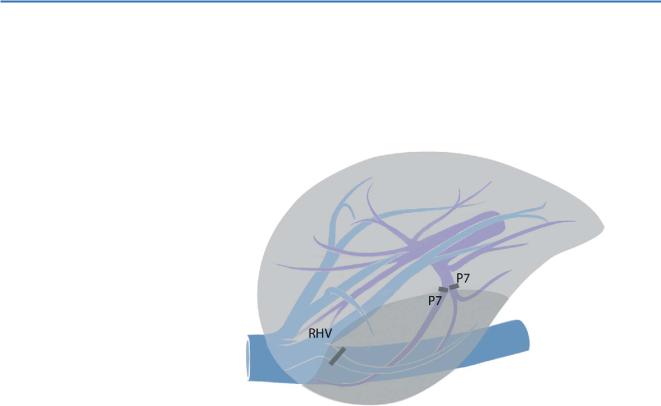
Anatomical Resection of Segment 7
Access to Sg7 is gained through a straight thoracoabdominal incision via the 8th intercostal space (left semilateral position), or through a right subcostal incision. An overview of the important anatomical structures is shown in the Figure.
Segmentectomies, Sectionectomies and Wedge Resections |
379 |
|
|
|
|
STEP 1 |
Identification of the intersegmental plane and ligation |
|
|
of small hepatic vein branches |
|
|
|
|
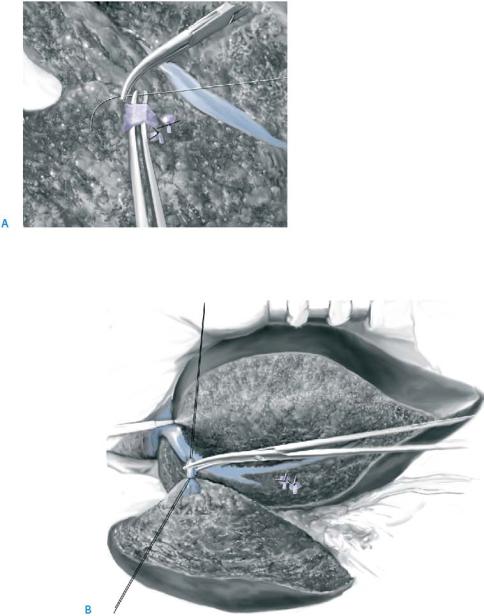
The intersegmental plane between segments 7 and 6 is identified by injecting the die into P6 (a counterstaining technique). A crushing method is applied using Pringle’s maneuver (A).
When a peripheral branch of the RHV is exposed, it is carefully traced proximally and the trunk of the RHV is exposed. Tiny branches of the RHV are carefully ligated with 4-0 silk (B).
380 |
SECTION 3 |
Liver |
|
|
|
STEP 2 |
Division of the portal pedicles for Segment 7 and exposure of the RHV |
|
|
|
|
The two major portal pedicles are exposed. Both are ligated and divided (A). The RHV is exposed and a thick drainage vein of Sg7 is ligated (B). After removal of Sg7, landmarks including RHV and stumps of P7 are exposed.
Segmentectomies, Sectionectomies and Wedge Resections |
381 |
|
|
Right Anterior Sectionectomy
(Right Paramedian Sectoriectomy,
Anatomical Resection of Segments 5 and 8)
This procedure requires complete division of the main and right portal fissure, and thus the area of parenchymal transection of this procedure is the widest among all anatomical liver resections.
382 |
SECTION 3 |
Liver |
|
|
|
STEP 1 |
Hilar dissection and identification of the anterior section, |
|
transsection along the midplane of the liver
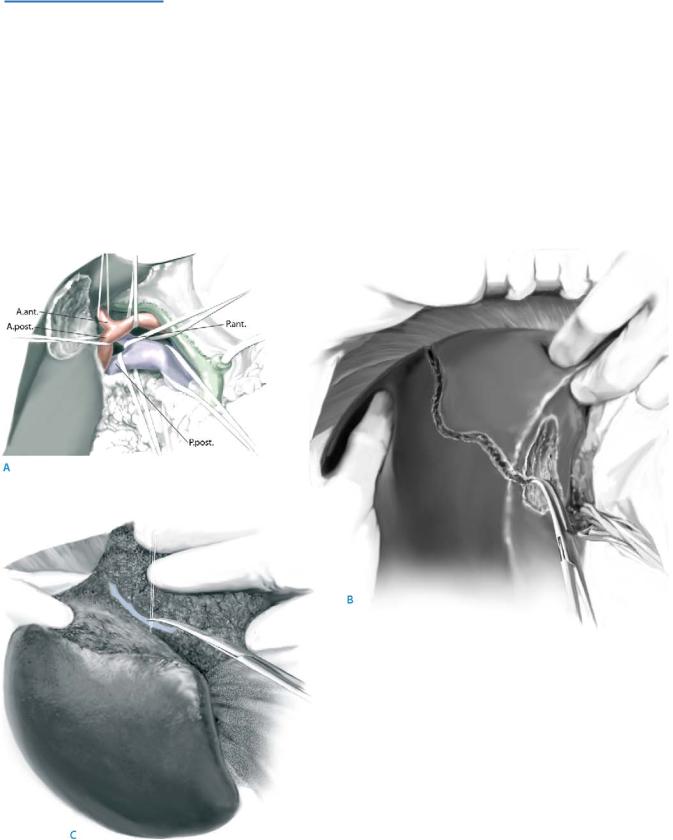
After cholecystectomy, the hepatic hilum is dissected and the right hepatic artery (RHA), the right portal vein (RPV), arterial and portal branches for the anterior and posterior section (Aant, Apost, Pant, Ppost), are isolated (for access to the hilum and preparation of right portal vein/right hepatic artery see also right hemihepatectomy and extended right hemihepatectomy) (A).
After clamping Aant and Pant, the liver surface of the anterior section is discolored and the demarcation lines are marked with electrocautery. This procedure confirms the secti-onal vascular anatomy and Aant and Pant can now be ligated and divided.
Next, under a selective vascular occlusion by soft vascular clamps of the left liver and anterior section, the hepatic parenchymal transection along the midplane of the liver is started (B). The MHV is exposed and tiny tributaries are carefully ligated and divided (C).